
Abstract
Background:
Anaplastic thyroid carcinoma (ATC) is a rare, aggressive malignancy with a median survival of five months. Multimodality treatment is associated with some improvement in survival, but patients are only infrequently curable. Although β-hCG secretion has been reported in many neoplasms, it has never been described in ATC. The objectives of this study were to report a case of β-hCG–secreting ATC and to study the expression and significance of β-hCG and PAX8 in an institutional cohort of ATC.
Methods:
The sentinel case was characterized and then immunohistochemistry was performed for β-hCG and PAX8 on 30 ATC patients. Clinical follow-up was obtained by chart review.
Results:
The sentinel patient with β-hCG–secreting ATC had a dramatic response to chemotherapy and radiation. After surgical excision of residual disease, the patient developed a regional recurrence of differentiated thyroid carcinoma at 18 months. However, she is now, 30 months after initial therapy, with no evidence of disease and no detectable serum β-hCG or thyroglobulin. Five of the 30 (17%) total ATCs were positive for β-hCG and 18 (60%) for PAX8. Outcomes for the β-hCG–positive cases were not significantly different from those for negative ones. However, none of the other four β-hCG–positive ATC patients received treatment with either chemotherapy or radiation. Interestingly, PAX8 positivity correlated with statistically significantly better overall survival (p=0.019).
Conclusions:
β-hCG is expressed in a minority of ATCs. Although only a single case in the study had diffuse immunohistochemical expression, the response it showed to aggressive multimodality therapy and the resulting favorable outcome suggest that β-hCG–positive ATC may be a unique tumor subtype, or possibly even a unique entity. PAX8 is a useful marker of ATC and may be helpful in the differential diagnosis with other malignant neoplasms.
Introduction
A
The clinical presentation is typically a rapidly growing, markedly infiltrative neck mass with hoarseness, dysphagia, vocal cord paralysis, pain, and/or dyspnea. The median survival is usually less than six months after diagnosis (4,6). Multimodality treatment with surgery (for resectable disease), radiation, and chemotherapy is associated with improved survival, but patients are only very infrequently curable (6 –9). Recently, we identified what we believe is the first case of a β-hCG–secreting ATC. The patient's serum β-hCG was elevated at diagnosis, and the tumor responded dramatically to chemotherapy and radiation. It regressed extensively and was subsequently surgically resectable. The patient is alive and disease-free over two years after initial therapy.
Although β-hCG secretion has been reported in many neoplasms, particularly carcinomas (10 –16), including being detectable in the serum in a minority of them, it has not been described in ATC. In addition, PAX8, an immunohistochemical marker of renal, ovarian, and thyroid carcinomas (17 –19), has been described as a potentially useful (as well as quite sensitive) marker for ATC (19,20). It has been shown to be consistently detectable by immunohistochemistry in the majority of differentiated thyroid carcinomas, but it has not been extensively studied in ATC. Its expression has not been correlated with patient outcomes.
The aims of this study were to report the index case with a β-hCG–secreting ATC, and, given its apparently unique clinical features, to determine the frequency of β-hCG expression in a larger cohort of ATC. Further, we sought to characterize the clinical and pathologic features of the positive tumors and to investigate if the expression of PAX8 was related to these cases or to patient prognosis.
Materials and Methods
After characterization of the sentinel β-hCG–secreting ATC case, with Human Research Protection Office approval, an additional 29 cases of ATC were retrieved from Barnes Jewish Hospital and Washington University pathology department files. Cases were identified by a pathology database keyword search using the terms “thyroid” and “anaplastic carcinoma” or “undifferentiated carcinoma.” Cases were included if they fulfilled the following criteria, derived from the World Health Organization definition (1): (i) the majority of the tumor had to be undifferentiated or anaplastic; (ii) there was convincing evidence of epithelial differentiation histologically or, if not, then confirmation of such by either pancytokeratin, thyroglobulin, or thyroid transcription factor 1 immunohistochemistry. The ATCs were subtyped into the following (1): (i) squamoid, (ii) spindled, (iii) pleomorphic, (iv) carcinosarcoma with cartilage or bone formation or other histologically defined sarcoma differentiation, (v) paucicellular, (vi) lymphoepithelioma-like, and (vii) giant cell (3). More than one subtype was allowable in an individual tumor. The presence of a coexisting differentiated carcinoma component was assessed by routine histologic examination or, in biopsy only cases, by clinical history of prior differentiated carcinoma, with tumors defined by traditional World Health Organization definitions. Clinical follow-up information was obtained by chart review.
