
Abstract
Background:
Medullary thyroid cancer (MTC) is a calcitonin (Ct)-secreting tumor of the parafollicular or C cells of the thyroid gland. Higher serum Ct levels are associated with larger tumor size, distant metastases, and prognosis. We report herein a case of prostate and multiple bone metastases of nonfamilial MTC with mildly elevated Ct levels.
Patient Findings:
A 73-year-old man who was found to have a 2.5 cm MTC in the left thyroid lobe with cervical lymph node metastases presented with confused mental status because of severe hypercalcemia (albumin-modified serum calcium concentration 15.2 mg/dL) associated with multiple bone metastases. Prostate biopsy was performed because the patient had frequent urination with mildly elevated serum prostate-specific antigen (5.297 ng/mL). Histologically, the prostate was diagnosed as MTC metastasis, forming a tissue architecture closely resembling the previously diagnosed MTC, and the cells were positive for Ct, carcinoembryonic antigen, and thyroid transcription factor 1. Although the patient had multiple MTC metastases, basal and calcium-stimulated serum Ct levels were not significantly elevated, measuring 22.7 pg/mL (normal <10 pg/mL) and 22.1 pg/mL, respectively.
Conclusions:
A chronic hypercalcemic state may exhaust Ct reserves and diminish the Ct response to an acute intravenous calcium injection. Therefore, the Ct level of a patient in a hypercalcemic state should be carefully interpreted. To our knowledge, this is the first reported case in the literature in which serum Ct levels were not significantly increased when associated with hypercalcemia, and an MTC metastasis to the prostate.
Introduction
M
Case Report
A 73-year-old man presented with a confused mental status. Recently, he had complained of general weakness and poor food intake for one month. He was then found to have a 2.5 cm MTC in the left thyroid lobe with cervical lymph node metastases by core needle biopsy (Fig. 1). He had aggravated symptoms of weakness and back pain, and was bedridden for one week. He had a history of type 2 diabetes mellitus and hypertension. His family history was unremarkable regarding any endocrinological or thyroid disease.
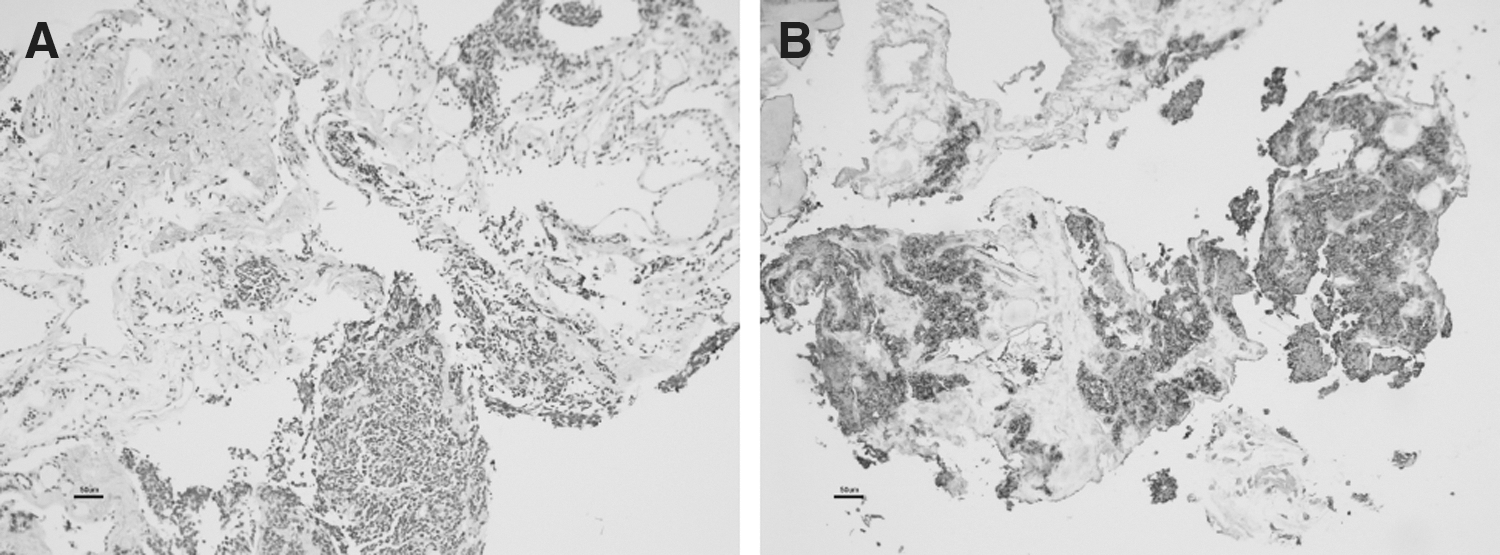
Thyroid core needle biopsy.
