
Abstract
Background:
Patients with Graves' disease (GD) and thyroid nodules have an elevated risk of developing thyroid carcinomas, which is primarily accounted for by well-differentiated tumors. Among these tumors, certain histological variants, such as the diffuse sclerosing and tall cell carcinoma, are characterized by a more aggressive behavior. The aim of this study was to evaluate the incidence, the clinical behavior in relation to histological variants, and the outcome of papillary thyroid carcinoma (PTC) in a cohort of patients with GD who had undergone thyroidectomy.
Methods:
A total of 2188 patients who underwent total thyroidectomy participated in this retrospective, nonrandomized, population-based study at a General Hospital. Of these patients, 181 had GD. The parameters examined included the clinical characteristics of the tumor and the final pathological examination of the thyroid carcinoma.
Results:
PTC was diagnosed in 570 patients. Among the 61 with PTC GD-positive, 59.0% presented with the pure papillary variant, 19.7% with the follicular variant, 6.6% with the sclerosing variant, and 18.0% with the tall cell variant (TCV) of PTC. Among 509 PTC GD-negative, 80.6% had pure papillary variant, 9.0% follicular variant, 3.7% sclerosing variant, and 6.1% TCV. Patients with tumor size >5 and ≤10 mm demonstrated that lymph node metastasis (p=0.001) and TCV in histological examination (p=0.003) were statistically significantly associated with GD-positive PTC.
Conclusions:
The incidence of PTC in GD-positive patients is higher than that in GD-negative patients. Aggressive variants of PTC, such as the TCV, were more frequent in nodular micro-PTC. These findings suggest that prompt and meticulous evaluation of nodules in any patient with GD associated with nodular alterations must be considered.
Introduction
G
The high incidence of PTC in GD suggests that a more aggressive approach for the management of these nodules is indicated. Accordingly, certain authors have suggested that early thyroidectomy remains an appropriate treatment option for nodular GD (7).
Some studies support that differentiated thyroid carcinomas in patients with GD are more aggressive than those in euthyroid patients (8). Pellegriti et al. (9) showed that in a series of 450 Graves' patients operated on in a 12-year period, 4.7% had clinically relevant differentiated thyroid carcinomas. In another study, the cumulative risk for recurrent/progressive distant metastases was approximately threefold higher in Graves' patients than in euthyroid patients (10). However, other studies that focused on incidentally discovered PTC do not support the claim that thyroid carcinomas are more aggressive in patients with GD than in euthyroid patients (5,10).
Filetti et al. (11) have shown that thyroid-stimulating antibodies present in Graves' patients are able to stimulate the function and growth of differentiated thyroid carcinoma metastases. In addition, the autoimmune process of GD per se may affect the clinical evolution of thyroid carcinoma by altering the host immune response to the tumor (12 –14).
Some studies have reported that the increased incidence of thyroid carcinoma is primarily accounted for by well-differentiated tumors that generally have a good prognosis (15 –17). However, among these tumors, certain histological variants such as diffuse sclerosing and tall cell variant (TCV) are characterized by a more aggressive behavior. To our knowledge, it is unclear whether these variants behave more aggressively in the presence of GD. The aim of this study was to evaluate the incidence, the clinical behavior in relation to histological variants, and the outcome of PTC in a cohort of patients with GD submitted for thyroidectomy during the period 2002–2010 in a Greek population.
Methods
Subjects
This is a retrospective, nonrandomized, population-based study. A total of 2188 patients who underwent total thyroidectomy in the Department of Otolaryngology at Venizelio General Hospital of Heraklion, Crete, between January 2002 and December 2010 were evaluated retrospectively. The surgical management of the patients was recommended upon referral to our hospital for several reasons, such as the presence of malignant or suspicious thyroid nodules identified by fine-needle aspiration biopsy (FNAB), multinodular goiter, the recurrence of hyperthyroidism in GD, or retrosternal goiter with compression of neighboring structures. The diagnosis of GD was based on the presence of typical symptoms, such as heat intolerance, fatigue, weight loss, increased sweating, increased appetite, muscle weakness, and tremor; laboratory findings included a suppressed TSH, elevated free triiodothyronine or free thyroxine, and positive TRAb. Ultrasonography revealed diffusely enlarged thyroid glands.
