
Abstract
Background:
Papillary thyroid cancer is the most common type of thyroid malignancy and has an excellent prognosis. Distant organ metastasis is rare. Bilateral adrenal metastases with iodine uptake has not been described before.
Patient Findings:
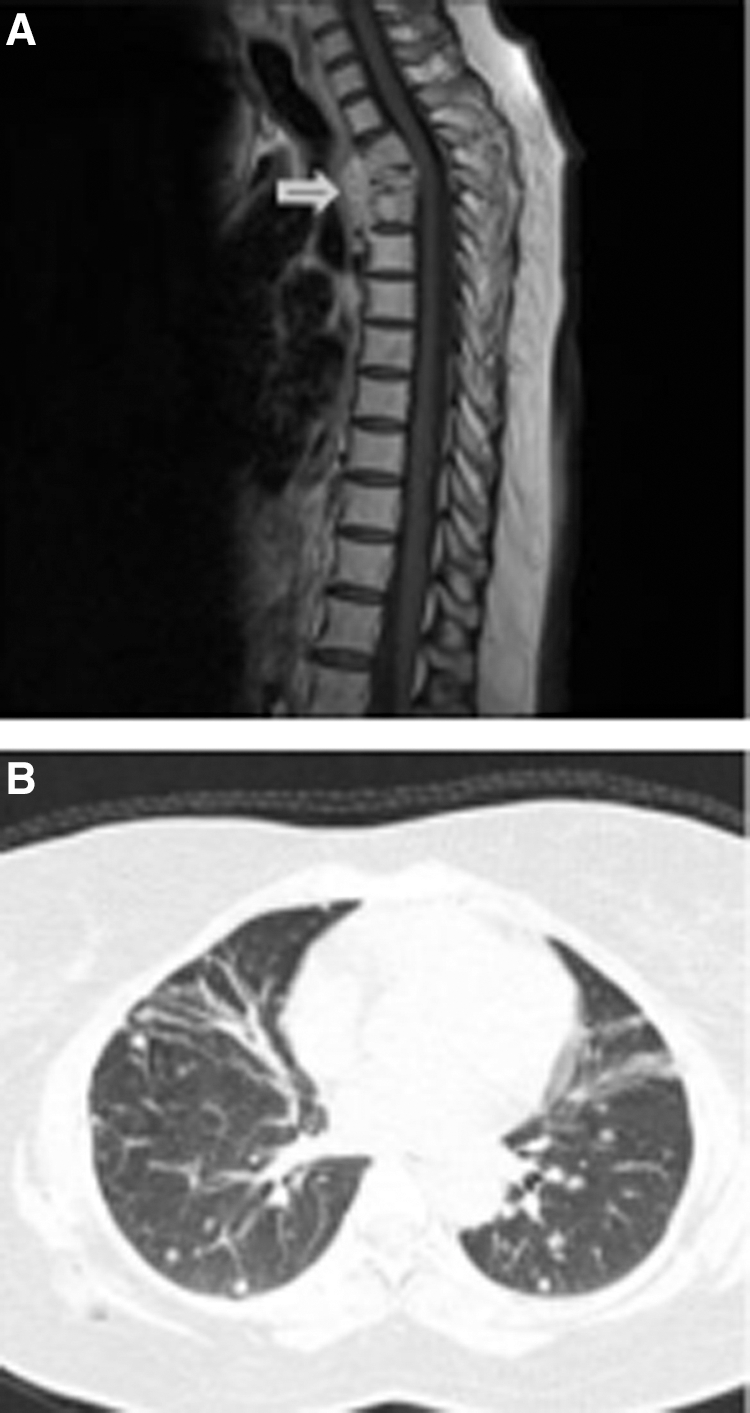
A 47-year-old woman presented for evaluation because of severe right upper arm pain and weakness. Magnetic resonance imaging of the thoracic spine showed a compression fracture at the third thoracic vertebra associated with a soft tissue mass. Computed tomography (CT)-guided biopsy of the mass showed metastatic papillary thyroid carcinoma. Ultrasonography of the neck showed an enlarged right thyroid lobe with cervical lymphadenopathy. A high-resolution CT scan of the chest showed multiple bilateral pulmonary nodules. Treatment included total thyroidectomy and lymph node dissection, external beam radiation to the thoracic spine, and 131I therapy. Initial whole body 131I scintigraphy showed faint uptake in the right upper abdomen, interpreted as a sign of physiologic bowel activity; however, repeat whole body 131I scintigraphy showed increased uptake in both adrenal glands, consistent with metastatic disease. Serial abdominal CT scans showed progressively enlarging bilateral adrenal masses. Despite additional treatment with 131I, the patient's disease progressed at all metastatic sites.