In laboratory findings, thyroid function and liver and renal functions were within normal limits, and hypercalcemia was revealed; his albumin-modified serum total calcium was 15.2 mg/dL and the ionized calcium was 3.22 mEq/L. Severe hypercalcemia was controlled with a saline infusion and intravenous (i.v.) pamidronate, and the patient's mental ability and calcium normalized.
Further laboratory investigation revealed a normal serum phosphorus and an undetectable serum intact parathyroid hormone. The parathyroid hormone-related protein level was 1.3 pmol/L (reference range 0–1.0). Basal and calcium-stimulated serum Ct levels were 22.7 pg/mL (reference range <10) and 22.1 pg/mL, respectively. To exclude the possibility of a high-dose hook effect, the laboratory was asked to reassay the samples using serial dilutions. At 1:10 and 1:100 dilutions, his basal Ct levels did barely change. The basal serum procalcitonin level was 2.37 ng/mL. The serum carcinoembryonic antigen (CEA) level was 8.66 ng/mL (reference range <4.7) and the prostate-specific antigen (PSA) was 5.297 ng/mL (reference range <4). Urinalysis showed microscopic hematuria, and 24-hour urine catecholamines were normal.
Thyroid ultrasonography showed two hypoechoic nodules in both thyroid lobes, the largest in the left upper lobe measuring 1.7 cm×1.3 cm×2.5 cm, which was diagnosed as MTC in a private hospital by core needle biopsy. Abdomen, chest, and neck computed tomography showed multiple small lung nodules with enlarged bilateral paratracheal, level IV, mediastinal and hilar lymph nodes, and lower thoracic vertebral metastases. A brain magnetic resonance imaging showed small osteolytic nodular lesions at the left frontal and right temporal bone. A 18F-fluorodeoxyglucose positron emission tomography scan showed increased uptake of 18F-fluorodeoxyglucose in the thyroid mass, cervical and para-aortic lymph nodes, and multiple bones (sternum, vertebrae, femur, and pelvic bone; Fig. 2). The patient developed severe hypercalcemia because of osteolytic bone metastases, which was aggravated by his bedridden status.
