
Abstract
Background:
Hospital-based studies may be hampered by referral bias. We investigated how the phenomenon may influence studies of hyperthyroid patients.
Methods:
By means of a computer-based linkage to the laboratory database and subsequent detailed evaluation of subjects with abnormal test results, we prospectively identified all 1148 patients diagnosed with overt hyperthyroidism in a four-year period in and around Aalborg City, Denmark. Each patient was classified according to nosological type of hyperthyroidism. We studied the referral pattern of patients to local hospital units, and analyzed how referral depended on subtype of disease, sex, age, and degree of biochemical hyperthyroidism.
Results:
In a 4-year period, 1032 hyperthyroid patients were diagnosed at primary care offices, and 435 of these (42.2%) were referred to specialized units, 92 patients had hyperthyroidism diagnosed in other hospital departments (referral: 43, 46.7%), and 24 patients had hyperthyroidism diagnosed at the specialized unit after referral for other diseases. Patients suffering from Graves' disease (GD; n=474, median age=65.8 years) were referred more often (odds ratio=1.7 [95% confidence interval 1.3–2.2]) than those diagnosed with multinodular toxic goiter (MNTG; n=525, median age=74.6 years). Higher age was associated with less referral of patients suffering from MNTG (referred vs. nonreferred patients, 64.0 vs. 77.4 years, p<0.001) and GD (43.9 vs. 56.4 years, p<0.001), whereas GD patients referred to a hospital had more severe biochemical hyperthyroidism (serum total triiodothyronine, 4.86 vs. 3.79 nmol/L; serum total thyroxine, 204 vs. 180 nmol/L; both p<0.001). Findings were confirmed in multivariate models reporting age as a significant predictor for referral in both GD and MNTG patients (both p<0.001). Among referred hyperthyroid patients (all combined), those aged up to 40 years (referral rate, 66.8%) were represented 11.6 (6.6–20.6) times more often than those aged 80 years and above (referral rate, 14.8%).
Conclusions:
Hyperthyroid patients referred to a specialized hospital unit were younger (GD+MNTG) and had more severe biochemical hyperthyroidism (GD) compared to nonreferred patients. Thus, referral bias may influence hospital-based studies of hyperthyroid patients, and may hamper external generalization of such studies. Whether the referral bias of hyperthyroid patients in Denmark can be generalized to other countries or cultures remains unknown.
Introduction
H
In a previous systematic PubMed search presented in a previous Danish investigation on iodine intake and thyroid diseases (DanThyr) article dealing with referral of hypothyroid patients (2), we explored various predictors for referral. We reported that studies may be distorted by referral bias, due to disparity between referred and nonreferred patients with regard to sex, age at disease onset, ethnicity, severity of disease, nosological type of disease, presence of concomitant disease, income, state of education, and marital status.
Based on the DanThyr study of patients newly diagnosed with thyroid disease (3), we previously reported that hypothyroid patients who were referred to specialized endocrine units were 16 years younger than those remaining in primary care clinics. The aim of the present study was to investigate referral patterns of patients suffering from different nosological types of hyperthyroidism to hospitals.
Materials and Methods
The present study was a part of DanThyr (3). We monitored all thyroid function tests requested by hospital doctors and general practitioners in and around the city of Aalborg in the period March 1997 to December 2000. A register was linked to the LABKA laboratory database containing results of all thyroid function tests requested by general practitioners and hospital doctors in the study area (4). Thus, a well-defined cohort of inhabitants in and around the city of Aalborg was monitored for 46 months (1,192,558 person-years of observation). Results of thyroid function tests performed were extracted to our research database on a weekly basis (5). Subjects with a thyroid function test suggesting overt hyperthyroidism (low thyrotropin combined with an elevated total triiodothyronine [T3] or thyroxine [T4]) were classified as possible hyperthyroid cases, and we contacted the doctor who requested the blood test and asked if this was a known or a new case of overt thyroid dysfunction. Hospital records were also scrutinized in order to verify incident cases. All incident cases verified as suffering from overt hyperthyroidism (n=1148) were individually scrutinized and classified into nosological types of hyperthyroidism according to well-defined criteria (6). We have previously described which biochemical criteria were set for diagnosing overt hyperthyroidism, and how the diagnosis was confirmed (6). We also outlined in detail how we used scintigraphic investigation, thyroid hormone receptor antibody measurement, and a detailed patient history in order to subclassify each patient into a specific type of hyperthyroidism: Graves' disease (GD; median age=50.7 years), n=474; multinodular toxic goiter (MNTG; median age=74.6 years), n=525; solitary toxic adenoma (median age=65.8 years), n=73; iatrogenic hyperthyroidism (n=32) due to amiodarone, radioactive iodine, lithium, or after surgical removal of parathyroid-hormone producing adenoma; thyroiditis (n=44) due to postpartum thyroid dysfunction, or subacute thyroiditis.
