
Abstract
Background:
Ectopic thyroid tissue is usually found anywhere along the embryonic descent pathway of the medial thyroid anlage from the tongue to the trachea (Wölfler area). However, ectopic thyroid tissue in the adrenal gland (ETTAG) is not easy to understand on the basis of thyroid embryology; because it is so rare, the possibility of metastasis should first be considered. Here, we describe two cases of ETTAG with pathogenetic implications and review the associated literature.
Patient findings:
Two cases of ETTAG presented as incidental cystic adrenal masses in adult females, one having a congenital hernia of Morgagni. The ETTAG was histologically indistinguishable from normal orthotopic thyroid tissue, and its follicular nature was confirmed by immunohistochemical positivity for thyroglobulin, thyroperoxidase, thyroid transcription factor-1 (TTF-1/Titf-1/Nkx2.1), cytokeratin AE1/AE3, cytokeratin 7, pendrin, human sodium iodide symporter, paired box gene 8, and forkhead box E1 (TTF-2), as well as positivity for the messenger RNA of the thyroglobulin gene by in situ hybridization analysis. No C cells (negativity for calcitonin, chromogranin, and synaptophysin) were present. Neither BRAF nor KRAS mutations were detected with real-time polymerase chain reaction analysis. Further work-up did not show evidence of thyroid malignancy.
Summary:
ETTAG is a rare finding, with only seven cases reported; women are much more frequently affected than men (8:1), and it usually presents in the fifth decade (mean age 54, range 38–67) as a cystic adrenal mass incidentally discovered on abdominal ultrasonography and/or in computed tomography images. ETTAG is composed of normal follicular cells without C cells. The expression of some transcription factors (TTF-1, paired box gene 8, and FOXE1) involved in development and/or migration of the medial thyroid anlage is preserved. Coexistence of a congenital hernia of Morgagni in one patient suggests an overdescent of medial thyroid anlage–derived cells in its pathogenesis.
Conclusion:
Although ETTAG pathogenesis remains unknown, the lack of C cells together with the coexistence of a congenital defect of the anterior diaphragm (hernia of Morgagni) in one of our patients could suggest an overdescent of medial thyroid anlage–derived cells in the origin of this heterotopia.
Introduction
T
This thyroid morphogenetic process is regulated by both cell-autonomous (activated by the thyroid transcription factor-1 [TTF-1/Titf-1/Nkx2.1], forkhead box E1 [FOXE1] [TTF-2], paired box gene 8 [PAX8], and hematopoietically expressed homeobox [HHEX]) and mesoderm-derived (mediated by T-box1 [TBX1] and fibroblast growth factors) mechanisms, acting in concert to promote the growth and survival of progenitor cells (1 –5). Hematopoietically expressed homeobox (HHEX) has an essential role in the maintenance of TTF-1, PAX8, and FOXE1 expression, whereas TTF-1 and PAX8 together regulate proliferation, survival, and differentiation of thyroid follicular cells (follicular pattern of growth), and FOXE1 their migration (3 –5). The expression of both TTF-1 and PAX8 precedes the onset of FOXE1 expression, and the expression of FOXE1 is tightly controlled by PAX8. Although thyrotropin (TSH) is the main growth stimulus of thyroid tissue, and TSH-releasing hormone signaling is required to complete the differentiation program of the follicular cells, the early growth and development of the fetal thyroid appears to be generally independent of TSH (3,4).
The ultimobranchial bodies constitute the lateral thyroid primordia and become apparent during the fourth to fifth week of gestation as stratified endodermal tissue in contact with the embryonic pharyngeal space (1). The ultimobranchial bodies are located in the most caudal pharyngeal pouches and fuse with the medial thyroid primordium to populate the thyroid gland with C cells. Although the orthodox view is that C cells ultimately derive from the neural crest (ectoderm), this assumption of mammalian C cells deriving from the neural crest has been challenged (6 –8).
Here we report two cases of ectopic thyroid tissue in the adrenal gland (ETTAG) with immunohistochemical, in situ hybridization, and molecular studies. Because of the embryological development of the thyroid, this type of ectopia is hard to comprehend. In this article, we also discuss the diagnostic challenges of the ectopic thyroid and its putative histogenesis after reviewing the literature.