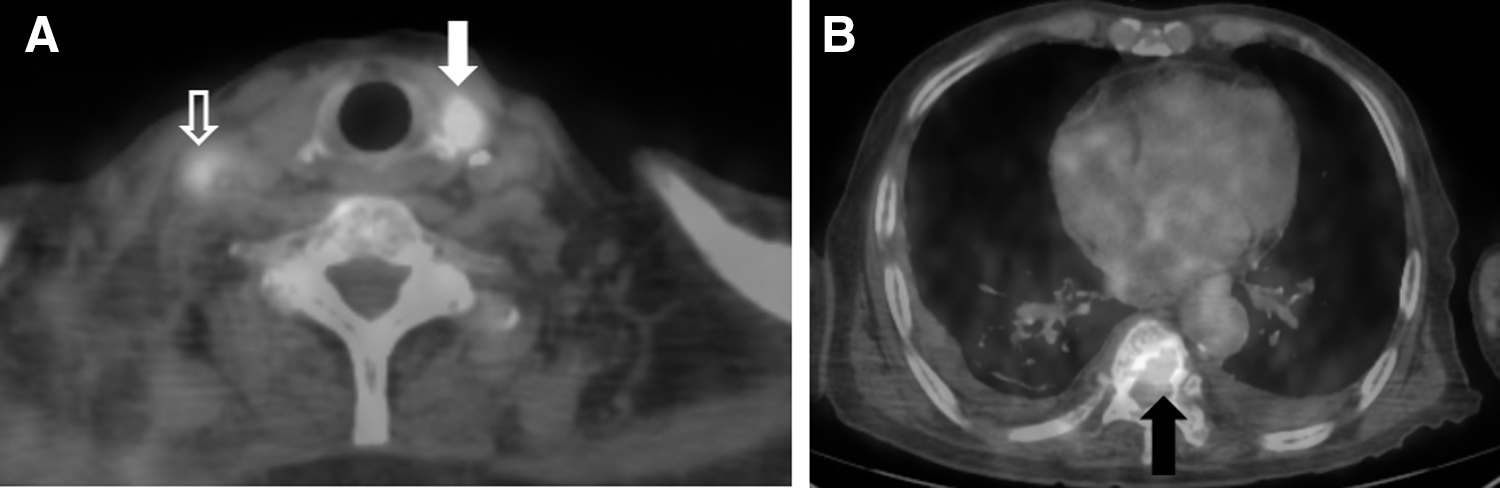
Positron emission tomography images show strong focal uptake in
A prostate biopsy was performed to determine the nature of the prostate lesion given that the patient had multiple osteolytic bone metastases, frequent urination symptoms, and a mildly elevated serum PSA (5.297 ng/mL). Histologically, the prostate lesion was diagnosed as metastatic MTC, forming a tissue architecture closely resembling the previously diagnosed MTC. The cells were positive for Ct, CEA, thyroid transcription factor 1 (TTF-1), cytokeratin, synaptophysin, and CD57 (Fig. 3). Immunohistochemical staining for P504s, p63, CD56, high-molecular-weight cytokeratin, and neurofilament were negative.
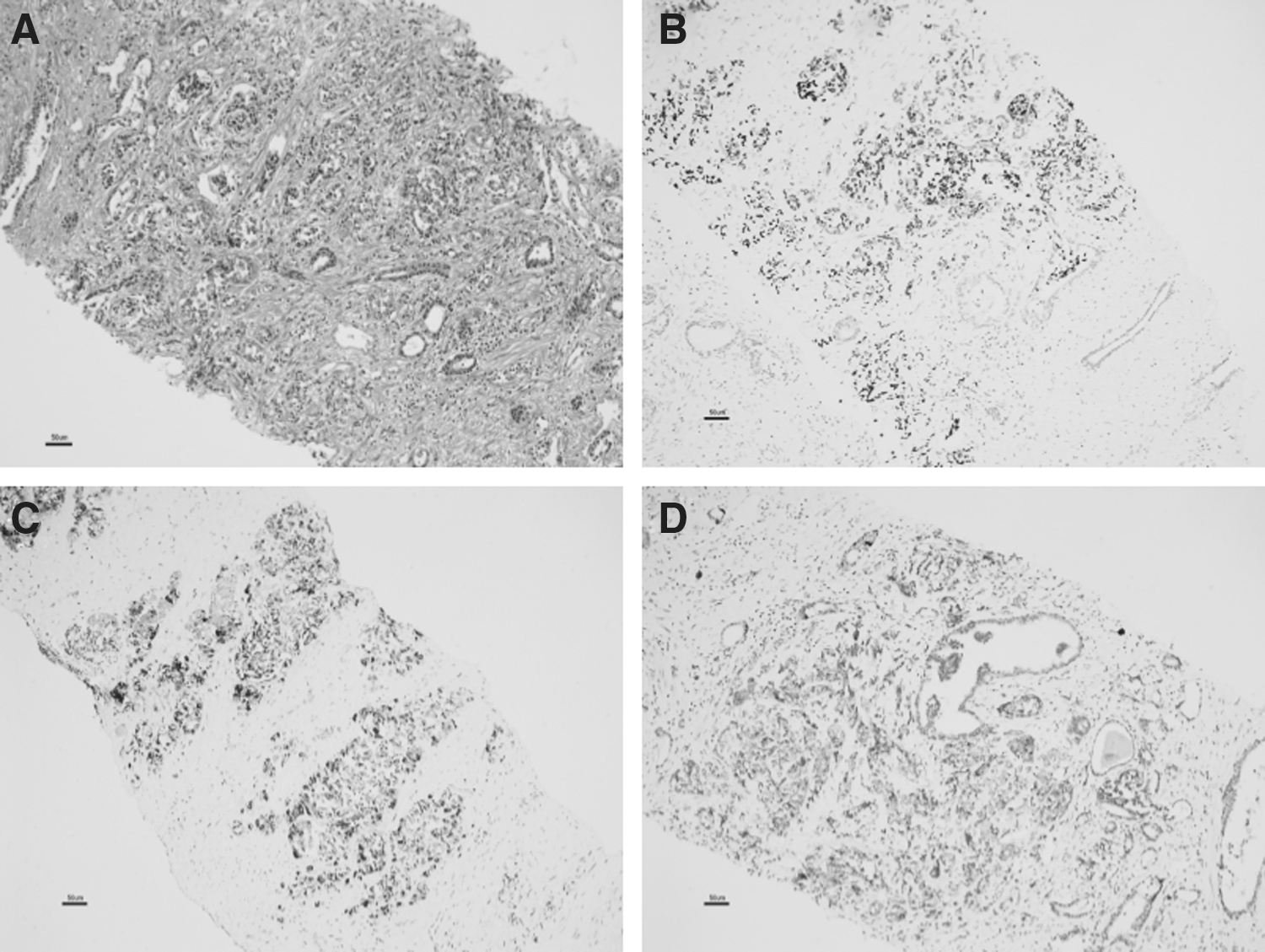
Prostate biopsy.
On admission, he was totally bed-ridden, mentally confused, and fully dependent on care (Eastern Cooperative Oncology Group performance score 4). Treatment with saline infusion, i.v. bisphonate, and nutritional support normalized his serum calcium level, and the patient showed some improvement of his general condition, but he remained disabled because of generalized bone pain and his performance score was still 3 at best. We considered a trial with a multikinase inhibitor because conventional chemotherapy has not shown efficacy in advanced MTC and has considerable toxicity. Unfortunately, he and his family members declined further treatment because of his condition and the advanced age of the patient, and he was lost to follow-up.
Discussion