Summary:
This patient had bilateral adrenal metastases from advanced papillary thyroid cancer with distant metastasis to lung and bone at initial presentation and poor response to repeated 131I therapy. Unilateral adrenal metastasis from thyroid cancer has been described previously in six cases; this is the first case report of bilateral adrenal metastases.
Conclusions:
Bilateral adrenal metastasis is rare in papillary thyroid cancer. Elevated abdominal uptake of 131I in a high-risk patient may be a sign of abdominal metastatic disease.
Introduction
P
Metastasis of papillary thyroid cancer to abdominal organs is extremely rare. Whole body scintigraphy with 131I is useful during follow-up to detect persistent disease, especially in high- or intermediate-risk patients. Adrenal uptake of 131I resulting from metastatic thyroid cancer has been described in four patients, including papillary thyroid cancer (two patients) (3,4), an undefined thyroid cancer originating from follicular cells (one patient) (5), and follicular thyroid cancer (one patient) (6). However, a literature review showed no previously reported case of bilateral adrenal uptake in patients with thyroid cancer who had whole body scintigraphy with 131I (7). We treated a patient with aggressive metastatic papillary thyroid cancer who had 131I uptake in both adrenals on 131I scintigraphy and bilateral adrenal lesions on abdominal computed tomography (CT) scans.
Patient
A 47-year-old woman presented for evaluation because of severe right upper arm pain and weakness. Magnetic resonance imaging (MRI) of the thoracic spine showed a compression fracture at the third thoracic vertebra associated with a soft tissue mass (Fig. 1A). A CT-guided biopsy of the mass showed metastatic papillary thyroid carcinoma. Ultrasonography of the neck showed an enlarged right thyroid lobe with cervical lymphadenopathy. A high resolution CT scan of the chest showed multiple bilateral pulmonary nodules (Fig. 1B). A whole body bone scintigraphy with technetium Tc 99m methylene diphosphonate showed only uptake at the third thoracic vertebra.
A 47-year-old woman who had metastatic papillary thyroid cancer. Initial treatment included thyroidectomy, external beam radiation therapy to the thoracic spine, and 131I.