Patients
The first patient (case 1), a 38-year-old woman, presented with lower back pain and a medical history significant for endometriosis. Abdominal ultrasound echography revealed a left adrenal 5.2 cm cystic mass and a small 4 mm stone in the left renal pelvis, with associated slight hydronephrosis. Computed tomography (CT) confirmed the adrenal mass, and magnetic resonance imaging showed a well-delimited left adrenal tumor, hypointense with gadolinium, that caudally displaced the left kidney. The aldosterone level was elevated to 687 pg/mL (reference range 30–159 pg/mL). A laparoscopic left adrenalectomy was performed as treatment. Because of the pathological findings, a work-up was carried out to evaluate for thyroid cancer. The results of a thyroid function test, including TSH and thyroxine, and a thyroid and neck ultrasonography (US) examination were normal. The patient was discharged in a clinically asymptomatic condition.
The second patient (case 2), a 59-year-old woman, presented with a symptomatic obstructive process secondary to a hernia of Morgagni containing a gastric volvulus, duodenum, transverse colon, and mesenterium. During the examination, a CT scan of the abdomen showed a concurrent nodular, well-delineated, left adrenal mass measuring 5 cm×5 cm. After surgical treatment of the diaphragmatic hernia, magnetic resonance imaging revealed that the left adrenal mass was hypointense (T2 sequence) and hypovascular (Fig. 1). A fine-needle aspiration biopsy of the adrenal mass was also performed, and the biopsy consisted of a serous fluid and rare histiocytes. The patient underwent an intercostal lumbotomy with a left adrenalectomy. A history of surgery due to cystocele with vaginal vault prolapse was found; however, no family data of thyroid cancer or abnormal results of thyroid tests were detected in the patient. The result of the neck US examination was normal. Four years later, the patient presented a peripheral T-cell lymphoma that was treated by conventional chemotherapy according to current protocols. Despite a partial response, the patient's clinical course was complicated by neutropenic fevers along with opportunistic infections, and she died seven months later.
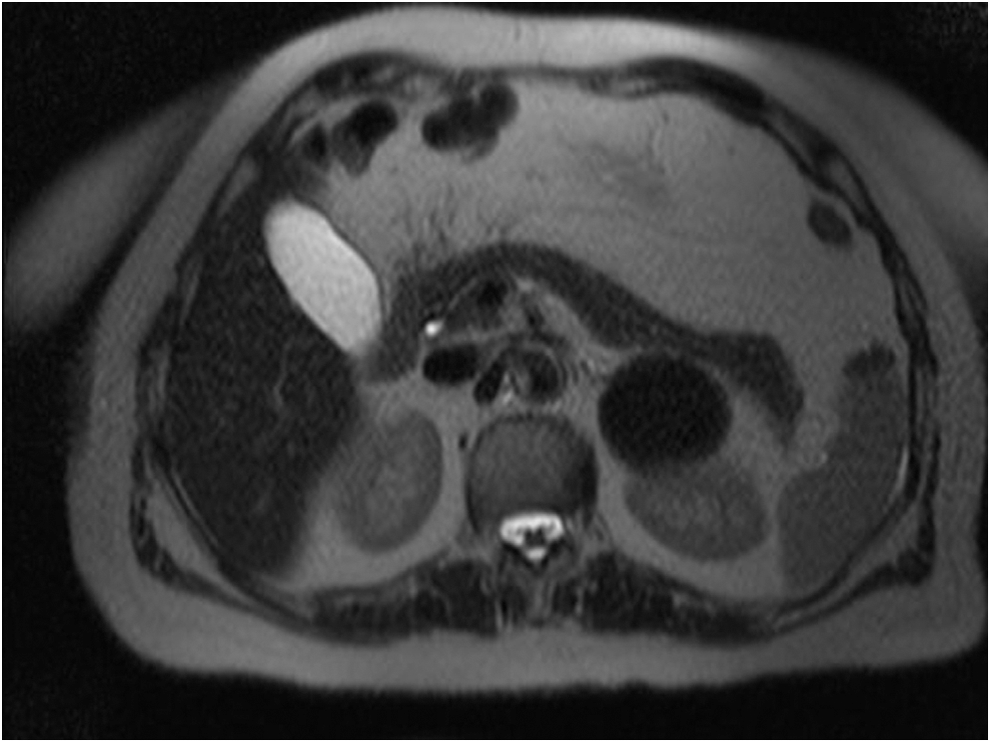
Abdominal magnetic resonance imaging scan from patient 2 showing a well-delineated mass in the left adrenal gland.