Immunohistochemistry
Immunohistochemistry was performed on formalin-fixed, paraffin-embedded 4 μm tissue sections on a Ventana Benchmark LT automated immunostainer (Ventana Medical Systems, Inc., Tucson, AZ) for PAX8 (Proteintech Group, Inc., Chicago, IL; product # 10336-1AP; rabbit polyclonal; dilution 1:80; incubation 40 minutes at 37°C) and for β-hCG (Ventana Medical Systems, Inc.; product # 760-2650; rabbit polyclonal; prediluted; incubation 16 minutes at 37°C). Both immunostains utilized the standard Ventana CC1 mild solution (1 mM EDTA buffer at pH 8.0) for antigen retrieval. For PAX8, a case of renal cell carcinoma, clear cell type, served as the positive control and a slide that was not incubated with primary antibody as the negative control. For β-hCG, normal placenta was used as the positive control, and then a slide that was not incubated with primary antibody as the negative control. The immunostained slides were reviewed by three study pathologists (N.B., R.D.C., J.S.L.), and staining in both the ATC and the differentiated carcinoma component (when present) was characterized. Staining intensity for β-hCG was categorized as weak, moderate, or strong. In addition, the staining distribution was categorized in quartiles as follows: 0, negative; 1+, 1–25% of tumor cells positive; 2+, >25–50%; 3+, >50–75%; 4+, >75%. PAX8 staining was characterized as positive or negative without further stratification based on the presence of any definitive tumor cell nuclear staining. Discrepancies were resolved by consensus review.
Statistics
Statistical analysis was performed using GraphPad Prism 6 (GraphPad Software, Inc., La Jolla, CA). Associations between the categorical clinical and pathological features were assessed using two-tailed Fisher's exact tests. Age, as a continuous variable, was simply divided at the median into two separate groups for analysis. Overall survival was defined as the time between the initial surgical pathology diagnosis to the date of death. Survival curves were determined by the Kaplan–Meier method and statistically analyzed using the Gehan–Breslow–Wilcoxon method.
Results
β-hCG–positive sentinel patient
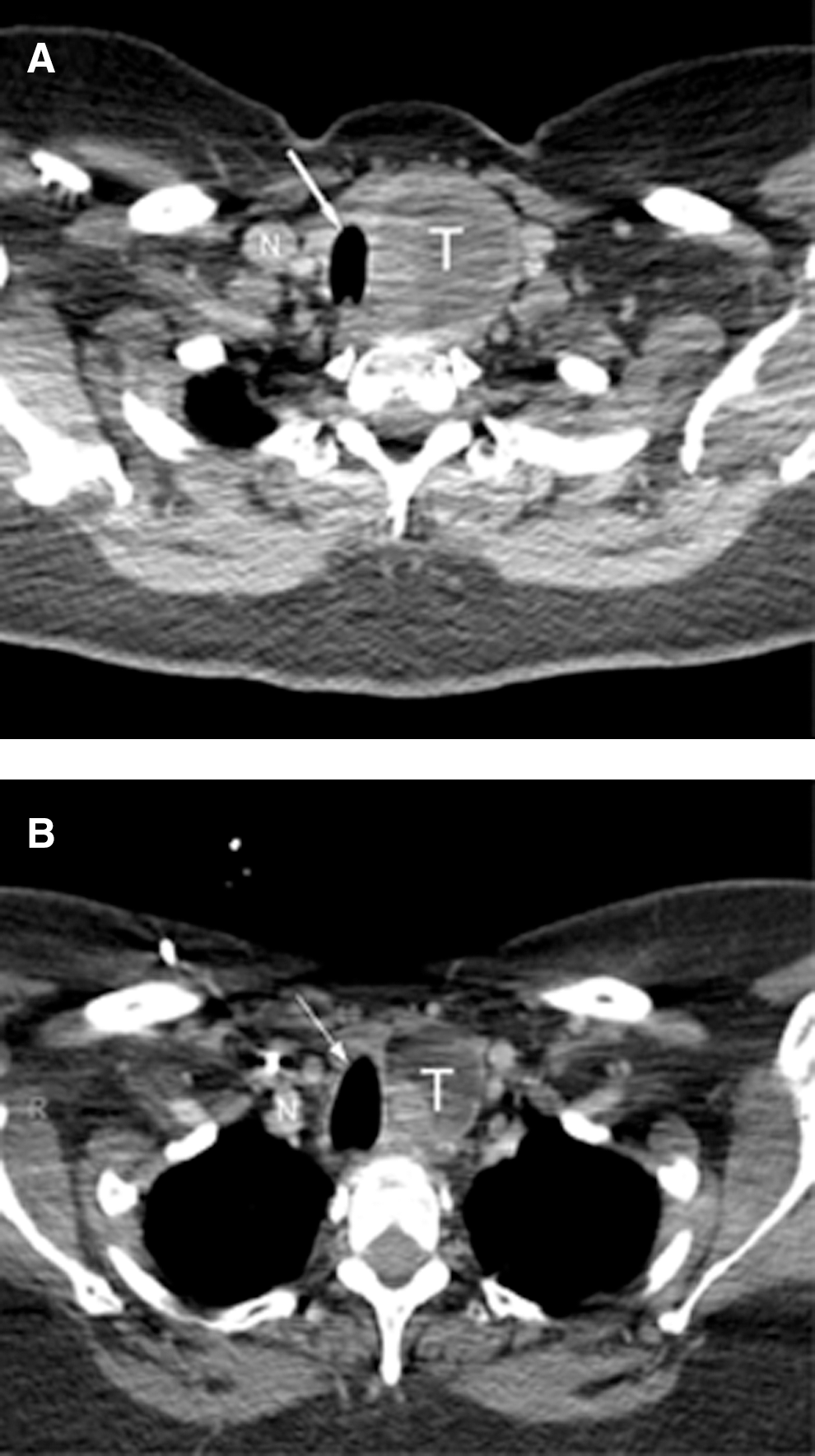