The Danish healthcare system
More than 99% of the Danish population is registered with a private general practitioner. General practitioners are the main gate for patients toward the healthcare system. They often take care of biochemical thyroid problems, as most patients suffering from GD are treated with antithyroid drugs as is also the case for many old patients suffering from MNTG. However, some patients are referred by general practitioners to hospitals for a second opinion or specialized treatment. Within the study area, no private specialty clinics are available, and patients may only be referred to public hospital care. All visits are free of charge in Denmark.
Classification of “referred” and “nonreferred” patients
We searched for referral pattern by seeking whether patients were referred to the local specialized endocrine unit, Department of Endocrinology, Aalborg University Hospital (DEAH). DEAH is the only specialty department in the area, to which hyperthyroid patients are referred. Information on referral was drawn from the electronic patient administrative system, in which all hospital in- and outpatients are registered. We evaluated every patient individually, and searched for hospitalizations in relation to the point of time at which hyperthyroidism was diagnosed. Only hospitalizations relevant for the care of hyperthyroidism were regarded as referral to the hospital. In addition, outpatients offered a DEAH visit were also regarded as referred patients. Thus, patients were allocated into one of five groups: I. Hyperthyroidism diagnosed by primary care physician with subsequent referral to DEAH. II. Hyperthyroidism diagnosed by primary care physician with no referral to DEAH. III. Hyperthyroidism diagnosed by secondary care physician (other departments at Aalborg University Hospital or other regional hospitals) with a subsequent referral to DEAH. IV. Hyperthyroidism diagnosed by secondary care physician with no referral to DEAH. V. Hyperthyroidism diagnosed at DEAH.
Groups I, III, and V were combined as referred patients, which is the patient category included in most hospital-based studies of patients referred to a specialty department. Subjects belonging to groups II and IV were classified as nonreferred patients.
Patient characteristics
For all patients, we collected information on age at diagnosis, sex, and serum levels of thyroid hormones (T3 and T4). Assays for total T4 and total T3 have been described previously (7,8).
Calendar year at diagnosis was recorded and used in statistical analyses to evaluate if implementation of the DanThyr program had altered the referral pattern from primary to secondary care.
Statistics
We used Statistical Package for Social Sciences (Chicago, IL) for calculation of means and medians of various patient characteristics. To compare referred with nonreferred patients, we tested the distribution of patient characteristics in univariate models (dichotomized variables: χ 2-test; continuous non-Gaussian distributed variables: Mann–Whitney U-test; test for trend: Mantel–Haenszel linear-by-linear association χ 2-test). A multivariate logistic regression model was used to identify which patient characteristics were associated with referral state. Calculations were performed for the two main types of hyperthyroidism, MNTG and GD. In both models, referral state was the dependent variable. The explanatory variables were age + serum T3 + year at diagnosis in model A, and age + serum T4 + year at diagnosis in model B. Variables with p-values<5% were regarded as significant predictors of referral.
Ethics approval
This study was approved by Regional Ethics Committee in Aalborg and Copenhagen. Permission for the Registry was obtained from the Danish Data Protection Agency.
Results
In Aalborg and surrounding municipals, 89.0% (1032/1148) of patients with hyperthyroidism were diagnosed by primary care physicians as depicted in Figure 1. Of these patients, 42.2% were referred to the DEAH for a second opinion and/or further treatment for hyperthyroidism. A similar patient rate was referred to DEAH (43/92, 46.7%) from other hospital departments, at which 8.0% of hyperthyroid cases had been diagnosed. Only a small part of the patients had their hyperthyroid state diagnosed at DEAH.

Flowchart depicting which institution requested thyroid function tests leading to the diagnosis of hyperthyroidism and subsequent referral to the Endocrine Department for specialist assessment.
