
Abstract
Background:
Symptomatic hyponatremia in association with radioactive iodine (RAI) therapy for differentiated thyroid cancer has rarely been reported. Due to the increasing incidence of thyroid cancer worldwide, more patients are now receiving postoperative RAI therapy. We report two cases of life-threatening severe hyponatremia in association with RAI therapy.
Summary:
Two elderly female patients who had bilateral thyroidectomies for their thyroid cancer underwent a low-iodine diet and levothyroxine withdrawal for two weeks prior to RAI therapy. Upon admission, the patients were given 130 mCi (4810 MBq) and 150 mCi (5550 MBq) of 131I respectively, and oral hydration (two to three liters of water daily) to increase the frequency of emptying the bladder of RAI. Both patients completed their RAI therapy without significant complications and were discharged from hospital. Two days after discharge, both patients were admitted to the emergency room with complaints of severe nausea and dizziness. Initial laboratory tests revealed that they were in a hypothyroid state and had severe hyponatremia with a serum sodium level of 108 mEq/L. The symptomatic hyponatremia responded to intravenous hypertonic saline infusion and thyroid hormone replacement, and the patients made a full recovery. The low-iodine diet and hypothyroid state with overzealous hydration in the setting of RAI therapy may have provoked severe hypotonic hyponatremia.
Conclusion:
Hypothyroid patients after undergoing RAI therapy, especially the elderly, are at an increased risk for serious hyponatremia and should be monitored closely.
Introduction
T
Patient 1
A 70-year-old woman was admitted to our emergency room (ER) with complaints of worsening dizziness and nausea. Her medical history revealed that she had hypertension, which was well controlled with valsartan 80 mg daily. Two months prior to her ER visit, she underwent a bilateral total thyroidectomy with central compartment neck dissection for papillary thyroid cancer with regional lymph-node metastasis (TNM stage T4aN1aM0). The day after the bilateral total thyroidectomy, she started to take levothyroxine 0.15 mg daily for four weeks until she switched to liothyronine 40 μg daily for another two weeks. A low-iodine diet was prescribed along with thyroid hormone withdrawal two weeks prior to RAI therapy. On the day of admission for RAI therapy, her serum sodium concentration was 135 mEq/L, and she was given 130 mCi (4810 MBq) of 131I. On the second day of hospitalization, she complained of mild nausea that was controlled by metoclopramide 10 mg and granisetrol 1 mg. She was advised to drink two to three liters of fluid daily for two days to facilitate elimination of residual RAI in the bladder. No further complaints were reported, and she was discharged on the third day after administration of RAI. She was given a prescription to restart levothyroxine 0.15 mg per day following discharge from hospital. Thyroid hormone replacement was delayed per protocol at our institution.
The patient was admitted to our ER two days after discharge. In the ER, her blood pressure was 140/80 mmHg, her pulse rate was 72 beats per minute, and her body temperature was 36.8°C. Upon examination, she was fully alert but complained of severe fatigue and dizziness. Skin turgor was not decreased, and her jugular vein was not distended. There was no pitting edema on the lower extremities. A full physical examination showed no abnormalities. A chest radiograph showed a normal cardiothoracic ratio, and initial blood tests demonstrated a critically low serum sodium concentration of 108 mEq/L (normal: 135–145 mEq/L). Further laboratory findings revealed a hypothyroid state accompanied by hypotonic hyponatremia with a high urine sodium and a urine osmolality greater than the serum osmolality. Laboratory values are summarized in Tables 1 and 2.
AST, aspartate aminotransferase; ALT, alanine aminotransferase; RBC, red blood cells; WBC, white blood cells.
Baseline values were obtained immediately after thyroidectomy.
BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate was calculated using Modification of Diet in Renal Disease equations; ER, emergency room; RAI, radioiodine; T3, triiodothyronine; T4, thyroxine; tCO2, total carbon dioxide; TSH, thyrotropin.
