
Abstract
Background:
Recent studies have suggested that metformin (MF) may lower thyrotropin concentration. This suggests a possible need for a dose reduction of levothyroxine in hypothyroid patients taking MF. However, contradictory results from heterogeneous study populations indicate that the underlying causes have not been completely elucidated. Patients with postoperative hypothyroidism—a condition not influenced by endogenous thyroid hormone production—have not been evaluated in order to evaluate the impact of MF.
Aim:
To determine the impact of MF in total thyroidectomized patients receiving levothyroxine replacement.
Patients and Methods:
One hundred ninety-two patients underwent total thyroidectomy during three years and were receiving levothyroxine substitution. Patients were divided into two groups depending on MF use: the non-MF group included 159 patients, of whom 134 were women [mean (SD) age, 52 (15.7) years; mean (SD) body weight, 70.2 (13.5) kg; 56 with differentiated thyroid cancer]; the MF group comprised 33 patients, of whom 24 were women [mean (SD) age, 63 (9.8) years; mean (SD) body weight, 79.3 (13.9) kg; 9 with differentiated thyroid cancer]. Levothyroxine requirements were compared between the groups, and the differentiated thyroid cancer cases were also analyzed separately.
Results:
Thyrotropin levels did not differ significantly between the MF and the non-MF groups. No differences in total levothyroxine dosage were found: 114 (100–150) [median (Q1–Q3)] μg in the non-MF group versus 125 (100–142) μg in the MF group (p=0.9). When calculating the weight-adjusted levothyroxine dose, significant differences were evident: 1.66 (1.38–2.08) μg/kg in the non-MF group versus 1.53 (1.26–1.70) μg/kg in the MF group (p=0.010). However, in a multivariate regression model with thyrotropin levels, age, body mass index, sex, and type of thyroid disease, MF treatment lost its significance.
Conclusions:
Thyroidectomized patients receiving MF treatment need a lower thyroxine dose than patients who do not receive the drug, possibly due to different characteristics (greater weight, age) of the patients with diabetes mellitus type 2.
Introduction
T
During the past 5 years, several publications have focused on the relationship between MF and thyroid function in an attempt to shed light on this issue. Most studies have confirmed the TSH-lowering effect of MF; however, the majority of studies were small in sample size and/or were carried out in certain groups of patients such as those with obesity (3) or polycystic ovarian syndrome (4). Besides, different etiologies and degrees of hypothyroidism have also been analyzed together (5). In one of the largest recent series among diabetic euthyroid individuals, the relationship between lower TSH values and MF was refuted (6). MF seems to influence TSH only in hypothyroid patients with or without levothyroxine treatment.
In the present study we aimed to add more information about the possible interaction of MF with levothyroxine requirements. We chose patients who underwent a total thyroidectomy to remove potential interactions between endogenous thyroid hormone production and TSH. This novel approach should allow us to draw more reliable conclusions.
Patients and Methods
We conducted a retrospective review of the charts from all those patients who underwent total thyroidectomy from June 2008 to July 2011 at our institution. Patients taking confounding medications (estrogen and testosterone, iodine, propranolol, amiodarone, lithium, dopamine agonists or antagonists, somatostatin analogs, steroids, phenytoin, carbamazepine, sertraline, rifampin, bile acid sequestrants, antacids, and raloxifene); patients affected with serious chronic medical conditions; and pregnant or lactating women were excluded. Patients were divided into two groups depending on MF use: the non-MF group included patients, with or without diabetes mellitus type 2, not taking MF; the MF group included patients with diabetes mellitus type 2 taking MF. The following variables were compared in both groups: sex, age, body height, body weight, indications for thyroid surgery, specimen pathology report, levothyroxine dose, last TSH value and free T4, type of DM, and antidiabetic medication. Data were collected before surgery and 3 months afterward or until replacement levothyroxine dose was properly adjusted (until TSH was <5 mIU/L and free T4 within the reference range). TSH was measured using a third-generation ultrasensitive immunochemiluminometric assay (Immulite 2500; Siemens Healthcare Diagnostics), with a sensitivity of 0.004 mIU/L (laboratory reference range 0.4–4 mIU/L). Free T4 was also determined with an immunochemiluminometric assay from the same manufacturer, with a sensitivity of 0.3 ng/dL (laboratory reference range 0.7–1.6 ng/dL). Continuous variables were summarized as mean (SD) or median (Q1–Q3), and categorical variables were summarized as proportions. Statistical analysis was performed using the χ2-test for categorical variable analysis, and by the Student's t-test and Mann–Whitney U-test to compare continuous variables between groups. Predictors that achieved a p-value <0.05 in bivariate analysis were assessed for inclusion in the multivariate model. All tests were two-tailed. A p-value <0.05 was considered to be statistically significant.