The patient is a 54-year-old woman who presented to an outside hospital in 2010 with a rapidly enlarging neck mass, which on examination and imaging was arising from the left thyroid lobe. Preoperatively, a serum β-hCG level was drawn in order to rule out pregnancy. When it returned as elevated, the outside surgeon declined to operate because of concern for possible pregnancy. She sought further treatment at Washington University in St. Louis. At presentation, she had mild neck pain but had no dysphagia, dyspnea, or hoarseness. Further sonographic and computer tomographic imaging showed a large, heterogeneously enhancing, unresectable left thyroid mass measuring approximately 6.2 cm×4.8 cm×4.5 cm (Fig. 1). The mass replaced almost the entire left thyroid lobe. Although the airway was deviated to the right, there was no overt tracheal invasion. Additional hypoechoic, subcentimeter nodules were seen in the right thyroid lobe. Left cervical lymphadenopathy was also present with the largest lymph node seen lateral to the internal jugular vein in the mid neck measuring 1.6 cm. Serum β-hCG was 48.0 IU/L (normal <5 IU/L) and serum calcitonin was <5 pg/mL (within normal limits). She was postmenopausal and an examination by her obstetrician revealed no evidence for pregnancy.
Pretreatment
Fine-needle aspiration of the left thyroid mass was positive for a high-grade malignancy consistent with ATC. A subsequent needle core biopsy showed a high-grade malignant neoplasm composed of sheets of pleomorphic cells with intervening hyalinized stroma (Fig. 2). The tumor cells were poorly cohesive and showed epithelioid to spindled features. Nuclei were angulated and hyperchromatic, and there were scattered prominent nucleoli. There was brisk mitotic activity and extensive necrosis. A panel of immunohistochemical stains performed at the time of diagnosis showed the tumor cells to be strongly and diffusely positive for pancytokeratin, vimentin, and β-hCG (Fig. 2). The tumor cells were negative for CD45, placental alkaline phosphatase, Oct3/4, inhibin, calcitonin, CD31, and thyroid transcription factor 1. The diagnosis of ATC was rendered after choriocarcinoma was ruled out by the lack of any multinucleated cell (syncytiotrophoblastic) component and also by the lack of inhibin or placental alkaline phosphatase expression.