Pathological findings
In patient 1, on the gross examination, the adrenalectomy specimen weighed 20 g and measured 7 cm×4 cm×2 cm; after sectioning, it showed a cystic gelatinous content, without necrotic or hemorrhagic areas, measuring 5 cm. In patient 2, the adrenal gland showed a similar appearance with a yellow-walled cystic cavity whose greatest diameter measured 4 cm.
Histologically, the surgical specimen in case 1 showed an adrenal gland with a fibrous capsule containing cystic formations lined by cuboidal to flattened cells with round, dark nuclei. The walls of the cysts revealed normal adrenal tissue intermingled with bland thyroid tissue and fibrosis. Thyroid tissue was distributed as small clusters of follicles or rows of follicles mixed with normal adrenal tissue (Fig. 2). Follicular structures containing colloid ranged in size from small to macrofollicles, sometimes with cystic dilation. Squamoid or hobnail appearance was found only in cells lining some cystic cavities. No particular distribution of thyroid tissue in the outer or inner parts of the adrenal gland was detected. The follicular cells had small, round nuclei with no ground-glass nuclei, pseudoinclusions, nuclear grooves, mitosis, papillae, stromal reaction, psammoma bodies, necrosis, or vascular invasion. One area with a solid nodular adrenocortical pattern consistent with a functioning adenoma was identified. Microscopic sections of the adrenal gland in case 2 showed thyroid tissue with similar features but without adrenocortical adenoma.
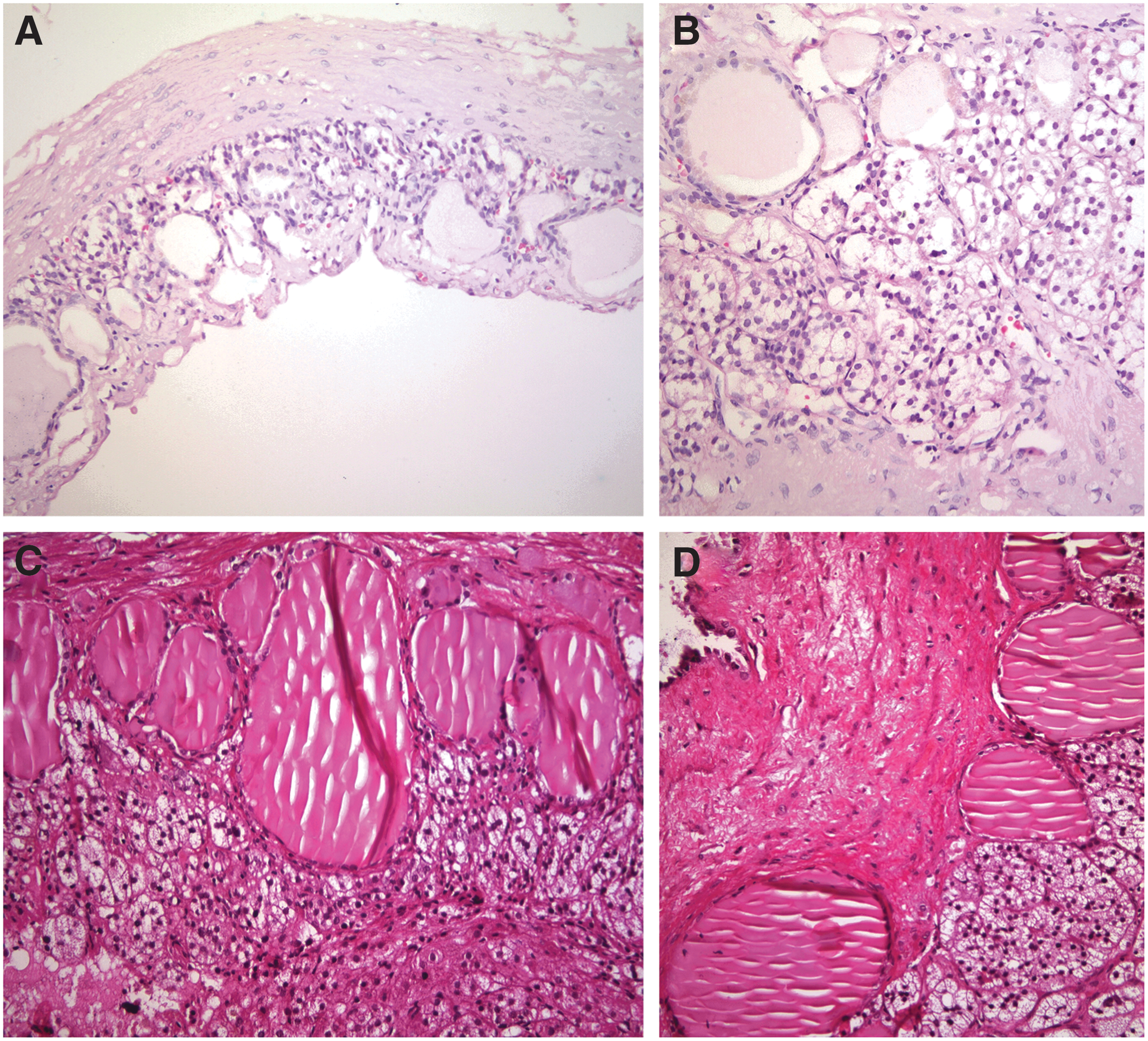
Morphology of ectopic thyroid tissue in the adrenal gland in patient 1
Immunohistochemistry and in situ hybridization analysis