All of the patients were operated on by the same surgeons, and the thyroid specimens were examined by three pathologists at our institution. Anatomical sections of the entire gland and additional lymph node tissue that were 1 mm thick were evaluated. The patients who had metastases that were detected preoperatively by FNAB, or intraoperatively by palpation of the central neck compartment, underwent a level VI dissection as recommended in the American Thyroid Association 2009 guidelines.
In the present study, the inclusion criteria were adult age, standard total thyroidectomy, and histopathological diagnosis of PTC. All of the patients with GD who were included in the study had positive TRAb. Patients with GD were treated with antithyroid drugs, which were administered either during 18 or 24 months. The patients who relapsed after two courses of treatment with antithyroid drugs underwent total thyroidectomy. Additionally, patients with GD with a positive FNAB for malignancy were operated on at diagnosis. The exclusion criteria included previous neck surgery, family history of thyroid cancer, and history of neck radiation. The patients were divided into two groups: group 1 comprised patients with PTC and GD, whereas group 2 comprised patients with PTC without GD.
Of the 2188 patients treated with total thyroidectomy, 687 (31.4%) were found to have malignant neoplasms. By histological examination, PTC was diagnosed in 570 (26.1%) patients, while follicular, medullary, and anaplastic thyroid carcinomas were diagnosed in 85, 28, and 4 patients, respectively. Concomitant central neck compartment lymph node dissection was performed in 148 (26.0%) patients with PTC. Of the 570 patients with PTC, 339 (59.5%) had papillary thyroid microcarcinomas (PTMC; tumor size ≤10 mm) and 231 (40.5%) had PTC (tumor size >10 mm).
The examined parameters included age at the time of surgery, sex, the clinical characteristics of the tumor and the final pathological examination of the thyroid carcinoma, including multifocality, bilaterality, cervical lymph node involvement, thyroid capsular invasion, and histological variants. The clinical characteristics considered for statistical analysis were age (<45 years vs. ≥45 years), sex, weight of the gland (≤30 g vs. >30 g), and cervical lymph node metastasis at the time of diagnosis as determined by preoperative FNAB. Where available, the preoperative diagnosis of PTC was made by FNAB. All nodules with suspicious ultrasonographic features such as microcalcifications, marked hypoechogenicity, irregular margins, and the absence of a hypoechoic halo around the nodule were biopsied, regardless of their size.
The histopathological features considered for statistical analysis were the size of the tumor at its greatest diameter (tumor ≤5 mm, tumor >5 to ≤10 mm, and tumor >10 mm), histopathological evidence of GD, thyroid capsular invasion, tumor focality (right lobe vs. left lobe; bilateral and unifocal vs. multifocal), and histological variants of PTC (papillary, follicular, sclerosing, TCV). The tumors were considered as multifocal if two or more foci were found in one or both lobes. In the case of multiple tumor foci, the dimension of the largest one was used for the statistical analysis. PTC was diagnosed as TCV if it was composed of ≥50% tall cells. The tall cells were defined as having a height that was at least twice their width, an eosinophilic cytoplasm, and with the nuclear features of PTC (18) (Fig. 1). The follicular variant of PTC was defined as being composed entirely or nearly completely of follicles, lined by cells with nuclear features of PTC (19).
