
Abstract
Background:
As defined by the Dietary Supplement Health and Education Act 1997, such substances as herbs and dietary supplements fall under general Food and Drug Administration supervision but have not been closely regulated to date. We examined the thyroid hormone content in readily available dietary health supplements marketed for “thyroid support.”
Methods:
Ten commercially available thyroid dietary supplements were purchased. Thyroid supplements were dissolved in 10 mL of acetonitrile and water with 0.1% trifloroacetic acid and analyzed using high-performance liquid chromatography for the presence of both thyroxine (T4) and triiodothyronine (T3) using levothyroxine and liothyronine as a positive controls and standards.
Results:
The amount of T4 and T3 was measured separately for each supplement sample. Nine out of 10 supplements revealed a detectable amount of T3 (1.3–25.4 μg/tablet) and 5 of 10 contained T4 (5.77–22.9 μg/tablet). Taken at the recommended dose, 5 supplements delivered T3 quantities of greater than 10 μg/day, and 4 delivered T4 quantities ranging from 8.57 to 91.6 μg/day.
Conclusions:
The majority of dietary thyroid supplements studied contained clinically relevant amounts of T4 and T3, some of which exceeded common treatment doses for hypothyroidism. These amounts of thyroid hormone, found in easily accessible dietary supplements, potentially expose patients to the risk of alterations in thyroid levels even to the point of developing iatrogenic thyrotoxicosis. The current study results emphasize the importance of patient and provider education regarding the use of dietary supplements and highlight the need for greater regulation of these products, which hold potential danger to public health.
Introduction
There have been several reported cases of factitious hyperthyroidism in patients taking nutritional supplements marketed to improve thyroid function or promote weight loss (5 –11). A case of drug-induced thyrotoxicosis was reported in a patient with postsurgical hypothyroidism who preferred to take “natural thyroid hormone” over the prescribed thyroid hormone medications. Serum thyrotropin remained in the undetectable range while taking the manufacturer's recommended dose of the supplement that contained bovine thyroid tissue. The excess in thyroid hormone replacement resulted in overt symptomatic thyrotoxicosis in the patient (5). In another case, a 20-year-old female patient took a nutritional supplement containing 60 mg bovine thyroid, 30 mg kelp, and other bovine glandular tissue, and she presented with symptomatic thyrotoxicosis just by taking the supplement at the recommended dose directed on the label. The patient's thyrotropin normalized within six weeks after stopping the supplement (6). There is a great potential for harm to people taking these unregulated thyroid hormone–containing supplements, as exposure to excess thyroid hormone can have numerous deleterious effects. With the current method of monitoring dietary supplements essentially by reports of adverse effects, the public is virtually unprotected against supplements containing ingredients that are potentially unsafe.
We examined the thyroid hormone content in 10 dietary health supplements marketed to the public for “thyroid support.” To date, there are no reported studies examining thyroid hormone content in widely available dietary supplements. The aim of the study was to determine the presence of active thyroid hormone in these supplements and calculate the daily dose received when taking the supplement according to the manufacturer's recommendation.
Materials and Methods
Thyroid supplements
Ten commercially available thyroid health supplements were purchased from retail stores in the local geographical region or via the Internet. The products were selected by an Internet search using key word searches including “thyroid health,” “thyroid supplements,” and “thyroid support.” The 10 thyroid health products identified as having the most commonly viewed websites by our Internet search were selected. Once the products were purchased, they were given a unique product identification (ID) number and recorded by their brand name, manufacturer, dosage form (tablet or capsule), and purchase location. Five products purchased were herbal-based supplements with no indication on the label that animal thyroid tissue was contained in the product, and the other five products were labeled as containing “raw thyroid” tissue, concentrate, or powder from bovine source. The selected products were analyzed for the presence of measurable amounts of thyroxine (T4) and triiodothyronine (T3). We used levothyroxine and liothyronine carried by the Walter Reed Army Medical Center pharmacy to be run as positive controls and standards. Three samples from each product were analyzed with the results for each of the samples being recorded as a mean value. The laboratory investigators who ran the samples were blinded to the product information, having been provided the samples with only a unique sample ID number.