In both cases, an immunohistochemical analysis was performed in formalin-fixed, paraffin-embedded sections using a peroxidase-conjugated labeled dextran polymer (Dako EnVision Peroxidase/DAB; Dako, Glostrup, Denmark) to avoid misinterpreting endogenous biotin or biotin-like activity in the cell cytoplasm or in nuclei as positive staining, with 3,3′-diaminobenzidine as the chromogen and a series of primary antibodies as follows: thyroglobulin (clone DAK-Tg6, dilution 1:20; Dako); thyroperoxidase (MoAb47, dilution 1:50; Dako); calcitonin (polyclonal, ready-to-use; Dako); TTF-1/Titf-1/Nkx2.1 (8G7G3/1, ready-to-use; Dako); cytokeratin (CK) 1–8, 10, 13–16, and 19 (AE1/AE3 ready-to-use; Dako); CK 7 (OV-TL 12/30, ready-to-use; Dako); CK 19 (CRCK108, ready-to-use; Dako); CK 20 (Ks20.8, ready-to-use; Dako); PAX8 (polyclonal, 1:200; Proteintech, Chicago, IL); FOXE1 (TTF-2; polyclonal, 1:200; Abcam, Cambridge, United Kingdom); pendrin (UIRF#01065, 1:500; MBL, Nana-ku Nagoya, Japan); human sodium iodide symporter (hNIS; prediluted; FPSA, Fremont, CA); chomogranin A (polyclonal rabbit, ready-to-use; Dako); synaptophysin (ready-to-use; Dako); galectin-3 (9C4, 1:200; Novocastra, Newcastle upon Tyne, United Kingdom); Hector Battifora mesothelial cell-1 (HBME-1, dilution 1:200; Dako); melan A (A103, ready-to-use; Dako); calretinin (DAK-Calret 1, ready-to-use; Dako); and Ki-67 (MIB-1, ready-to-use; Dako). The results were identical and therefore reported together (Fig. 3). The epithelial cells lining the follicles and cysts were positive for thyroglobulin, thyroperoxidase, TTF-1, CK AE1/AE3, CK 7, PAX8, and FOXE1. Weak immunoreaction for pendrin and hNIS was also detected in these follicular cells. Positivity for CK19, galectin-3, and HBME1 was limited to some squamous cells lining the cystic cavities. No reaction was found for calcitonin, CK20, chromogranin, synaptophysin, or calretinin. Positivity for melan A was observed only in the cytoplasm of adrenocortical cells. The proliferative index (Ki-67) was very low (<0.5%).