The patient was initially given intravenous normal saline with potassium and calcium supplements to correct her electrolyte disturbance and neurologic symptoms. Levothyroxine 0.15 mg was also given to replace thyroid hormone. However, despite initial infusion of normal saline and levothyroxine administration in the ER, her neurologic symptoms persisted, and her serum sodium concentration declined to 107 mEq/L. Therefore, the levothyroxine dosage was increased to 0.3 mg on the second day of admission, and 3% saline solution was started at 40 mL/hour. The subsequent 3% saline infusion was guided by frequent monitoring of her serum sodium concentrations and lasted for 48 hours. The patient was advised to restrict free water intake and was monitored meticulously (Fig. 1). By the fifth day of admission, her neurologic symptoms improved, and the serum sodium concentration gradually improved to 135 mEq/L. She was discharged from the hospital, and her follow-up serum sodium level was 145 mEq/L on the 16th day after discharge without any further symptoms or complaints.
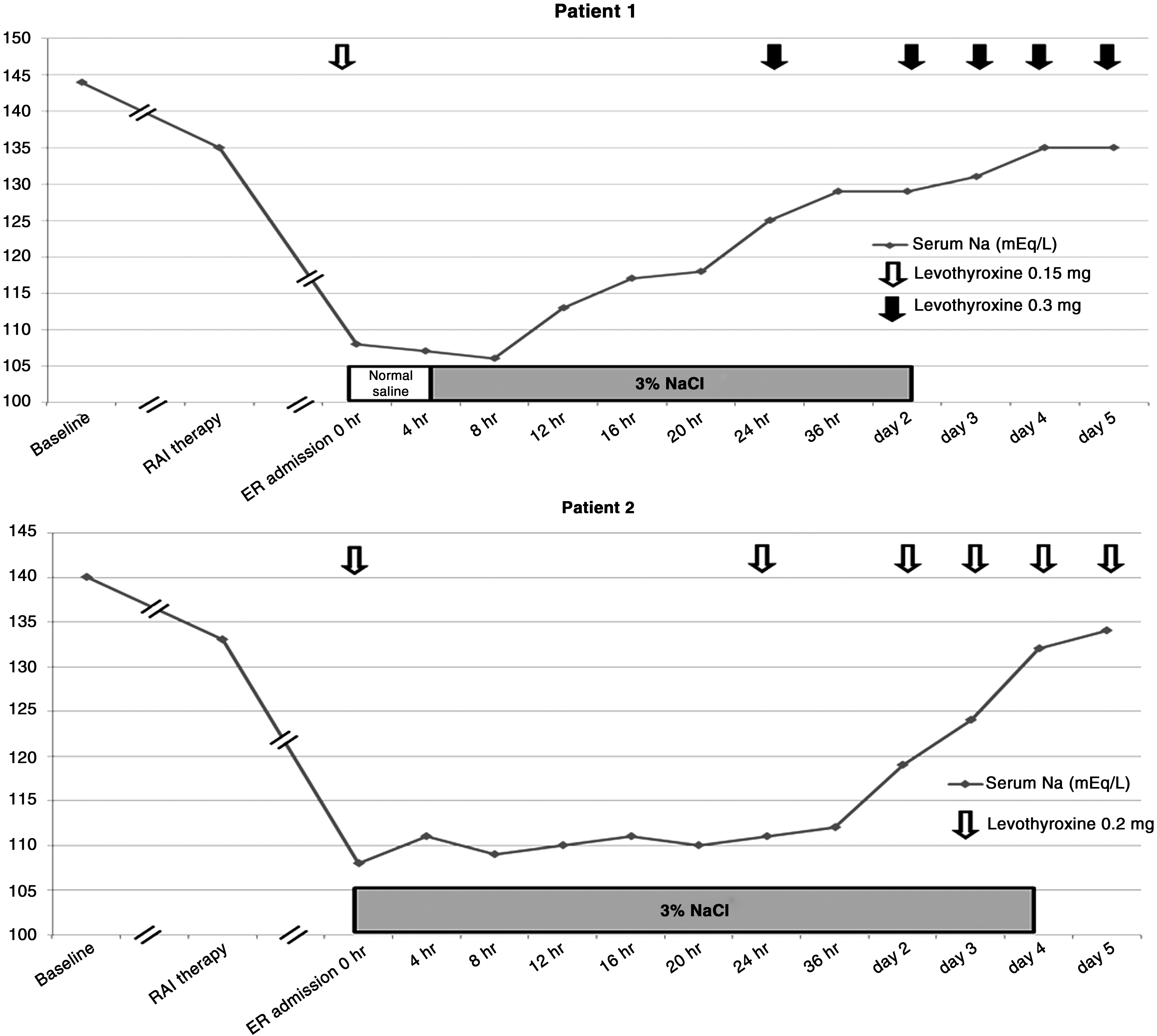
Serial changes in serum sodium concentrations at different stages of clinical course. Treatment with intravenous infusion of normal saline and hypertonic saline is shown as a bar graph. Downward open and closed arrows indicate time points of thyroid hormone administration.