Results
Among 244 total thyroidectomies performed, 192 met the inclusion criteria for the present study. The reasons for exclusion of 52 patients were the following: insufficient data for analysis (patients moved to another place or thyroid hormones were not available), TSH or free T4 were out of the reference range at the moment of the study, or the patients were taking cofounding medications cited above.
There were 127 patients with nonmalignant thyroid diseases (mainly multinodular goiter and Graves' disease), and in 65 patients the surgical indication was differentiated thyroid cancer (DTC). All patients with DTC received suppressive doses of levothyroxine, targeting TSH to <0.1 mIU/L. Those patients were also analyzed separately. There were 159 patients in the non-MF group and 33 in the MF group. Patients in the MF group were older and heavier than those in the non-MF group (Table 1).
Mean (SD); bmedian (Q1–Q3).
MF, metformin; TSH, thyrotropin; F, female; M, male; DTC, differentiated thyroid cancer.
TSH levels did not differ significantly between the groups: 0.67 (0.11–2.81) mIU/L in the non-MF group and 0.80 (0.11–4.28) mIU/L in the MF group (p=0.46). The median TSH among DTC patients was 0.08 (0.015–0.66) mIU/mL, whereas those with benign diseases maintained a serum TSH level of 1.31 (0.29–4) mIU/L. Free T4 was similar among the non-MF [1.29 (1.2–1.4 ng/dL)] and the MF group [1.33 (1.1–1.59) ng/dL)] (p=0.9). There was no difference in total levothyroxine dose between the groups: 114 (100–150) μg/day in the non-MF group versus 125 (100–142) μg/day in the MF group (p=0.9). Patients taking MF were significantly heavier than those in the non-MF group [79.3 (13.9) vs. 70.2 (13.5) kg; p=0.001]; therefore, we calculated a weight-adjusted dose of levothyroxine. This variable showed a significant difference: 1.66 (1.38–2.08) μg/kg/day in the non-MF group versus 1.53 (1.26–1.70) μg/kg/day in the MF group (p=0.010). Levothyroxine related to body mass index (BMI) maintained this difference (p=0.012).
In the subanalysis of DTC patients, the levothyroxine dose was substantially higher in DTC patients than in patients with benign disorders, in order to reach a suppressive level. Overall DTC patients took 142.9 (25) μg/day, whereas patients without cancer needed only 109.7 (21) μg/day. Among patients with DTC, the 56 patients without MF took a median levothyroxine dose per kilogram of 2.11 (1.75–2.5) μg/kg/day, whereas the 9 patients on MF took 1.57 (1.44–2.12) μg/kg/day (p=0.05).
According to those data in the bivariate analysis, a multivariate logistic regression analysis was constructed in which the weight-adjusted dose of levothyroxine was entered as a dependent variable, whereas levels of TSH, age, BMI, sex, type of thyroid disease, and MF treatment were included as covariates. In that analysis, only age (p<0.001), BMI (p<0.001), and type of thyroid disease (p<0.001) retained significance (Fig. 1). Thus, MF treatment (p=0.4) lost its significance.