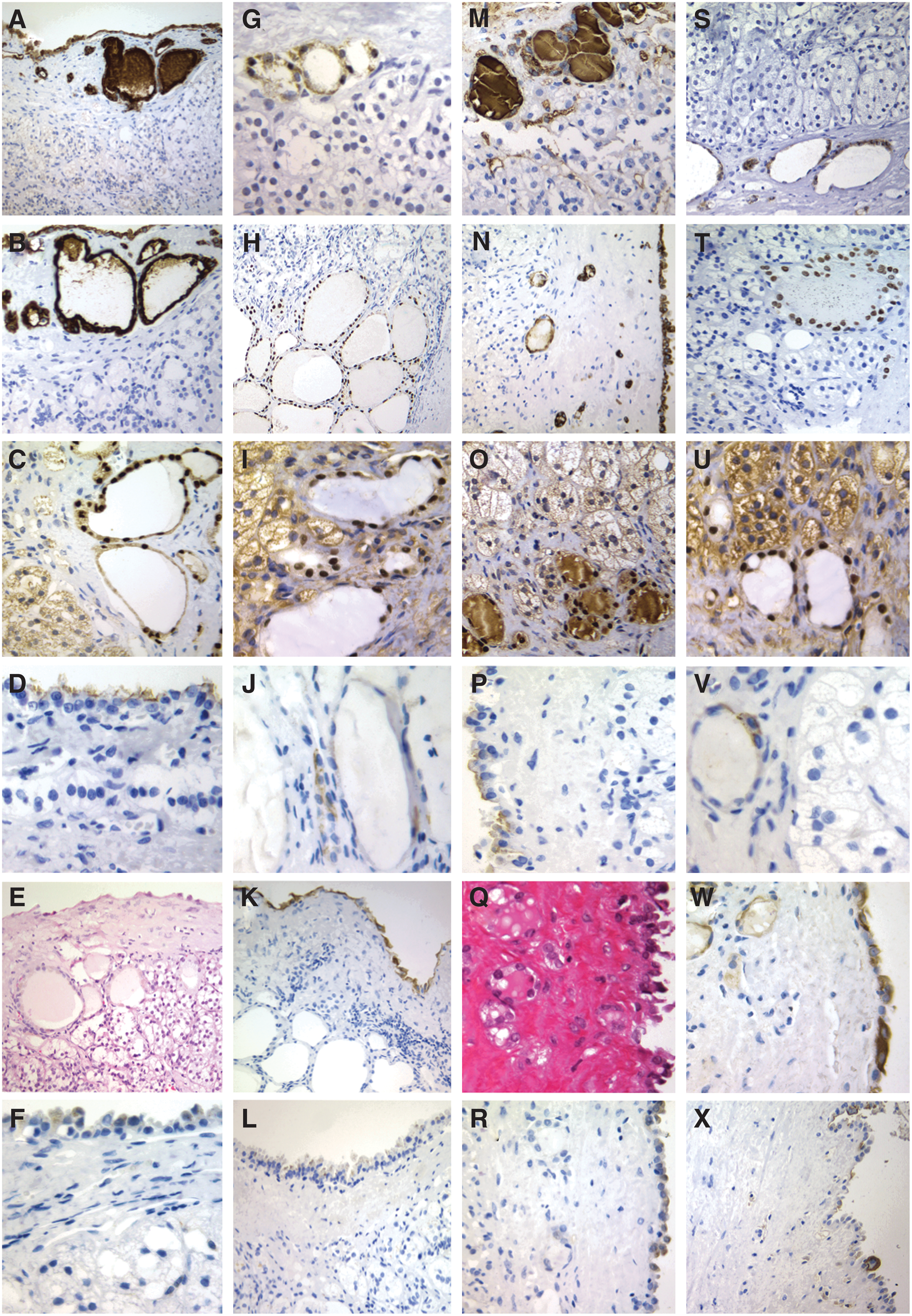
Immunohistochemical and in situ hybridization features of ectopic thyroid tissue in the adrenal gland of patient 1
In situ hybridization for thyroglobulin and calcitonin was also performed on 3-μm-thick paraffin sections using commercial single-stranded DNA probes (CEM-0016, Histosonda Thyroglobulin [Cenbimo, Lugo, Spain] and CEM-0017, Histosonda Calcitonin [Cenbimo]), following the manufacturer's protocol. Positivity for thyroglobulin (Fig. 3G, S) with negativity for calcitonin was confirmed in both cases.