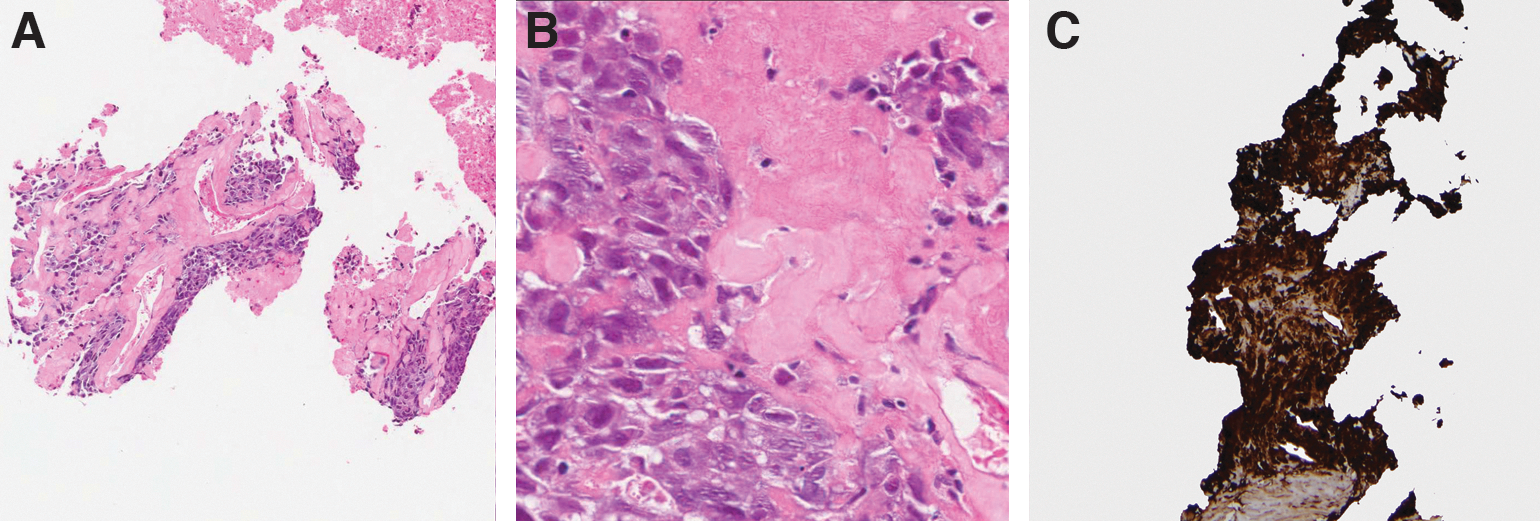
Histologic features of the index β-hCG–positive anaplastic thyroid carcinoma on needle biopsy.
The patient received intensity-modulated radiation therapy to 61.2 G in twice daily fractions and taxol chemotherapy of 40 mg/m2 weekly for 5 weeks. After a dramatic clinical response with the tumor decreasing in size by more than one-third and going from fixed to mobile, the tumor became surgically resectable. The serum β-hCG level remained elevated, concerning for persistent viable disease. Resection of the entire thyroid gland and left neck regional lymph nodes showed a 4.7 cm×3.8 cm×3.5 cm extensively necrotic tumor in the left lobe (Fig. 3A). Less than 25% of the tumor was still viable, and it consisted of a pleomorphic, spindled, and epithelioid neoplasm with large nuclei with vesicular chromatin and prominent nucleoli. Occasional mitotic figures were seen. The tumor was present in ill-defined sheets, and, interestingly, did not show an infiltrative growth pattern, having a relatively defined periphery with a pseudocapsule (Fig. 3B). The margins of resection were negative for tumor. Immunohistochemistry was performed and showed the tumor cells to be strongly and diffusely positive for cytokeratin 7 and β-hCG but negative for S100. A component of well-differentiated carcinoma with large cells with abundant, eosinophilic cytoplasm and round nuclei with prominent nucleoli was also present, features of Hürthle cell carcinoma (Fig. 3C). The left neck lymph node dissection showed metastatic Hürthle cell carcinoma in 1 of 32 lymph nodes, but no metastatic ATC.

Gross and histologic features of the index β-hCG–positive anaplastic thyroid carcinoma on surgical resection.