In our case, a patient who was found to have MTC and regional lymph node metastases presented with confused mental status because of hypercalcemia, which resulted from osteolytic bone metastases. He was found to have an MTC metastasis to the prostate that was confirmed by immunohistochemical staining of the biopsy samples. Although the patient had MTC with multiple metastases, his basal and stimulated Ct levels were only mildly elevated.
Metastasis to the prostate from malignancies of other organs is extremely rare and usually occurs only in advanced stages of cancer; the majority of metastases to the prostate occur typically by direct invasion from adjacent cancers such as the bladder or rectum (3,6). Metastases to the prostate are difficult to verify by routine imaging, and metastasis from MTC has not been reported to date. In our patient, a prostate biopsy was performed because he had hypercalcemia caused by multiple osteolytic bone metastases, complaints of urination difficulty, and a mildly elevated PSA. The biopsy showed a metastatic MTC lesion that was positive for Ct, CEA, and chromogranin A (CgA) immunostaining. The primary MTC was diagnosed by core needle biopsy, and only CgA immunostaining was performed, because of insufficient thyroid biopsy tissue. CgAs are proteins stored and released with peptides and amines in a variety of neuroendocrine tissues (7). CgA production and immunoreactivity is observed in approximately 80–100% of all MTC patients, and increased serum levels are found in approximately 50% (8,9). To exclude the possibility of a rare neuroendocrine tumor of the thyroid that may have a similar histological appearance with MTC and immunohistochemical expression of CgA (10,11), we performed immunostaining for TTF-1, CEA, and Ct of the prostate biopsy tissue. The primary thyroid origin of this tumor was supported by positive immunoreactivity of tumor cells for TTF-1, CEA, and Ct.