Patient 2
A 68-year-old woman was admitted to our ER for severe nausea, vomiting, and impaired consciousness. She also had hypertension for 20 years and was managed with a combination of amlodipine 5 mg, telmisartan 40 mg, and hydrochlorthiazide 12.5 mg daily. Two months prior to her ER visit, she was diagnosed with papillary thyroid cancer with regional lymph-node metastasis, and she underwent a bilateral total thyroidectomy with central compartment neck dissection (TNM stage T4aN1bM0). On the day after the thyroidectomy, she started to take levothyroxine 0.2 mg daily for four weeks until her medication was switched to liothyronine 40 μg daily for two more weeks. She was advised to adhere to a low-iodine diet, and thyroid hormone replacement was withdrawn for two weeks prior to RAI therapy. On the day of admission for RAI therapy, her serum sodium concentration was 133 mEq/L, and she was given 150 mCi (5550 MBq) of 131I. On the second day of RAI therapy, she complained of nausea, and metoclopramide 10 mg and ondansetron 8 mg were given to control her symptoms. She was advised to drink two to three liters of fluid daily for two days to facilitate adequate elimination of residual RAI. No further complaints were reported, and she was discharged on the third day of RAI therapy. She was also given a prescription to restart levothyroxine 0.2 mg per day following her discharge from hospital per protocol.
The patient was admitted to our ER two days after discharge from RAI therapy. In the ER, her blood pressure was 160/70 mmHg, her pulse rate was 104 beats per minute, and her body temperature was 36.8°C. Upon examination, she was disoriented and complained of nausea and vomiting. Skin turgor was not decreased, and her jugular vein was not distended. There was no pitting edema on her lower extremities, and a full physical examination showed no abnormalities. A chest radiograph showed a normal cardiothoracic ratio, and initial blood tests demonstrated a critically low serum sodium concentration of 108 mEq/L. Further laboratory findings revealed that the patient was in a hypothyroid state accompanied by hypotonic hyponatremia with a high urine sodium and a urine osmolality greater than her serum osmolality. Laboratory values are summarized in Tables 1 and 2.
Hydrochlorothiazide, which could cause or aggravate hyponatremia, was stopped immediately, and administration of levothyroxine 0.2 mg was initiated to replace thyroid hormone. Intravenous 3% saline solution was also immediately started at 50 mL/hour in the ER because of her neurologic signs with disorientation. The rate of the subsequent hypertonic saline infusion was guided by frequent serum sodium concentration monitoring and was adjusted to avoid rapid overcorrection of her serum sodium. The patient was advised to restrict free water intake and was monitored meticulously (Fig. 1). Her neurologic symptoms and symptoms of nausea and vomiting improved along with gradual correction of her serum sodium concentration. She was discharged from the hospital on the fifth day after ER admission, and a daily dose of 0.2 mg levothyroxine was prescribed. She was advised to discontinue taking hydrochlorothiazide. Her serum sodium level was 139 mEq/L on the sixth day after discharge, and her follow-up examinations revealed no complications of hyponatremia.