A postoperative β-hCG level was <5 IU/L. The patient recovered well after surgery and then, based on pathology results, received 100 mCi of radioactive iodine with the post-treatment scan showing expected thyroid bed uptake only. She remained well and disease-free until 18 months postsurgery, when she developed a positive thyroglobulin level of 7 ng/mL with a withdrawal TSH level of 36 mU/L. A 5 mCi iodine scan using 131I during hormonal withdrawal revealed no uptake, but a subsequent fluorodeoxyglucose positron emission tomography/computed tomography scan showed a left paratracheal mass. Her β-hCG level continued to be <5 IU/L, however. Fine-needle aspiration showed a pleomorphic carcinoma, which was favored to be recurrent ATC. Subsequent surgical resection of the mass showed two 0.4 cm foci of Hürthle cell carcinoma in follicles and with extensive fibrosis and cystic change. The nuclei were vesicular with prominent nucleoli but no significant mitotic activity. The nuclear atypia was felt to be treatment related. There was no evidence of ATC, and the resection margins were tumor-free. She is now alive and disease-free at 30 months after her initial diagnosis. The quantitative serum β-hCG level continues to be undetectable.
Clinicopathologic features of the tumor cohort
Clinicopathologic features of the cases are presented in Table 1. The cases consisted of the following types: squamoid (15/30 [50%]), spindled (16/30 [53%]), pleomorphic (10/30 [33%]), lymphoepithelioma-like (1/30 [3%]), and giant cell (7/30 [23%]). There were no carcinosarcoma or paucicellular types. There was a coexisting differentiated carcinoma component in 19 of the 30 cases (63%). These were as follows: papillary carcinoma (13/30 [43%]), insular carcinoma (2/30 [7%]), follicular carcinoma (1/30 [3%]), Hürthle cell carcinoma (1/30 [3%]), and unknown/not otherwise specified (2/30 [7%]).
Boldface indicates that p<0.05 is statistically significant.
β-hCG–positive vs. negative.
PAX8-positive vs. negative.
n/a, not available; SD, standard deviation; IMRT, intensity modulated radiation therapy.
Immunohistochemistry
Immunohistochemistry results are presented in Tables 1 and 2. β-hCG expression was present in 5 of 30 cases (17%), but only the sentinel case showed strong, diffuse staining. The remaining positive cases showed either strong β-hCG staining in less than 25% of cells, or just moderate intensity staining in up to 75% of the cells (Fig. 4). No expression was detected in any of the differentiated thyroid components. β-hCG expression was not significantly associated with any of the other clinical or pathologic variables. PAX8 staining was present in the ATC component of 18 of 30 (60%) cases, including 2 of the 5 (40%) β-hCG–positive cases. The differentiated component was positive for PAX8 in all 14 cases that had one. The index case, with strong and diffuse β-hCG expression and positive serum β-hCG, was negative for PAX8. There was no correlation between β-hCG and PAX8 expression (p=0.36). PAX8-positive patients were statistically significantly younger than the PAX8-negative patients (61.8±9.8 vs. 71.3±9.0 years, p=0.01) and more likely to have undergone surgical treatment (p=0.018).