The Ct levels are highly sensitive and specific for MTC; therefore, it is a useful tool for initial diagnosis and postoperative disease surveillance (12,13). An MTC can be excluded if the basal Ct level is <10 pg/mL, whereas basal Ct levels >100 pg/mL are considered predictive of MTC. A pentagastrin or a calcium stimulation test is required for basal Ct levels between 10 and 100 pg/mL; stimulated Ct values >100 pg/mL are also considered to be predictive of MTC (14). Pentagastrin and calcium-stimulated Ct result in a Ct level increase of more than two or three times above the basal levels (4). Although pentagastrin stimulation has been shown to be superior than calcium stimulation alone (15), pentagastrin is not available in Korea. In our study, we performed the calcium stimulation test after correction of the hypercalcemia, at a basal Ct level of 22.7 pg/mL. Normally, the preoperative Ct levels significantly correlate with MTC tumor size and are predictive of metastatic disease (4). The lack of a markedly elevated serum Ct (<100 pg/mL) in patients with metastatic MTC is associated with a low risk of MTC or, very rarely, nonmetastasizing micro-MTC (size <10 mm) (16). Although our patient had a 2.5 cm MTC in the thyroid gland with multiple metastases, the stimulated Ct level was only 22.1 pg/mL, whereas the pathological specimens stained strongly positive for Ct in the metastatic tumor. Lambert et al. (5) reported that the mean maximal increase of Ct levels with the calcium stimulation test was significantly lower in patients with primary hyperparathyroidism than in normal subjects. A chronic hypercalcemic state induces an exhaustion of thyroidal Ct reserves; therefore, the Ct response to the acute i.v. calcium injection is diminished (17). However, there are no formal studies on the impact of hypercalcemia on Ct levels in patients with MTC. We suggest that a chronic hypercalcemic state in MTC could be a reason for the lack of a Ct increase in response to i.v. calcium. Disappointingly, the patient could not be followed; therefore, the Ct levels could not be evaluated after his calcium level was within the normal range.
Hypercalcemia leads to progressive mental impairment and renal failure. Cancer-associated hypercalcemia can occur because of osteolytic bone metastases with local release of cytokines (including osteoclast-activating factors), tumor secretion of parathyroid hormone-related protein, and tumor production of 1,25-dihydroxyvitamin D (18,19). Wu et al. (20) reported that the bone metastatic rate for MTC was 12% (3/25) and all cases showed osteolytic lesions on radiograms similar to the present case. Additionally, the patients with bone metastases presenting with hypercalcemia had a worse survival rate, even if they were actively treated (21).
Even though the patient did not get any additional treatment for MTC, a trial of multikinase inhibitors might have been the best therapeutic option, considering his large burden disease and his symptoms. Conventional chemotherapy employing doxorubicin and cisplatin is not recommended in advanced MTC because of limited efficacy and significant toxicity (22,23). In recent years, several multikinase inhibitors targeting rearranged during transfection (RET), epidermal growth factor receptor (EGFR), and vascular endothelial growth factor (VEGF) have been evaluated in clinical trials with some promising results. Vandetanib prolonged median progression-free survival from 19 months in the placebo arm to a predicted median of 31 months in the vandetanib arm with a manageable side effect profile (24). Vandetanib was approved by the FDA in April 2011 for the treatment of advanced symptomatic MTC. Cabozantinib prolonged progression-free survival from 4 to 11 months and was approved by the FDA in November 2012 (25). Surgical resection of the thyroid was not considered necessary, because the patient had no signs of airway or cervical compression (23). External beam radiation therapy to the painful spine metastases was considered to control bone pain, but the patient opted for conservative management.
In conclusion, MTC metastasis to the prostate has been associated with widely disseminated disease in this patient. The patient presented here is unusual because serum Ct levels were only mildly increased despite the presence of multiple metastases. Although dedifferentiation cannot be entirely excluded, we believe that this was because of his hypercalcemic state. The Ct level of a patient with hypercalcemia needs to be carefully interpreted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.