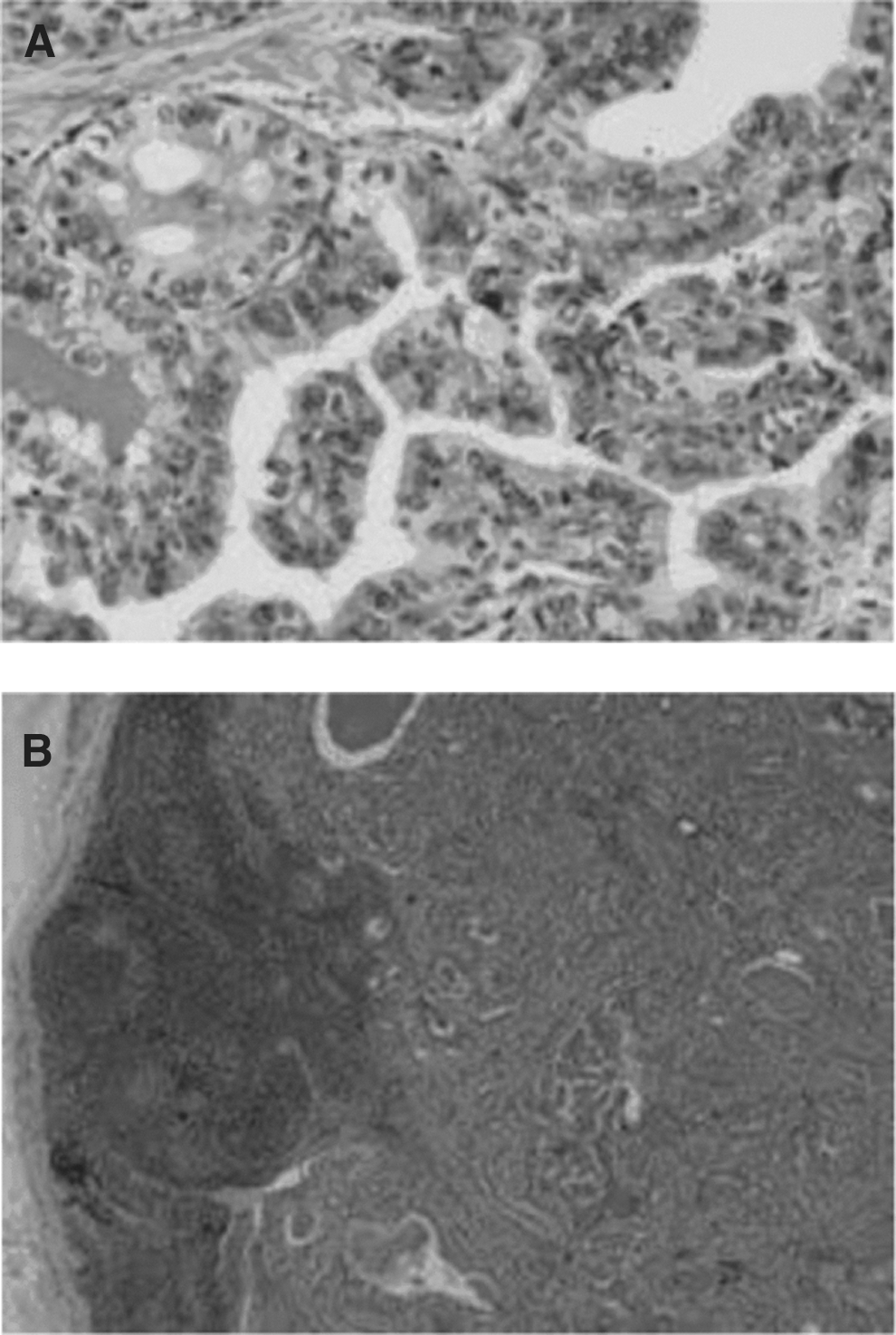
The patient was treated with total thyroidectomy and lymph node dissection. Histologic evaluation of the thyroid tumor (3 cm long×5 cm wide) showed a classic variant of papillary thyroid carcinoma of the right thyroid lobe (Fig. 2A). There was no tall cell, columnar, or diffuse sclerosing variant to suggest aggressive tumor biology. There was lymphovascular and capsular invasion, and four lymph nodes contained metastatic papillary thyroid carcinoma (Fig. 2B).
The lesion at the third thoracic vertebra was not operable and was treated with external beam radiation therapy from the first to fourth thoracic vertebrae. After withdrawal of thyroid hormone for 4 weeks, serum thyrotropin (TSH) was 51 mU/L, the stimulated thyroglobulin was 1426 ng/mL (Table 1). The patient was treated with 131I (9.6 GBq). The posttherapy whole-body scintigraphy showed radioactive iodine uptake in the thyroid bed, the third thoracic vertebra, and right pulmonary nodules (Fig. 3A). An abdominal CT scan showed normal adrenal glands (Fig. 4A). The patient was treated with a suppressive dose of levothyroxine (125 μg once daily).
