
Abstract
Background:
Some studies have shown a higher incidence of thyroid cancer in patients with insurance coverage and higher socioeconomic status (SES), and a higher thyroid cancer stage in patients with lower SES, suggesting SES-related health disparity in thyroid cancer. However, it is not known if the same is evident under a universal healthcare system such as that in Canada.
Methods:
We used data from the Canadian Thyroid Cancer Consortium, a large thyroid cancer registry that collects data from two major thyroid cancer referral centers (London, Ontario, and Halifax, Nova Scotia). We included patients who presented with thyroid cancer between 1998 and 2011. We determined age at presentation, sex, and thyroid cancer status using the American Joint Committee on Cancer (AJCC) staging criteria. Individuals' postal codes were used to retrieve data from the Canadian census for the years 1996, 2001, and 2006 to approximate household income. Ordered logistic regression was used to determine odds ratios of presenting with more advanced stage thyroid cancer as they relate to income, age, and sex.
Results:
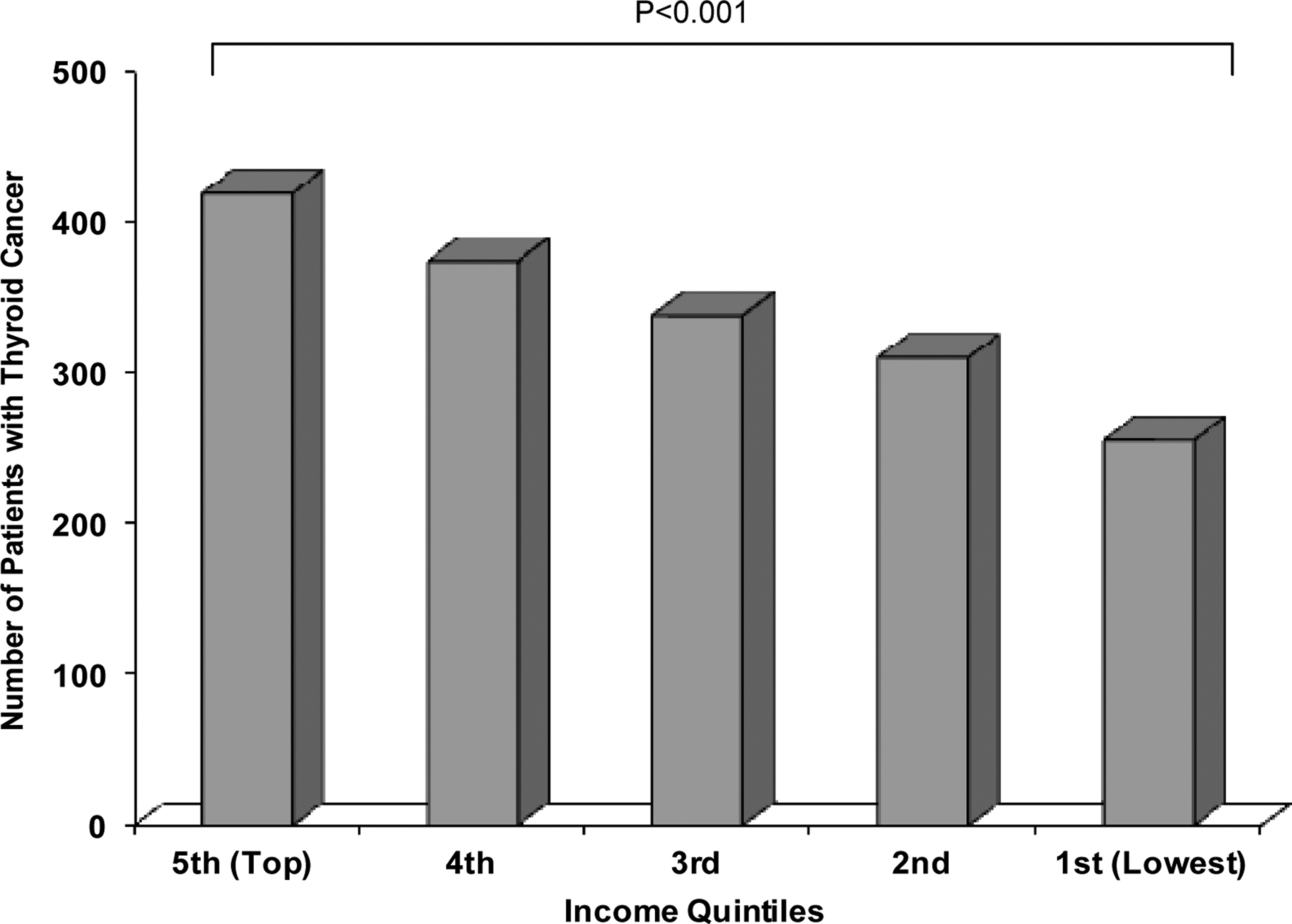
We included 1701 patients: 1334 cases from London and 367 from Halifax. Thyroid cancer was diagnosed more frequently in the higher SES groups (p<0.001). Compared to patients in the top income quintile, patients in the lowest and second-lowest income quintiles had significantly higher odds of having more advanced stage thyroid cancer at presentation (OR 1.58, p=0.002; 1.37, p=0.024 respectively).