Characteristics of referred and nonreferred hyperthyroid patients were compared in an univariate model (Table 1). Patients referred to the specialized hospital unit were on average 15 years younger and had more severe hyperthyroidism at diagnosis (higher serum total T4 and total T3). Sex did not affect the probability for subsequent referral. Further, no trend in referral rate was observed during the four-year study period from March 1997 to December 2000.
Data are number of patients (percent of all), mean, or median (25%;75% percentiles) of serum concentration.
Patients who were referred to Department of Endocrinology, Aalborg Hospital, from general practitioners or other hospital departments.
Of 502 hyperthyroid patients, 487 had T3 measured (15 had not T3 measured, and hyperthyroidism was based on low thyrotropin and high T4).
Of 646 hyperthyroid patients, 640 had T3 measured (6 patients had not had T3 measured).
The study period only included the first nine months in year 1997.
Mantel–Haenszel linear-by-linear association χ 2 trend test.
ref., referred patients; nonref., nonreferred patients; T3, triiodothyronine; T4, thyroxine.
In hyperthyroidism (all groups combined), 43.7% (502/1148) of patients were referred to DEAH (Table 2). A higher referral rate was observed among those diagnosed with GD (odds ratio [OR]=1.35 [95% confidence interval (CI) 1.06–1.73]) compared to the remaining hyperthyroid patients, and among patients harboring solitary toxic adenoma (OR=2.04 [CI 1.23–3.41]), and the iatrogenic types (OR=2.90 [CI 1.30–6.66]).
OR for referral to Department of Endocrinology, Aalborg Hospital (each group is compared to all other groups combined).
Hyperthyroidism caused by amiodarone (n=13), radioactive iodine treatment (n=11), lithium (7), and thyroid manipulation during surgery for parathyroid hormone–producing adenoma (n=1).
Postpartum thyroid dysfunction (n=23) and subacute thyroiditis (n=21).
CI, 95% confidence interval; OR, odds ratio.
We further analyzed the effect of age and the degree of biochemical hyperthyroidism on the referral pattern in two multivariate logistic regression models (Table 3). Age was a significant predictor for referral in both MNTG (p<0.001) and GD (p<0.001). Serum levels of T3 and T4 were predictors only for referral in Graves' hyperthyroidism. Sex and calendar year at diagnosis did not predict later referral to specialized endocrine unit.
Comparisons were made using a multivariate logistic model, with referral as the independent variable. Independent (=explanatory) variables were obtained at diagnosis (before treatment). Values represent odds ratios for being referred to specialized hospital units.
Values <1 indicate higher referral of women, >1 higher referral of men.
Values <1 indicate lower referral with progressively higher age.
Values <1 indicate higher referral with progressively lower T3 or T4, >1 higher referral with progressively higher T3 or T4.
Values <1 indicate higher referral in the beginning of the study period 1997–2000, >1 higher referral at study end.
p<0.05, ** p<0.001.
The profound effect of age on the referral pattern in hyperthyroidism is depicted in Figure 2. Among referred patients, those aged up to 40 years (referral rate, 66.8%) were represented 11.6 (6.6–20.6) times more often than those aged 80 years and above (referral rate, 14.8%). We found no difference in age-specific referral fractions of patients diagnosed with MNTG and GD. However, due to different ages at onset, more GD than MNTG patients were referred for specialist opinion.