Molecular studies
In molecular analysis, we used a real-time polymerase chain reaction technology system (Cobas 4800 System, v2.0; Roche Diagnostics, Barcelona, Spain) for the detection of the V600E (1799 T>A) BRAF gene mutation (Cobas 4800 BRAF V600 Mutation Test) and the KRAS gene (codons 12, 13, and 61) mutations (Cobas KRAS Mutation Test) in formalin-fixed, paraffin-embedded adrenal and thyroid tissue (after microdissection) from both patients. No mutations, however, were identified in the BRAF or KRAS genes.
Discussion
Here we report two very unusual cases of ETTAG. Ectopic thyroid tissue can be more easily found in the tongue, neck, mediastinum, great vessels, and heart, or anywhere along the embryonic descent pathway of the medial thyroid anlage from the tongue to the trachea (Wölfler area); its microscopic appearance is similar to that of normal thyroid tissue, and this ectopic thyroid tissue is subject to the same diseases that occur in the orthotopic thyroid gland (1,9 –11). Sometimes, thyroid tissue in the neck can be secondary to surgical seeding or accidental trauma (11). In the so-called parasitic nodule (accessory or sequestered thyroid nodule), the anatomic connection with the thyroid gland can be lost or missed by the surgeon, but in these cases, the ectopic tissue resides in the same fascial plane, is unassociated with lymph nodes, and exhibits a similar appearance to that of the thyroid gland (1,11). The possible occurrence of ectopic thyroid tissue in cervical nodes in the presence of an apparently normal thyroid gland, a condition formerly called lateral aberrant thyroid, generally represents the metastasis of a clinically undetected papillary thyroid carcinoma. In the rare cases of truly normal follicles within nodes, the ectopic thyroid tissue is typically scanty, devoid of atypia, and centered in or immediately subjacent to the lymph node capsule of only one or two nodes (1,11).
Ectopic benign thyroid tissue in unifocal, bifocal, and multifocal locations can be found anywhere along the path of descent of the gland, but ectopic thyroid tissue in subdiaphragmatic locations rarely occurs (12). Infradiaphragmatic ectopic thyroid has been reported in the submucosa of the duodenum (13), small intestinal mesentery (14), porta hepatis (12), gallbladder (15,16), pancreas (17), periesplenic area (18), ovary (19,20), fallopian tube (20), inguinal region (21), and vagina (22). To our knowledge, only seven cases of ETTAG have been reported in the literature (23 –28) (Table 1). Women are much more frequently affected than men (8:1), and most cases clinically presented in the fifth decade (mean age 54, range 38–67) as a cystic adrenal mass incidentally discovered on abdominal US or in CT images. The first six cases of ETTAG were reported in the Japanese population (23 –27); however, a seventh case in an African American woman has been more recently published (28), and our two cases have been found in women from Colombia and Spain, respectively.
I, radioactive iodine; CT, computed tomography; F, female; M, male; MRI, magnetic resonance imaging; US, ultrasonography.