Conclusions:
Our study suggests that, similar to countries that lack a universal healthcare system, health disparity in thyroid cancer also exists in Canada. It appears that while thyroid cancers were diagnosed more frequently in Canadian patients of higher SES, Canadian patients in the lower SES groups had more advanced stage thyroid cancer at presentation.
Introduction
T
Some studies found that while incidence of thyroid cancer was rising, so was the discovery of small-size tumors. This suggests a potential effect of increased diagnostic surveillance (2,4). As the access to diagnostic tests may vary between patient groups, the diagnosis of thyroid cancer and the stage at presentation could be affected by variability in access to healthcare. A retrospective chart review from two hospitals in New York, NY, found that patients presenting to a public hospital, most of whom did not have private insurance, were more likely diagnosed with advanced-stage thyroid cancer than those presenting to a university teaching hospital (5). A small eight-year retrospective chart review of 292 patients from Texas found that individuals with low income and less prestigious jobs were more likely to present with high-risk thyroid cancer (6). Furthermore, a study from New Jersey showed that patients of high SES had the highest incidence of thyroid cancer (7). Overall, these studies suggest there is a relationship between SES and thyroid cancer.
All these studies were performed in U.S.-based populations, and health disparity in cancer has indeed been documented in several studies originating from the United States (8,9). This observation has often been attributed to the multi-payer, mostly privately funded healthcare system in the United States that results in a high number of low-income individuals having limited access to healthcare. Canada and the United States are ethnically, culturally, and economically similar, but Canada provides healthcare through a single-payer, government-funded system. The Canadian healthcare system provides universal coverage for all healthcare services that are considered medically necessary, so that individuals are provided care on the basis of need rather than the ability to pay. To our knowledge, the relationship between SES and thyroid cancer has not been studied within a government-funded system such as that in Canada. Therefore, we investigated the relationship between SES and thyroid cancer stage at presentation in Canada, using data from a large Canadian thyroid cancer registry.
Methods
Patients
Patients were recruited from the thyroid cancer clinics at two tertiary Canadian centers that participate in a thyroid cancer study registry known as the Canadian Thyroid Cancer Consortium (CTCC). Six Canadian centers participate in this registry, but for the present study, only centers that have enrolled more than 200 patients were included. Thus, the two centers for the present study were the London Health Sciences Centre (LHSC) in London, Ontario, and the Queen Elizabeth II Health Sciences Centre (QEII) in Halifax, Nova Scotia. LHSC is the major referral center for patients residing in Southwestern Ontario, whereas QEII is the major referral center for patients in Nova Scotia. All thyroid cancer patients attending these clinics during the study periods were invited to enroll in the CTCC. More than 95% of invited patients provided written informed consent. The study was approved by research ethics boards at the respective institutions. The London site has a subdivision that only looks after patients with microcarcinoma (tumor size <1 cm), whereas such a subdivision does not exist for the Halifax site. For the London site, we included patients diagnosed between 1998 and 2010; for the Halifax site, we included patients diagnosed between 2001 and to 2011. The study period for the Halifax site is different because data collection was started later at that site.
Staging of thyroid cancer
Individual cases of thyroid cancer were staged according to the American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) classification system, 6th edition (10). Information pertaining to clinical and pathological stage of thyroid cancer at presentation was obtained from clinic notes prepared by treating physicians and cross-referenced with original pathology and/or imaging reports.