Discussion
Many institutions restrict dietary iodine intake and withdraw levothyroxine for at least two weeks prior to RAI therapy to decrease the total body iodine pool and maximize the RAI uptake by residual thyroid tissues (2). Such a low-iodine diet is usually accompanied with low salt intake, and rare cases of severe symptomatic hyponatremia associated with a low-iodine diet have been reported (4 –6). Recently, Al Nozha et al. (6) reviewed eight cases of life-threatening hyponatremia associated with a low-iodine diet prior to RAI therapy. They suggested that a prolonged low-iodine diet, low salt intake, and the use of thiazide diuretics in elderly patients are risk factors for the development of severe hyponatremia (6). Consistent with their data, our patients were also elderly females, and one was taking hydrochlorothiazide for treatment of underlying hypertension. However, our patients developed severe hyponatremia only after completion of RAI therapy. They underwent a low-iodine diet and levothyroxine withdrawal per protocol prior to RAI therapy, and the patients' blood chemistries demonstrated only slightly subnormal serum sodium concentrations before initiation of RAI therapy. The RAI was given as scheduled, and the patients were discharged two days after completion of RAI therapy. However, both patients developed severe symptomatic hyponatremia at home, which warranted ER admission. The patients reported here underline the potential complications of severe hyponatremia in patients undergoing RAI therapy and suggest the need for careful monitoring of serum sodium concentrations not only during RAI therapy but also throughout the immediate post-RAI therapy period in high-risk elderly patients.
Hypothyroidism is commonly encountered in RAI therapy. However, short-term hypothyroidism after RAI therapy for high-risk thyroid carcinoma is usually not associated with severe hyponatremia (7). In the literature, elderly patients in a hypothyroid state, like our patients, have rarely been reported to develop severe hyponatremia. Patients undergoing high-dose RAI therapy at our institution are given levothyroxine after a short delay per protocol, and this may have led to an aggravated hypothyroid state. Possible mechanisms for the development of hyponatremia in a hypothyroid condition are impaired water excretion and failure to achieve maximal urinary dilution. Exaggerated natriuresis in response to volume alterations in a senile kidney is another possible mechanism resulting in a hyponatremic state (8). Furthermore, inappropriate antidiuretic hormone (ADH) secretion, which is observed secondary to the age-related physiological changes in salt and water balance in elderly patients, may have also contributed to the observed hyponatremia (9,10). In a state of normal or increased fluid intake, the inability to decrease urine osmolality below plasma osmolality may result in hyponatremia (11). This failure to dilute the urine is generally caused by not being able to suppress ADH secretion maximally (11). Failure to suppress plasma ADH during an acute water load in hypothyroid patients was initially reported by Skowsky and Kikuchi (12), and a recent animal model of hypothyroidism also demonstrated nonosmotic release of ADH and impaired urinary dilution (13). The absence of any reported hypotensive events in our patients argues against baroreceptor-mediated nonosmotic secretion of ADH and dilutional hyponatremia. Compared to younger individuals, elderly patients in a hypothyroid state are more susceptible to the dangers of hyponatremia because of excessive ADH (9,10). Unfortunately, plasma ADH levels were not measured in our patients. However, increased urine osmolality and urinary sodium excretion suggest a failure to dilute the urine maximally and to suppress plasma ADH during increased water intake. It may be prudent to start levothyroxine 24 hours after RAI therapy to avoid any excessive hypothyroid state in elderly patients prone to electrolyte imbalance.
Acute complications of RAI therapy usually include nausea and vomiting, salivary gland swelling, and stomatitis in a dose-dependent manner (3). Studies have shown that 50% to 67% of patients complain of nausea starting as early as two hours after RAI treatment and lasting up to two days after therapy (3). Stomatitis and sialadenitis are also common complications of RAI therapy that lead to poor oral intake and aggravate hyponatremia. Complaints of nausea were controlled with frequent antiemetic medications, and this aggressive management may have masked the derangement of the underlying serum sodium concentration.
Excessive oral hydration may have contributed to the development of severe hyponatremia in our patients. Oral hydration is usually recommended to promote frequent urination to empty the bladder of residual RAI (3). Our patients were advised to drink two to three liters of fluid daily, and both patients drank tea, which is basically sodium-free water. Although the exact mechanism of development of hyponatremia in the setting of RAI therapy in elderly patients is not evident, overzealous sodium-free water intake in the setting of a urinary dilution defect may have contributed to the development of an electrolyte imbalance.
In conclusion, especially elderly patients with thyroid cancer may develop severe hyponatremia in association with hypothyroidism, low dietary sodium intake, and excessive hypotonic fluid intake after RAI therapy. In elderly patients undergoing RAI therapy, sodium concentration should be measured, thiazide diuretics should be avoided, and early replacement of levothyroxine is recommended.
Footnotes
Author Disclosure Statement
No competing financial interests exist.