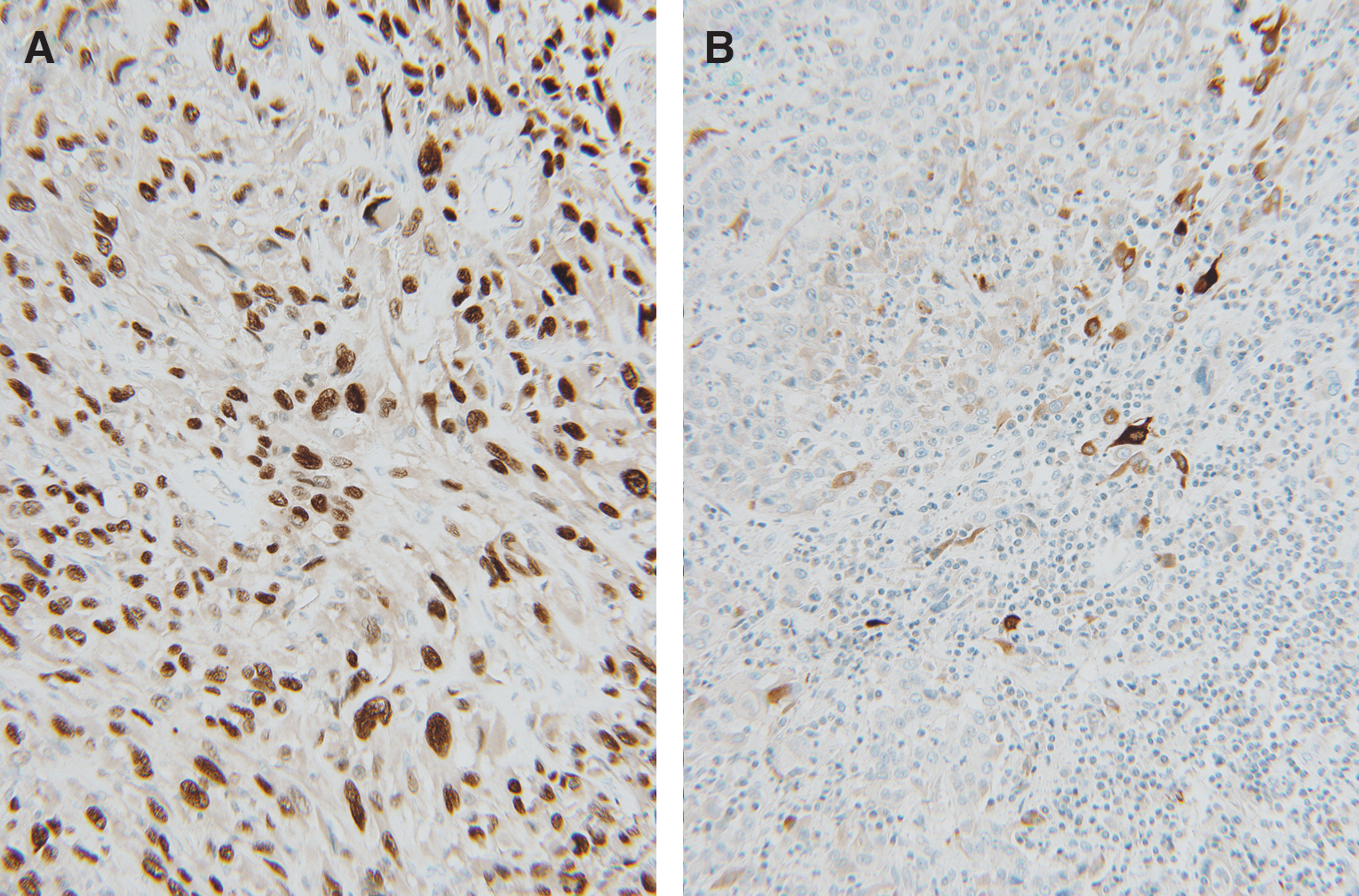
Representative PAX8-positive and β-hCG–positive anaplastic carcinoma cases from the additional cohort.
Sentinel case; patient alive and without evidence of disease.
No follow-up data obtainable; patient lost to follow-up.
+, positive staining (in quartiles).
Survival analysis
Twenty-seven of the 29 (93%) patients with clinical data available died during the follow-up period, at a median of 3.3 months, and all with progressive disease. Follow-up of the five β-hCG–positive patients showed that only the index case patient survived. However, the remaining four patients did not receive multimodality therapy. Three of four underwent surgical resection but none were treated with chemotherapy or radiation therapy. These four patients all died at a median of 2.7 months (82 days). The median survival of the β-hCG–positive cases (106 days) was comparable to the β-hCG–negative ones (110 days) and there was no difference in univariate survival analysis by β-hCG expression (p=0.63) (Fig. 5). Interestingly, PAX8-positive patients had improved overall survival (median 4.9 months vs. 2.0 months, p=0.019). Among the major clinical and pathologic features (Fig. 5), patients who received surgical treatment had statistically significantly improved overall survival (p=0.0073), and there was a trend toward improved survival by patient age (p=0.12), but this was not statistically significant.