Determination of socioeconomic status
Our study registry does not collect income data at the level of individual patients. Instead, we approximated household income by using a second data source—the Canadian Census of Population for the years 1996, 2001, and 2006. The finest level of disaggregation at which census information is released by Statistics Canada is the dissemination area (DA), a small, relatively stable geographic unit composed of one or more adjacent dissemination blocks, with a population of 400 to 700 persons (11). DAs cover all the territory of Canada. For each DA and for each of the three census years available, information was collected on average household income. Statistics Canada defines a census division (CD) as a group of neighboring municipalities joined together for the purposes of regional planning and managing common services. CDs in Ontario are typically at least 75,000 people but can range in population from fewer than 20,000 people to more than a million. In the province of Nova Scotia, CDs are smaller on average and range from fewer than 10,000 people to more than 300,000 in Halifax. DAs within each CD were sorted by average household income and then assigned to one of five income quintiles for that CD. For each case of thyroid cancer, an income quintile rank was assigned based on the DA corresponding to the patient's postal code of residence. This method controlled for differences in wages and prices across regions.
Postal Code Conversion File Plus (PCCF+) software was used to map individual patients' postal codes to a specific DA. In order to match postal code and DA information as closely as possible, cancer cases were assigned to census years as follows: cases presenting from 1996 to 2000 were associated with data from the 1996 census; cases presenting from 2001 to 2005 were associated with data from the 2001 census; and cases presenting from 2006 to 2010 were associated with data from the 2006 census.
Data analysis
Descriptive data are presented as mean±SD or number and percentage as appropriate. We used simple bivariate regression to compare characteristics between patients included from London and those from Halifax.
For the analysis of income in relation to thyroid cancer stage at presentation, the dependent variable of interest was the stage of thyroid cancer based on the AJCC TNM classification at the time of presentation. Four categories were defined, corresponding to Stages I, II, III, and IV. Since the dependent variable was ordinal, we used an ordered logistic regression to obtain odds ratios for being affected by high-stage thyroid cancer at presentation. The trend for stage and income was then estimated with simple linear regression. Interpretation of odds ratios on indicator variables is similar to that in a logistic model, in that an odds ratio greater than one implies that the indicator variable is associated with a greater likelihood of having a more advanced stage of cancer at presentation. The regressions included controls for the individual's sex, age at presentation, income quintile of the individual's neighborhood, and time trend. Time trend is a variable introduced to control for time-varying confounders. Location-specific regressions were also applied to compare patterns between sites. Finally, for the London site, we also included an indicator variable for the clinic at which the patient was assessed (i.e., regular clinic vs. microcarcinoma clinic). Statistical significance was accepted at a p-value of <0.05.
Results
A total of 1873 patients—1475 from London and 398 from Halifax—were seen in the thyroid cancer clinics and consented to participate in our registry. We excluded 141 London patients and 31 Halifax patients because of missing data (unmatched postal code, suppressed census information, or incomplete patient information). This resulted in 1701 patients for whom we had all the necessary information (Table 1).
Statistical comparisons were made using simple bivariate regression analysis comparing the London and Halifax sites.
AJCC, American Joint Committee on Cancer (10).
Considering the overall sample of patients, the mean age at the time of presentation was 47.5±15.1 years, ranging from 13 to 90 years. The majority (78%) was female. The average tumor size at presentation was 2.6±1.7 cm. A total of 43% of patients presented with Stage I thyroid cancer, 25% with Stage II, 24% with Stage III, and 8% with Stage IV.
When comparing the two sites, the sex distribution, size of thyroid tumor at presentation, and income quintile distribution were similar. The mean age was higher in Halifax (49.7±15.8 years) than in London (47.0±14.9 years; p=0.002). Significant differences were found in the percentage of patients diagnosed in each stage of thyroid cancer except for Stage IV: London's percentages were 19% lower for Stage I (p<0.001), 9% higher for Stage II (p=0.001), and 10% higher for Stage III (p<0.001).
The distribution of thyroid cancer patients across income quintiles is shown in Figure 1. Thyroid cancers were found more frequently in the SES groups with higher income (coefficient estimate 39.2, p<0.001 [CI 31.9–46.4]), with the number of thyroid cancer patients in the top quintile SES group being 68% higher than in the lowest quintile SES group.
Presentation of thyroid cancer in relation to income.