Sample preparation and high-performance liquid chromatography analysis
Each tablet of supplement or standard (liothyronine sodium, levothyroxine sodium) was dissolved in 10 mL of acetonitrile and water with 0.1% trifloroacetic acid (50:50 v/v). For product ID numbers 6, 7, 8, 9, and 10, two tablets were dissolved as above to increase the sensitivity of detection. The suspension was centrifuged at 872 g (2000 rpm, Thermo Scientific Survall Legend XTR) for 10 minutes and the supernatant was used for analysis. T3 and T4 levels were measured by high-performance liquid chromatography (12 –14) (FIG. 1), which consisted of a Waters 2998 Photodiode Array Detector, Waters 2695 Alliance, and a column, Nova-Pak CN HP 60A 4 μm, 75 mm×3.9 mm i.d. (Waters, Milford, MA). A mobile phase consisted of acetonitrile and water with 0.1% trifluoroacetic acid (40:60 v/v). The detector was set at 225 nm, and 40 μL of standard or sample was injected with the autosampler. The following concentrations of standards were used for the external calibration curve: 78.1, 156.3, 312.5, 625.0, and 1250.0 ng/mL. Using four levels of standard as control to monitor the accuracy and precision of the assay yielded a recovery of 97.3% for T3 and 94.3% for T4. The average of R 2 for the standard curve for T3 was 0.9992 and for T4 was 0.9985. Chromatographic data were processed using the Empower Chromatography Management software (Waters). Results were listed by product identification number and amount of T4 and T3 in micrograms per tablet (mean±standard deviation). Total or daily recommended dose of T4 and T3 were calculated per serving instruction included on the product label.
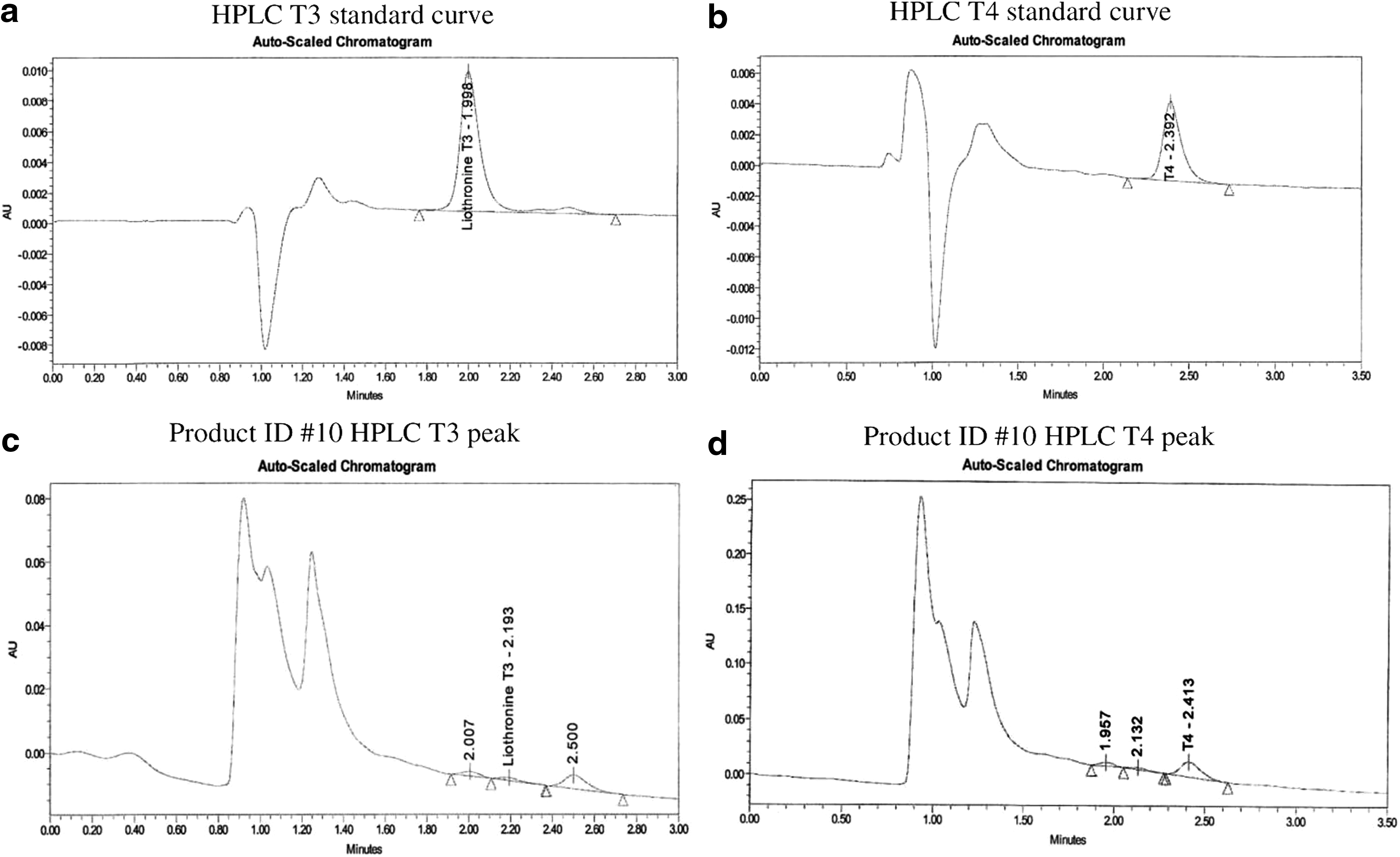
High-performance liquid chromatography (HPLC) curves for thyronine (T3) and thyroxine (T4) assays in standard liothyronine sodium
Results
The amounts of T3 and T4 in micrograms per tablet are presented in Table 1. The 10 supplements are listed by product ID number and reported as mean T3 and T4 values for triplicate runs. Nine out of 10 products revealed a detectable amount of T3 ranging between 1.3 and 25.4 μg/tablet. Taken at the manufacturer's recommended dose, five supplements delivered T3 quantities of greater than 5 μg/day (5.5–25.4 μg/day). Five products showed a detectable amount of T4 ranging from <0.5 to 22.9 μg/tablet. Taken at the recommended dose, one product delivered a T4 quantity of >25 μg/day. Five products (product ID numbers 2, 3, 5, 9, and 10) contained a detectable amount of both T3 and T4. Product ID number 3 contained the greatest amount of measured T3 and T4, with both hormone levels being significantly greater than the lowest dose of levothyroxine (25 μg) and liothyronine (5 μg) available under prescription.