The follicular nature of the ETTAG of our two patients was demonstrated by the immunoreactivity for thyroglobulin, thyroperoxidase, pendrin, hNIS, and some thyroid-restricted transcription factors (TTF-1, PAX8, and FOXE1). Additional positivity for thyroglobulin was confirmed at the messenger RNA level by in situ hybridization. Because it is important to rule out metastases from thyroid cancer when thyroid tissue is found in an ectopic location, we demonstrated a very low proliferative index, and no morphological, molecular, or clinical data of thyroid malignancy were detected. With the exception of the limited expression of CK19 in the squamoid follicular cells lining cystic structures, the immunoprofile of CKs was concordant with that of normal thyroid tissue. In addition to CK19, positivity for galectin-3 and HBME-1 was detected only in the same squamoid follicular cells lining the cystic cavities, in less than 95% of all of the follicular cells. Combined expression of CK19, galectin-3, and HBME-1 is found in papillary thyroid carcinomas (11,28,29), but the same phenotype has also been reported in the squamoid nests of Hashimoto thyroiditis, and in solid cell nests of the thyroid (30,31). In our cases, this squamoid appearance and immunophenotype should be interpreted as “ductal metaplasia,” as described by Caillou (32), instead of malignancy. In addition, the absence of BRAF and RAS mutations, two prevalent molecular alterations often found in well-differentiated thyroid cancer (1,11), although not in itself totally excluding malignancy, agrees with the benign nature of this ectopic thyroid tissue and, at the same time, supports the lack of implication of these genes in the pathogenesis of this heterotopia.
Previous explanations for why thyroid tissue can be found in the adrenal gland include metastasis, teratoma, metaplasia, heterotopia (choristoma), and overdescent of the hypoglossal duct remnant (23 –26,28). One case of ETTAG with concomitant incidental (nonrelated) micropapillary thyroid carcinoma was reported (28), and two cases of ETTAG were incidental findings during preoperative abdominal CT for gastric cancer (26,27); metastatic thyroid cancer, however, was excluded in all published cases (23 –28). Although the presence of thyroid tissue in the ovary (as well as fallopian tube) could be easily understood by considering the struma ovarii as a teratoma, this histogenesis for thyroid tissue in the adrenal glands is difficult to accept because the histological examination of the lesion did not show other tissue components typical of teratomas (epidermis, skin appendages, etc.). Because the adrenal cortex originates from the mesodermal layer, the adrenal medulla from the ectodermal germinal layer, and follicular cell from the endoderm, follicular metaplasia from adrenal cells is not probable.
Transcription factors TTF-1, PAX8, and FOXE1, essential for regulating proliferation, survival, differentiation, and/or migration of the medial thyroid primordium (3 –5), were normally expressed in the ectopic thyroid tissue of our two cases. Both our study and the findings of another group (26) confirmed the lack of C cells in the ETTAG; as a consequence, an overdescent of remnants of the medial (endodermal) thyroid anlage can be hypothesized. This idea also seems supported by the coexistence of a diaphragmatic hernia of Morgagni in patient 2, a congenital defect of the anterior diaphragm that could facilitate the anomalous migration of follicular cells. C cells of the thyroid tissue are decreased in patients with congenital diaphragmatic hernia (33); nevertheless, we were unable to find any association between hernia of Morgagni and ectopic thyroid tissue after having searched the PubMed database for articles including the keywords “hernia of Morgagni” published between August 1, 1949, and December 1, 2012.
Conclusions
We report two cases of ETTAG, a rare lesion much more frequent in women than in men that usually presents in the fifth decade as an incidental cyst encountered on US and/or in CT images. ETTAG shows a histological and immunohistochemical profile similar to that of normal thyroid tissue but without C cells. Although the histogenesis of ETTAG is unknown, the lack of C cells fits with a medial thyroid anlage derivation. This, taken together with the coexistence of a diaphragmatic hernia of Morgagni, a congenital defect of the anterior diaphragm found in one of our patients, supports the hypothesis of an overdescent of medial thyroid anlage–derived cells in the histogenesis of this heterotopia.
Footnotes
Acknowledgment
This study was supported by Grant PI12/00749-FEDER from Instituto de Salud Carlos III, Ministry of Economy and Competitiveness, Madrid, Spain.
Author Disclosure Statement
The authors declare that no competing financial interests exist.