The relationship between income and the presenting stage of thyroid cancer is shown in Figure 2. Compared to patients in the top income quintile, patients in the lowest and second lowest income quintiles had significantly higher odds of presenting with more advanced stage thyroid cancer (OR 1.58 for lowest income quintile, p=0.002; OR 1.37 for second lowest income quintile, p=0.024). Higher thyroid cancer stage was found to correlate with lower income quintile (coefficient estimate −0.127, p=0.014 [CI −0.2 to −0.05]); that is, the odds ratio for being affected by more advanced thyroid cancer was reduced by 0.127 as one went up an income quintile. For every year increase in age at the time of presentation, the odds of thyroid cancer stage being more advanced were 2% higher (p<0.001; not shown in Fig. 2). The odds of a male facing higher stage thyroid cancer at presentation were more than twice that of a female (OR 2.10, p<0.001; not shown in Fig. 2).
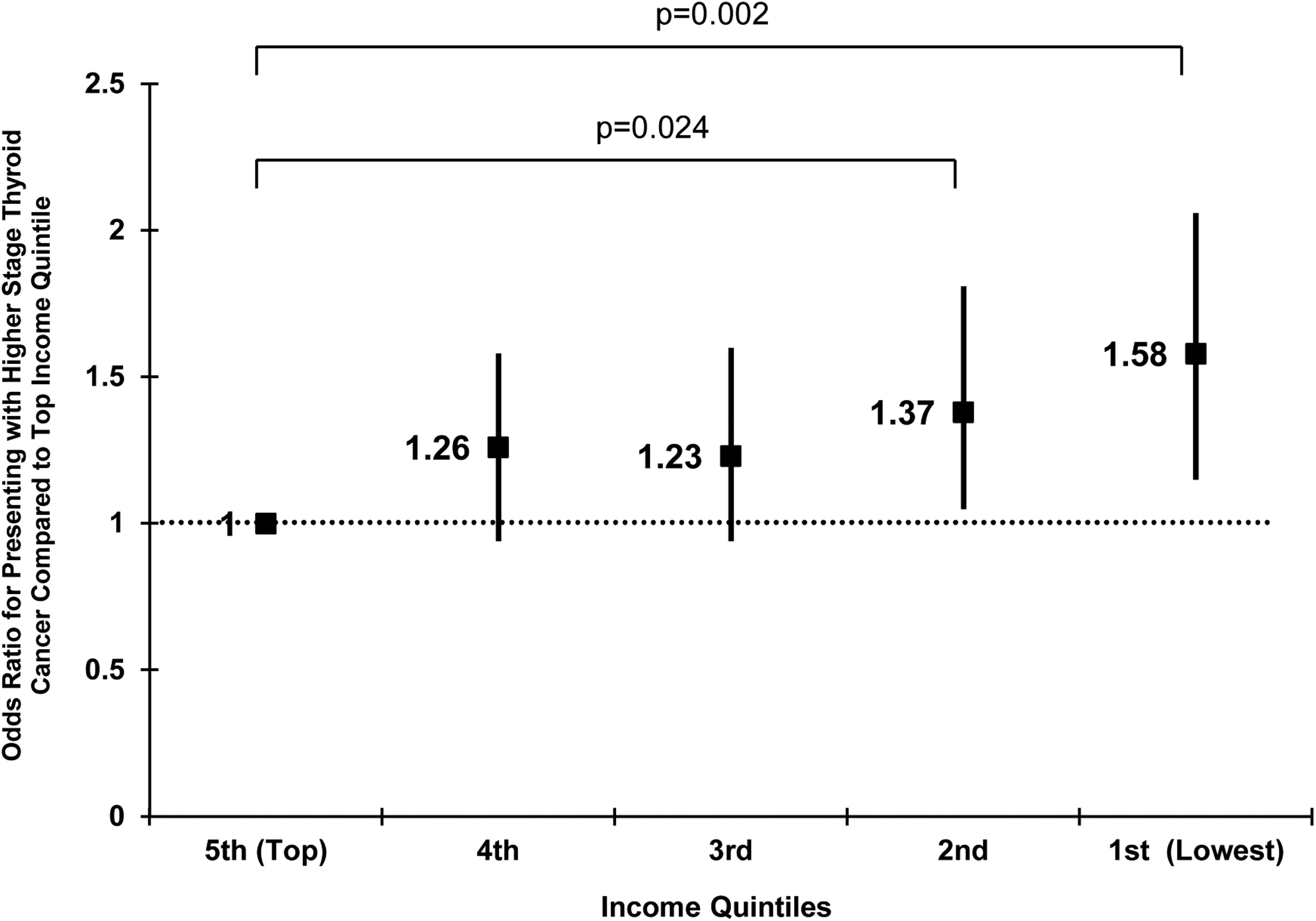
Thyroid cancer stage at presentation and income. Thyroid cancer stage at presentation analyzed per income quintile using ordered logistic regression. Results are presented as odds ratio and confidence interval as compared to the highest income quintile. An odds ratio greater than one indicates greater likelihood of having more advanced stage thyroid cancer at presentation.