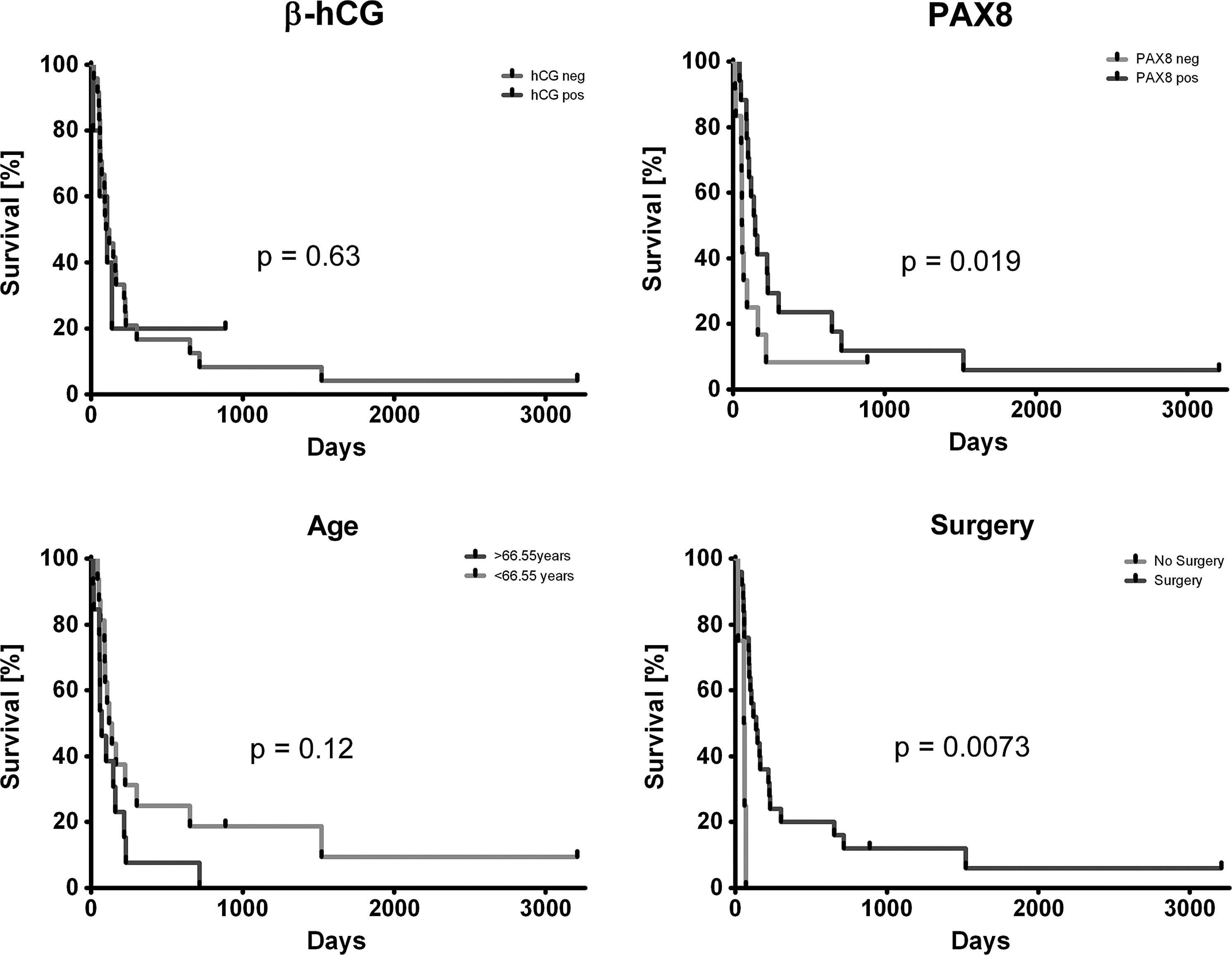
Univariate overall survival curves for β-hCG and PAX8 expression, patient age, and surgical treatment.
Discussion
ATC is one of the most aggressive human cancer types. Although some treatments have shown improvement in survival, the studies are retrospective and generally consist of small numbers of patients. Surgical resection, if feasible, does appear to be associated with improved survival (8,21). Radiation, with or without chemotherapy, also improves locoregional disease control and survival (7,8). However, it is distinctly uncommon for patients to be cured of their disease. Despite the emergence of small molecule inhibitors and monoclonal antibodies in modern cancer care, there are still no targeted therapies proven to be effective for ATC.