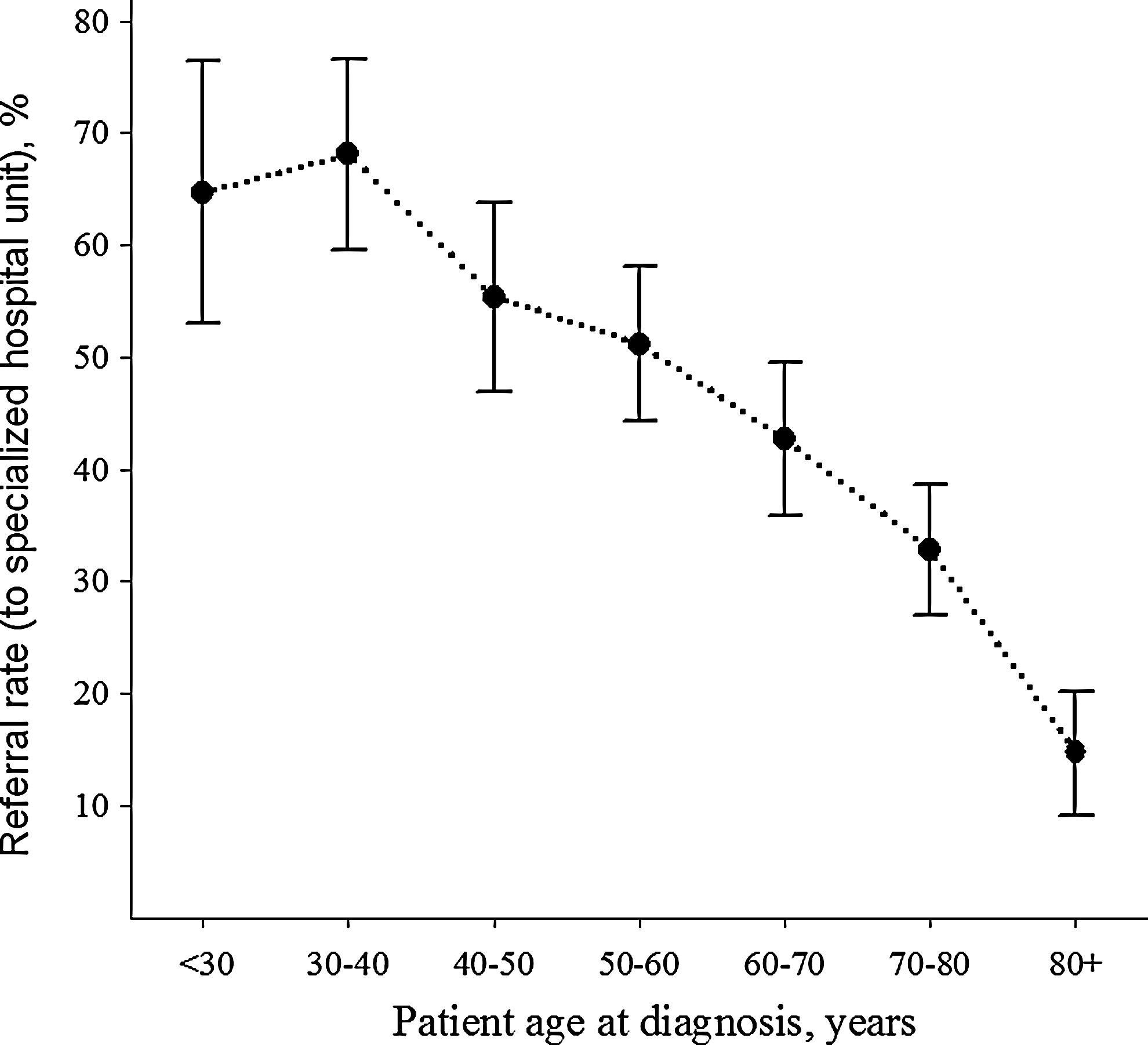
Referral rates (including 95% confidence interval) of hyperthyroid patients (all types combined) according to age at diagnosis. Referral rates stratified on age <30, 30–39.9, 40–49.9, 50–59.9, 60–69.9, 70–79.9, and ≥80 (in years) were 64.7, 68.1, 55.4, 51.2, 42.7, 32.8, and 17.4 (in %), respectively.
Discussion
The present study is the first investigating the effect of various predictors, including age on hospital referral of patients newly diagnosed with hyperthyroidism. We show that several factors influenced the likelihood of referral.
Predictors for referral
Progressively higher age was associated with a lower frequency of referral to a specialized endocrine unit. This is in accordance with other studies of various diseases (9 –30) reporting the same age-dependent referral pattern. We only identified a few studies reporting higher referral rate among the elderly diabetes patients (31,32).
In GD, referred patients had higher serum T4 and T3 levels than the group of GD patients not referred to a hospital. Whether it is the degree of biochemical abnormality per se or the symptoms caused by high levels of T4 and T3, which led to referral of GD patients, remains an unsolved question. Men and women newly diagnosed with hyperthyroidism were referred at equal frequency.