Table 2 demonstrates results of ordered logistic regressions specified for each of the two participating sites. In London, the odds of getting higher-stage thyroid cancer were significantly higher in the first (i.e., lowest) and third income quintile when compared to the fifth (i.e., top) income quintile. The odds ratio for the second quintile was of similar size but lay just outside the 5% level of significance. For the Halifax site, we found a similar trend toward higher-stage thyroid cancer in the first and second income quintiles, but statistical significance was not reached. Consistent with results from regression on the combined London and Halifax sample, location-specific regressions again indicated that older age (OR 1.01, p=0.02 for London; OR 1.05, p<0.001 for Halifax) and male sex (OR 2.15, p<0.001 for London; OR 2.23, p=0.001 for Halifax) were associated with higher-stage thyroid cancer.
Per year increase in age.
Per year compared to the year prior.
Ordered logistic regression.
OR, odds ratio; CI, confidence interval.
Discussion
Our study results suggest that thyroid cancers were more frequently diagnosed in Canadian patients with higher SES, while patients with lower SES were diagnosed with more advanced-stage thyroid cancer at the time of presentation. We also found that SES correlated with thyroid cancer incidence and cancer stage at presentation in a stepwise manner.
These results, obtained from more than 1700 patients from two Canadian thyroid cancer referral clinics, are consistent with previous studies performed in the United States. A retrospective study in 292 patients in Texas, assessing the period between 1987 and 1994, found that neighborhood income was lower in the high-risk thyroid cancer group than in the low-risk thyroid cancer group (6). Another study found more advanced thyroid cancer in patients presenting to a public hospital than those presenting to a university teaching hospital (5). It has been suggested that lack of private insurance in patients presenting at the public hospital may be associated with more advanced thyroid cancer stage at diagnosis. In contrast to these studies, our study was done in Canada, which has a single-payer, government-funded system. Despite this, we found more advanced stage thyroid cancer in patients with lower SES, suggesting that an SES-related health disparity is also present in Canada. A few other studies in nonthyroid cancer have also suggested SES-related health disparity in Canada. In 1997, a population-based study conducted in Ontario, Canada, found that the risk of death from various cancers (not including thyroid cancer) ranged from 1.27-fold to 1.56-fold higher in patients with income less than $20,000 as compared to those with income more than $50,000 (12). A similar study from Ontario in 2010 demonstrated significant worsening of overall survival by 1.47-fold and 1.36-fold respectively for cancers of the breast and colon in patients from the lowest income quintile compared to the highest (13).
The degree to which SES affects thyroid cancer stage at presentation may vary between Canada and the United States. In the Texas study, patients from households with an income of less than $20,000 had threefold higher odds of being diagnosed with Stage III or Stage IV thyroid cancer compared to patients from households with an income of more than $20,000 (6). In our study, patients from the lowest income quintile had about 1.5-fold higher odds of getting advanced-stage thyroid cancer, the risk increase being about half of that seen in the Texas study. While these data are very limited, they suggest that the degree of health disparity in Canada may perhaps be less profound than in the United States. One potential contributing factor for health disparity in Canada may be the nonmedical costs related to accessing the healthcare system, for example travel costs to tertiary centers, parking, hotel stays, and loss of income. While patients do not pay for direct medical costs in a universal healthcare system, patients with lower SES could be disproportionately affected by these nonmedical costs. More studies are needed to test this hypothesis and determine to what magnitude a universal healthcare system reduces health disparity with respect to thyroid cancer diagnosis and treatment.
Another potential contributing factor may be related to differences in the extent to which individuals from different SES levels choose to access primary care, have periodic health examinations, or have neck ultrasounds. In our study, we found that patients with higher household income were more frequently diagnosed with thyroid cancer, with this relationship progressing in a stepwise manner with more thyroid cancer cases found as one goes up consecutive income quintiles. This finding is consistent with a recent study based on the SEER database that found a positive correlation between thyroid cancer incidence and healthcare access, with the latter measured using a number of surrogate markers such as family income, level of education, insurance status, and English as primary language (14). Similarly, a separate study, also using the SEER database, analyzed thyroid cancer incidence with respect to time and found more rapid rise in incidence in patients from higher SES groups compared to those from the bottom SES quartile (15). The importance of diagnosing small thyroid cancers is under debate. Some authors have suggested that there may be an overdiagnosis of cancer, which is defined as detecting an indolent “cancer” that would otherwise not go on to cause symptoms or death (16,17). Further study of observed patterns between tumor size and SES may be instructive in this regard.