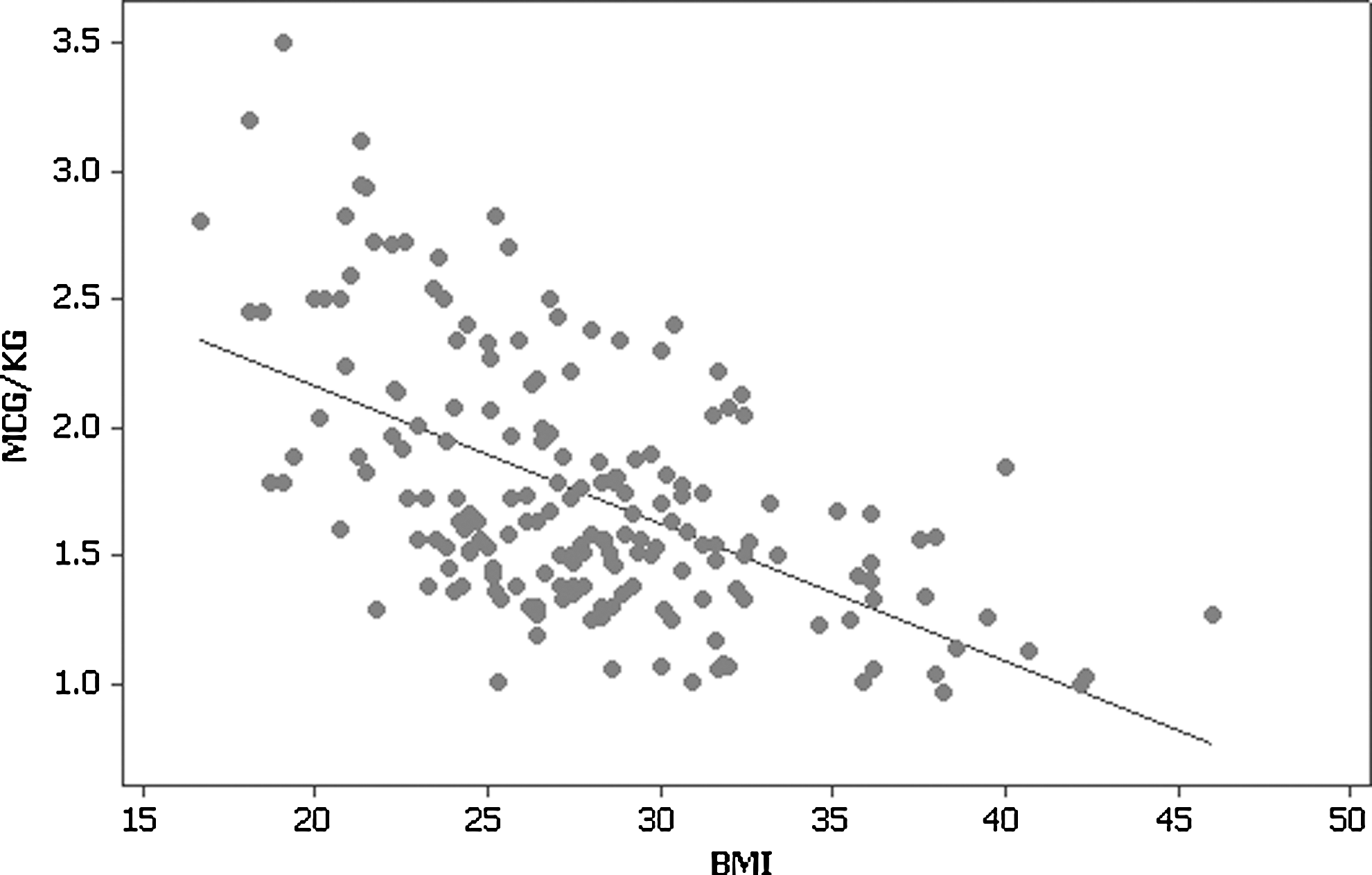
Correlation between levothyroxine dose per weight in kilograms (μg/kg) and body mass index (BMI). Multivariate logistic regression analysis: R 2=0.32.
Discussion
We found a difference in levothyroxine dose in patients with hypothyroidism depending on MF use. Our model of thyroidectomized patients, a condition not influenced by endogenous thyroid hormone production, seems to reinforce the hypothesis of a TSH-lowering effect of MF in patients requiring levothyroxine, as proposed by other authors (1). However, this difference may be related to other variables, especially age, BMI, and the TSH objective of the treatment. Nevertheless, the clinical relevance of this finding seems moderate. For instance, a patient of 70 kg weight and receiving MF would need 107 μg/day, whereas the same patient not receiving MF would need 116 μg/day.