As provided on the label.
Mean±SD.
Calculated maximum/total daily dose (mean) per recommended daily intake dose.
ID, identification; T3, triiodothyronine; T4, thyroxine.
Five products included in the study were labeled as containing bovine thyroid tissue, extract, or concentrate (product ID numbers 6–10). One of the products (product ID number 7) had no detectable level of T3 or T4, product ID numbers 6 and 8 contained T3 only, and product ID numbers 9 and 10 revealed detectable amounts of both T3 and T4. The two products with detectable amounts of T3 and T4 were labeled as containing a processed bovine thyroid tissue as extract or concentrate. The other five products were listed as herbal-based supplements (product ID numbers 1–5) based on the manufacturer's label not listing any content of animal thyroid gland products. All contained various amounts of L-tyrosine (150–1000 mg) and iodine (100–240 μg). Herbs commonly found in the herbal-based supplements were guggul (Commiphora mukul), kelp, ashwagandha (Withania somnifera), bladderwrack (Fucus vesiculosis), Coleus forskohlii, and Schisandra chinensis. All five herbal-based supplements contained detectable amounts of T3, and two of them had detectable levels of T4 (Table 1).
Discussion
In the present study, we report that the majority of dietary thyroid supplements analyzed contained clinically significant amounts of T3 and/or T4. Five products labeled to contain bovine thyroid tissue revealed variable amounts of T3 and/or T4 level, whereas the other five products containing various herbs and minerals with no information on animal thyroid products all had detectable T3 and/or T4. In the latter group, one of the products would potentially deliver 32 μg of T3 hormone per day if taken at the recommended daily dose. The calculated daily dose of several of the products equaled or exceeded common treatment doses for hypothyroidism. The significant amounts of thyroid hormone in these products place unwitting consumers at an increased risk for the development of thyrotoxicosis and its associated complications. Thyroid hormone medication is classified as a narrow therapeutic drug by the Food and Drug Administration, and therefore close monitoring of thyroid hormone levels is required. However, clinical experience indicates that consumers taking these supplements go untested for the most part until they either develop adverse symptoms or have thyroid blood test done by their provider for other indications. Furthermore, many patients do not report the use of such dietary supplements to their providers unless specifically questioned about their use.