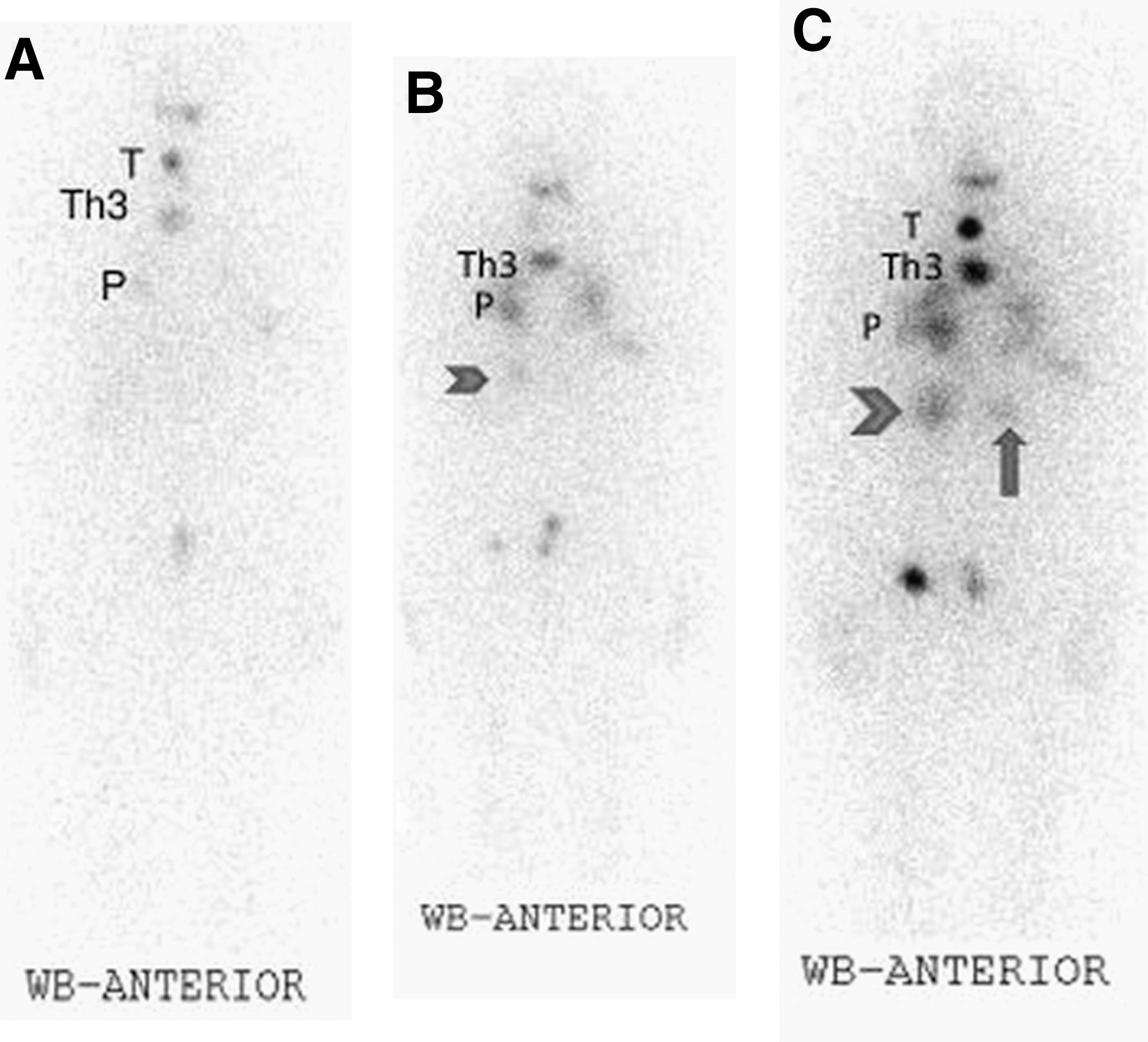
Serial whole-body scans after treatment with 131I.