Some authors have shown a TSH-lowering effect of MF in hypothyroid patients on levothyroxine, and in patients with subclinical hypothyroidism without treatment (4). More recently, this observation has also been reported in diabetic patients with TSH in the upper range of normality (2.51–4.5 mIU/L) (5). Accordingly, it appears that the early hypothesis postulating that MF would improve the absorption of exogenous levothyroxine appears no longer plausible.
In contrast to this “peripheral hypothesis,” it has been postulated that MF effects may have an effect on hypothalamic–pituitary signaling. Thyroid hormones negatively regulate their own production through central actions on the hypothalamic–pituitary–thyroid axis (7), mainly through T3 control of TSH gene expression. However, some circumstances, such as reduced food availability, may downregulate the hypothalamic–pituitary–thyroid axis even in the presence of normal or lower thyroid hormone levels. As a possible central target, MF inhibits the activity of the enzyme AMPK (8). AMPK plays a relevant role in nutritional sensing and feeding behavior through neuropeptides and modulation of the hypothalamic–pituitary axis. Thus, inhibitory effects mediated by T3 could be counteracted by the inhibition of central AMPK by MF. It has also been postulated that a reduction in circulating fatty acids could mediate the central effects of MF (9). In support of a central effect of MF, it is interesting to note from rat experiments that the drug enters the cerebrospinal fluid and reaches high levels. The pituitary gland is the region with the highest accumulation of MF under normal and inflammatory conditions (10).
An increased central bioavailability of thyroid hormones in patients taking metfomin could also explain lower TSH levels. For instance, MF might affect deiodinase 2 (DIO2) activity, which is found mainly in glial cells, astrocytes, and tanycytes in the mediobasal hypothalamus. DIO2 catalyzes locally the conversion of T4 to the active T3 (11). Interestingly, DIO2 polymorphism generating less T3 have been associated with some degree of insulin resistance (12); however, as of yet it remains unknown whether MF may enhance DIO2 activity, providing more T3 at the pituitary level, at least in hypothyroid patients.
Of note, some authors have not found any relationship between MF treatment and TSH. A cross-sectional study by Diez and Iglesias (6) on euthyroid diabetic patients showed that the TSH levels of patients taking MF were even higher than those without the drug. Similarly, Rotondi et al. (13) found that in euthyroid women with polycystic ovarian syndrome, TSH did not change after starting MF. On the other hand, among patients with hypothyroidism, the size of the decrease in TSH has varied between studies. In some patients, TSH falls to subnormal levels; for instance, it fell in 20% of DM patients with stable levothyroxine dose in one study (14); however, the decrease in another study was from 2.16 to 1.33 mIU/L and only 8.4% of patients had undetectable levels (5).
Possible controversies found in clinical studies may be attributed to a large degree of interindividual variability. MF is a water-soluble cationic drug that undergoes renal secretion, mainly through the organic cation transport system. Genetic variations in the genes coding for transport systems have been linked to altered pharmacodynamic and pharmacokinetic responses to the drug. Moreover, other factors such as age, sex, and comorbidity may affect MF variability (15).
In our study, the multivariate analysis revealed that subjects with greater BMI and older patients do need lower amounts of levothyroxine per kilogram. This may be a reflection of the different body composition in these populations, probably showing proportionally less lean body mass. Consistent with this notion, Santini et al. (16) demonstrated through DEXA studies that the levothyroxine dose was positively correlated mainly with lean body mass (r=0.66). Thus, BMI and older age, both greater in the MF group, would be confounding variables in our study, giving the impression that the weight-based levothyroxine dose was lower when taking the drug.
A limitation of our study is that the TSH level was not evaluated in each patient before MF introduction. Therefore, we cannot quantify the drop in TSH while on the drug; however, as noted in isolated patients from our cohort within this study protocol, starting MF was not associated with an evident fall in TSH.
In conclusion, our study indicates that thyroidectomized diabetic patients receiving MF treatment need lower doses of levothyroxine per weight than those without MF. However, advanced age and obesity could explain the lower levothyroxine requirement in patients on MF. Therefore, careful studies have to be carried out regarding the influence of body composition on levothyroxine dose in patients taking MF.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.