Dietary and herbal thyroid supplements marketed to improve thyroid health or support thyroid function so as to improve energy and/or promote weight reduction appeal to many patients who are under the misconception that herbal products are safer than conventional medications. A case series from Japan reported 12 patients who presented with thyrotoxicosis from taking a nonprescribed weight control herbal product called “Dream Shape” and “Ever Youth” (8). Both claimed to contain natural food products and neither indicated thyroid hormone or desiccated thyroid tissue content. T3 and T4 were measured from two products, which revealed a content of T3 ranging between 0.97 and 1.1 μg, and of T4, between 3.1 and 4.5 μg per capsule. An undeclared animal thyroid tissue used in a Chinese herbal supplement was reported in a patient who presented with factious thyrotoxicosis and a suppressed thyrotropin <0.1 μIU/mL (9). In 2006, French health authorities banned the importation, preparation, prescribing, and dispensing of substances that contain thyroid powder, thyroid extracts, and thyroid hormones or thyroid hormone derivatives following a thyrotoxicosis-related death in conjunction with the use of a “slimming aid” that contained powdered thyroid extract (15).
Among 10 thyroid supplements used in the current study, 5 were not labeled to contain bovine thyroid tissue or hormones but still had detectable amounts of thyroid hormone. Herbs commonly found in the active ingredients were iodine-rich substances such as kelp or bladderwrack (F. vesiculosus), or substances believed to be thyroid stimulants, Ashwagandha root (W. somnifera), C. forskohlii, or guggul based on animal studies. Kelp or bladderwrack are used as a source of iodine in herbal medicine to treat patients with underactive thyroid glands. Large doses of iodine may occasionally precipitate a reversible hyperthyroidism in patients with underlying autoimmune thyroid autonomy (16). Ashwagandha, known as “Indian ginseng,” has shown thyroid stimulatory effects leading to thyrotoxicosis in an animal study (17). C. forskohlii is often used in cell physiology research as its byproduct, forskolin, stimulates cyclic AMP production, which may play a role as a stimulant on thyroid hormone production by promoting sodium-iodide symporter function. S. chinensis does not have known thyroid stimulatory effects in animal studies (18). Any thyroid stimulatory actions of these herbal substances do not account for detectable amounts of thyroid hormones in our in vitro study. However, the possibility of additional effects of these preparations on endogenous thyroid function further heighten the concerns raised in this study. The presence of T3 alone in some of the samples would appear to implicate selective addition of this hormone to the product, as those containing a desiccated animal source would be expected to have both T4 and T3 present. Adulteration of herbal supplements is not uncommon. Under the Dietary Supplement Health and Education Act of 1997, there are no federal standards for dietary supplements in regard to product consistency, purity, and quality. Several reports in the medical literature describe adverse effects secondary to herbal supplements that were subsequently revealed to deviate from either the labeled content or the dose of active ingredients (19 –21).
This study documents the presence of a detectable amount of T3 and T4 in readily available dietary supplements, with some of them containing clinically significant amounts of T3 and T4 equal to or exceeding standard thyroid hormone dosing for hypothyroid patients. Patients purchasing these products may do so under the misunderstanding that the products are proven safe and that they hold some benefit in improving thyroid function. However, an accumulating body of clinical evidence indicates safety concerns with these products and to date no definitive data exist regarding the efficacy of various herbs to improve thyroid function.
Our study has several limitations. First, the study did not attempt to measure thyroid hormone levels in patients receiving these supplements. However, as the exact contents of any one of these products are not fully known to us and as they may hold a risk for development of thyrotoxicosis, we did not feel that it would be ethical to administer these supplements to human research subjects. Next, the 10 supplements we studied may not be representative of all available preparations, but since nearly all contained thyroid hormone, we suspect otherwise.
The findings of this study emphasize the importance of educating both patients and providers on the potential adverse effects related to the use of dietary and herbal supplements marketed to improve thyroid function. They also highlight the need for greater regulation of these supplements as they hold potential medical hazards to the public. It is essential that providers screen all patients for dietary or herbal supplement use and recognize that abnormal thyroid function can result from the use of such products. Furthermore, patients should be educated and counseled that substances deemed as “natural” are not automatically safe and free from adverse effects.
Footnotes
Acknowledgment
The authors acknowledge the Henry M. Jackson Foundation for supporting study funds.
Author Disclosure Statement
The authors have no conflict of interest to disclose.