Serial CT scans of the abdomen.
RAI, radioactive iodine; T4, thyroxine; TSH, thyrotropin; Tg, thyroglobulin.
The patient was followed for 3 years and was treated with three additional therapeutic doses of 131I (9.2 GBq per treatment); the doses were limited to 9.2 GBq to minimize the risk of pulmonary toxicity. All therapies were obtained after withdrawal of levothyroxine for 4 weeks. After thyroid hormone withdrawal, the TSH levels ranged from 51 to 97 mU/L and the thyroxine (T4) levels were between 2 and 5 pmol/L (reference range 22–24 pmol/L; Table 1). Whole-body iodine scans were performed 10 days post 131I therapy. After the third 131I dose, the whole-body scintigraphy showed increased uptake in both lungs and the third thoracic vertebra; faint uptake was noted in the right upper abdomen and was interpreted as a sign of physiologic bowel activity (Fig. 3B). Abdominal CT scanning showed a right adrenal lesion (Fig. 4B). After the fourth 131I dose, the whole-body scan showed increased uptake in both adrenal glands, with greater intensity in the right compared to the left adrenal gland; there was increased uptake in the thyroid, the third thoracic vertebra, and both lungs (Fig. 3C). A repeat abdominal CT scan showed bilateral adrenal lesions (Fig. 4C). The left adrenal lesion (2 cm×3 cm) was enhanced and solid, and the right adrenal lesion (5 cm×6 cm) was cystic (8 Hounsfield units); both left and right adrenal glands had enlarged since the previous CT scan, consistent with bilateral adrenal metastasis.
Tissue biopsy of the adrenal masses was not obtained. Despite additional radioactive treatment and full TSH suppression (TSH 0.01 mU/L), the patient's disease progressed at all metastatic sites, with persistently elevated thyroglobulin levels; the stimulated thyroglobulin at the last radioactive iodine therapy was more than 5000 ng/mL (Table 1).
Discussion
This patient had bilateral adrenal metastases from papillary thyroid cancer. Bilateral adrenal metastases from papillary thyroid cancer are rare. Adrenal metastasis secondary to thyroid cancer was described previously in six patients, including four patients who had increased iodine uptake on whole body iodine scintigraphy (3 –6), one patient who had metastasis noted on a fluoro-deoxyglucose positron emission tomography (PET) scan (8), and one patient who had metastasis noted after adrenalectomy (9).
Optimal treatment of papillary thyroid cancer includes thyroidectomy, adjuvant 131I ablation therapy, and long-term TSH suppression with levothyroxine. Lifelong follow-up is needed and may include neck ultrasonography, measurement of stimulated and nonstimulated thyroglobulin levels, whole body scintigraphy with 131I, CT, MRI, and fluoro-deoxyglucose PET scans.
In whole-body 131I scintigraphy, iodine uptake in the abdomen is a common finding and may represent normal bowel activity. However, in a high-risk patient, iodine uptake may be an early sign of metastatic disease, as in the present patient. Delayed views and correlation with anatomic studies such as CT, MRI, single-photon emission CT, or PET-CT may help distinguishing normal physiologic iodine uptake from adrenal metastasis. The prognosis of patients with papillary thyroid cancer and distant metastasis is worse in older patients (age >45 years), multiple organ involvement, higher tumor stages, aggressive histologies, and a loss of the ability to concentrate 131I (10).
In summary, the present patient with advanced papillary thyroid cancer had the unusual finding of bilateral, rapidly growing adrenal metastases, confirmed with bilateral adrenal 131I uptake on whole-body scintigraphy and abdominal CT scans. The patient had a poor response to repeated radioactive iodine therapy after thyroidectomy. Elevated abdominal uptake of 131I in a high-risk patient may be an early sign of abdominal metastatic disease.
Footnotes
Acknowledgments
The author expresses her gratitude to her husband Dr. Iskander Algithmi for his outstanding support.
Disclosure Statement
The author has no conflict of interest.