We included two Canadian regions in our study: Southwestern Ontario and Nova Scotia. Subgroup analysis based on geographic location found a strong association between low income and high-stage thyroid cancer for the London area and a similar trend for Nova Scotia, though it did not reach statistical significance. The latter was likely caused by a lack of power for the Halifax site, which included fewer patients than the London site (367 vs. 1334 patients). A larger sample size across multiple regions will be needed to investigate this suggestion.
The tumor stages found at presentation were different between Halifax and London, with London having a lower proportion of patients with Stage I, and a higher proportion of patients with Stage II and Stage III as compared to Halifax. This was perhaps related to variation in referral pattern. The Halifax site is the single referral center for all patients with thyroid cancer within Nova Scotia. The London site is a referral center for patients from a much larger region including Southwestern and Northern Ontario who require additional treatments, particularly radioactive iodine. This likely resulted in a shift toward a more advanced stage at presentation for the London site.
In other regressions not reported here, we also included a set of indicator variables for the census division of residence of each patient. These binary variables reflect unobserved differences across region of residence of individuals that might be important for stage at presentation or tumor size, such as proximity to a hospital or clinic. Including these variables did not qualitatively change the results.
There are several limitations to our study. Our study database may not be representative of all cancer cases occurring in the respective regions and was accrued on a referral basis rather than that of a regional cancer registry. The pattern of referral of patients to tertiary referral centers may have changed over time. Enrollment into our study database, while high (>95% of patients consented to enroll), was dependent upon patients' consent. In relation to SES, we were only able to approximate household income from census-level neighborhood data rather than individual-level data. However, this method had been used previously (18). Finally, while our study suggests that health disparity in thyroid cancer is present in Canada, it remains to be elucidated if and to what extent this may affect clinically relevant outcomes. Our study categorized thyroid cancer based on the widely used AJCC TNM classification system, which predicts disease-specific mortality (10). However, as mortality from thyroid cancer is low, it might be prudent to use the recently introduced ATA classification system (19) to assess the relation between SES and thyroid cancer outcomes. Our study did not include data on possible confounders, for example fluency in English (required for informed consent), obesity, alcohol use, and smoking history, which are related to SES and may affect thyroid cancer risk. Obesity has been proposed as a risk factor for thyroid cancer (20), while cigarette smoking and alcohol intake are associated with reduced risk of papillary thyroid cancer, the most common form of differentiated thyroid cancer (21). Our study can, however, not assess whether these factors may influence the relation between SES and incidence and stage of thyroid cancer at presentation.
Our study is notable for a number of strengths. Most previous studies on the relationship between thyroid cancer and SES focused on cancer incidence, whereas very few studies have investigated such relationship focusing on cancer stage at presentation. Our study investigated the latter using a much larger group of patients than any similar studies in the past. We enrolled patients from two Canadian sites, reducing the chance of single-center bias. Also importantly, we are the first group, to our knowledge, to explore the relationship between SES and thyroid cancer based on data from a country that provides universal healthcare. Our study sample of patients displayed similar characteristics as those in other thyroid cancer study populations. Much like other studies (22,23), our study found that the majority, almost 80%, of thyroid cancer patients were female. Male patients presented with more advanced stage thyroid cancer; this is consistent with findings from other studies (5,6). Further, we found an association between older age and more advanced thyroid cancer; this is consistent with previous findings that older age carries worse prognosis in thyroid cancer (22 –24).
In conclusion, this study in two Canadian thyroid cancer centers found that lower SES was associated with more advanced thyroid cancer stage at presentation, and higher SES was associated with higher frequency of presentation with thyroid cancer. Further studies will be required to explore the underlying reasons, as well as if and to what extent SES-related differences in thyroid cancer stage translate into differences in clinical outcomes.
Footnotes
Acknowledgments
The Canadian Thyroid Cancer Consortium has received funding in the form of unrestricted grants from Genzyme Inc., Canada. We thank Helen Fong, Laura Wood, and Christina Keller for their invaluable assistance.
Author Disclosure Statement
No competing financial interests exist.