Our study shows an unaltered referral pattern over time, which is in line with the scheduled implementation of the DanThyr program (3). Thus, no interference was introduced, and the study represents how thyroid patients are dealt with in routine clinical care.
Most studies worldwide have described a predominance of GD compared to multinodular toxic goiter as reason for referral. In the present study, this was also true for the fraction of patients referred to hospitals (GD vs. MNTG, 45.4% vs. 37.5%). However, among those not referred for a second opinion and treatment, MNTG was the most common type of hyperthyroidism (MNTG vs. GD, 52.2% vs. 38.1%). Thus, differences in incidence rates of subtypes of hyperthyroidism between studies may, to some degree, reflect different referral pattern, although differences in iodine intake level have a major impact (33). At the time of the study, iodine intake in Aalborg was moderately low, leading to a high incidence of MNTG (6).
Perspectives
Feinstein (34) stated that a necessary condition for recruiting patients to research studies is that “patients will appear at the particular setting in which research is being conducted.” In other words, referral pattern may influence whether patients recruited are representative for the entire cohort of patients diagnosed in society. We have demonstrated that younger patients would be over-represented if hyperthyroid patients were only selected and studied at hospitals. Similar findings have been reported in studies of patients suffering from various types of cancer (13,15,16,19,22,25), cardiac disease (10,23,24), Alzheimer's dementia (14), Parkinson's disease (11), nonautoimmune diabetes mellitus (30), transient ischemic attacks (20), infective endocarditis (21), multiple sclerosis (26), female urinary incontinence (17), children suffering from mental disorders (18), oncology patients undergoing psychiatric treatment (12), and in post mortem referral for autopsy (9). Thus, referral bias may hamper a wide range of studies.
Study strengths and limitations
This study provides novel information on referral pattern and bias in and around a city with a total of 311,102 inhabitants representative for the Danish population with regard to sex and age distribution (35). The skills of general practitioners, the availability for a quick second opinion as hospital outpatients, and the patients' wishes and demands for a second opinion may differ between geographical areas in Denmark, as well as in the rest of the world. Thus, the referral pattern in other geographical areas in Denmark may be different. However, we have no such data available.
Each medical record was scrutinized in order to select precisely those patients who, as in- or outpatients, were referred for a second opinion or treatment of newly diagnosed hyperthyroidism. This is in contrast to ordinary register studies, which only rely on the discharge diagnoses and not on the context of each medical record.
A variety of patient characteristics not included in our data analyses such as socioeconomic status, marital status, and comorbidity may predict later referral to a hospital. Unfortunately, we only had available data on sex, age at diagnosis, subtype of disease, calendar year, and thyroid hormone levels.
We have no data to evaluate whether the proportion of patients referred to a specialty department is at a reasonable level. However, in our area elderly patients suffering from MNTG are mostly treated medically, which may explain the low rate of referral among the elderly. In addition, GD patients consulting physicians in the study area are often treated medically and not by radioactive iodine, which is the preferred treatment in other parts of the world.
We considered how to classify patients who had hyperthyroidism diagnosed at DEAH (group V). As most of these patients had been referred for thyroid problems such as goiter or subclinical hyperthyroidism, and then during follow-up developed hyperthyroidism, they were classified as referred patients.
Conclusions
Patients who were diagnosed with hyperthyroidism and subsequently referred to hospitals differed from those not referred. Referred patients suffering from MNTG or GD were younger, and Graves' patients referred to a specialized endocrine hospital unit exhibited a higher state of biochemical hyperthyroidism. Thus, hospital-based studies may not represent the entire cohort of patients with new hyperthyroidism, and they may not reflect the clinical problems encountered in general practice in all detail. It remains unknown if this referral bias of hyperthyroid patients can be generalized to other countries or cultures.
Footnotes
Acknowledgments
This study was part of DanThyr, and it was supported by the following grants: IMK General Foundation; The Danish Council for Independent Research; Ministry of Food, Agriculture and Fisheries; the Danish Agency for Science, Technology and Innovation, Institute for Clinical Medicine, University of Aarhus; and Aase og Ejnar Danielsens Foundation. We are indebted to the general practitioners in Northern Jutland and to clinical chemical laboratory at Aalborg Hospital for their helpful collaboration in identifying patients.
Author Disclosure Statement
The authors declare that they have nothing to disclose.