Our study is the first to report a β-hCG–secreting ATC and, further, is the first to characterize a cohort of ATC for immunohistochemical expression of β-hCG. This tumor, unlike typical ATC, was highly treatment-responsive and has had a favorable outcome at two and a half years of follow-up. The anaplastic carcinoma component, although surgically unresectable at presentation, responded dramatically to intensity modulated radiation therapy and taxotere chemotherapy. It became surgically resectable and since that time, the patient has been alive and free of ATC, although she did have a nodal recurrence of Hürthle cell carcinoma 18 months after surgery, which was treated effectively. The tumor secreted β-hCG detectable in the serum, which persisted after chemoradiation but became nondetectable after the first surgical procedure. This confirms that the source of the β-hCG in the serum was the ATC. Quantitative serum β-hCG levels have been obtained every 6 months, which have continued to be undetectable.
In the follow-up study of 29 more ATC cases, the four additional β-hCG–positive patients all rapidly died of disease despite three undergoing surgical resection. However, none of them was subsequently treated with either chemotherapy or radiation. Although it is difficult to draw conclusions from one case, strongly β-hCG–positive ATC, particularly as manifested by positive serum β-hCG levels, may be a unique entity with a favorable outcome. The diagnosis of primary thyroid choriocarcinoma was strongly considered and ruled out for several reasons: (i) the morphology lacked the biphasic cyto- and syncytiotrophoblastic cells seen with choriocarcinoma; (ii) there was a differentiated thyroid carcinoma component intimately associated with the undifferentiated carcinoma; (iii) the tumor lacked expression of inhibin, a very sensitive marker of trophoblastic differentiation, and also lacked expression of placental alkaline phosphatase; (iv) a choriocarcinoma would have manifested much higher serum β-hCG levels, especially relative to the large size of the thyroid mass; and, finally, (v) no primary thyroid choriocarcinoma has ever been described.
PAX8 immunohistochemistry was also performed, and 18 of the 30 cases showed staining in the ATC component of the tumors. This is comparable to the emerging literature on this marker in thyroid cancer (19,20) and again shows that PAX8, which appears to be quite specific for thyroid follicular differentiation, at least among head and neck tumors, is a good marker for ATC in cases where the diagnosis may not be straightforward. PAX8 is much more consistently expressed in ATC than thyroglobulin and thyroid transcription factor 1, the other markers of follicular differentiation, which are only expressed in less than 25% of cases (19,22). Interestingly, the expression of β-hCG and PAX8 does not appear to be related. Only 2 of the 5 β-hCG–positive cases were positive for PAX8, and the index case with diffuse β-hCG expression and known elevated serum levels was negative, despite coming from a background of Hürthle cell carcinoma. Ours is the first study to find PAX8 expression to be prognostic. The patients with PAX8-positive ATC had statistically significantly better overall survival in univariate analysis. This is tempered by the fact that PAX8-positive tumors were more frequent in younger patients and in patients undergoing surgical treatment, both of which were also associated with improved survival. In particular, patients with ATC who have been candidates for surgical resection and multimodality therapy have been shown to have improved survival.
What is the significance of β-hCG in ATC? This index case suggests that β-hCG–secreting ATC may be a unique entity and that it may be associated with more treatment-responsive disease. However, it is just a single case. Since patients with ATC are not routinely tested for β-hCG, either by serum or urine testing or by tumor immunohistochemistry, the frequency of this association is unknown. Since hCG has been shown to be expressed (and sometimes secreted in the circulation) by nontrophoblastic carcinomas at various sites [most notably the urinary bladder (10) and lung (16)], the current case may just be a rare example of this phenomenon in ATC. Interestingly, β-hCG production has been associated in some studies with more aggressive clinical behavior (16), which was definitely not the finding in our case. Further studies and observation for additional cases of ATC that express β-hCG will be critical for ascertaining both the frequency of this association and if it truly bears reproducible clinical significance.
Footnotes
Acknowledgments
The authors would like to acknowledge Jianping Li, BS, Autumn Watson, BA, and Neha Dahiya, MD, MBA, of the Anatomic and Molecular Pathology Core Laboratory for their expert technical assistance with the immunohistochemical staining.
Author Disclosure Statement
No competing financial or other interests exist for the authors.