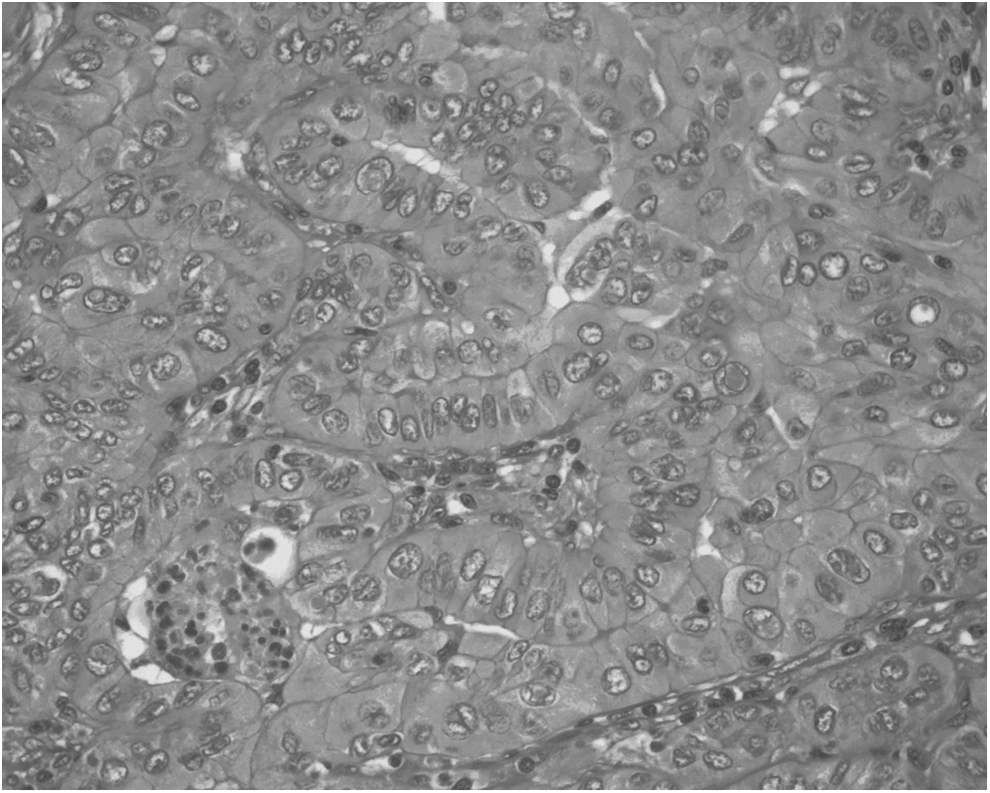
Typical features of tall cell variant (TCV) papillary thyroid carcinoma at high-power magnification (hematoxylin and eosin, ×400). The cells of the TCV are two or more times as high as they are wide and they have abundant eosinophilic cytoplasm. The nuclei of TCV cells have abundant intranuclear pseudoinclusions.
The 7th edition of the International Union Against Cancer TNM Classification for Malignant Tumors (20) was used to describe and categorize cancer stages and progression. PTC was defined as incidental or clinically unsuspected in patients who underwent surgery for diseases unrelated to thyroid malignancy and in whom the diagnosis of PTC was made at final histology. PTC was considered to be nonincidental or clinically suspected when at least one of the following occurred: (i) preoperative diagnosis or suspicion based on FNAB of the malignant thyroid nodules; (ii) preoperatively proven or suspected neck node metastasis; and (iii) preoperatively proven or suspected distant metastasis.
The follow-up period ranged from 12 to 86 months (mean 31.90±17.10 months). All of the patients were examined at 3, 6, and 12 months after the initial treatment. Thereafter, they were examined yearly or more frequently, in a follow-up period of 12–86 months, depending on their clinical course. During the follow-up period, the patients were subjected to clinical examination, neck ultrasonography, and measurement of serum TSH, thyroglobulin, and free thyroxine. One year after initial therapy, a whole-body scan was performed to detect local thyroid remnants and lymph node and/or distal metastases, according to the guidelines of American Thyroid Association (21). Patients with TSH-stimulated serum thyroglobulin levels <1 ng/mL, negative whole-body scan, and with no evidence of neck lymph node metastases at ultrasonography were defined as being free of disease. Distant metastases were found at the time of diagnosis in 28 (4.9%) of patients with PTC.
Statistical analysis
Univariate analysis was performed with the Pearson chi-squared test and the Fisher exact test as appropriate. Statistically significant results obtained from univariate analysis were submitted to multivariate logistic regression. A p-value <0.05 was considered to be statistically significant. SPSS software version 17 (SPSS, Inc., Chicago, IL) was used for statistical analysis.
Results
Tumor characteristics
In total, 2188 patients were subjected to total thyroidectomy from January 2002 through December 2010. Of them, 181 patients underwent total thyroidectomy for GD, and PTC was detected in 33.7% of these patients. PTC was diagnosed in 570 patients who were divided into two main groups as follows: group 1 comprised 61 (10.7%) patients with GD and group 2 comprised 509 (89.3%) patients without GD. The patients with PTC were further classified into the three following subgroups based on the size of their tumors: subgroup A with microcarcinomas sized ≤5 mm comprised 250 (43.9%) patients; subgroup B with tumor size >5 mm and ≤10 mm comprised 89 (15.6%) patients; subgroup C with tumor size >10 mm (conventional PTC) comprised 231 (40.5%) patients (Fig. 2).
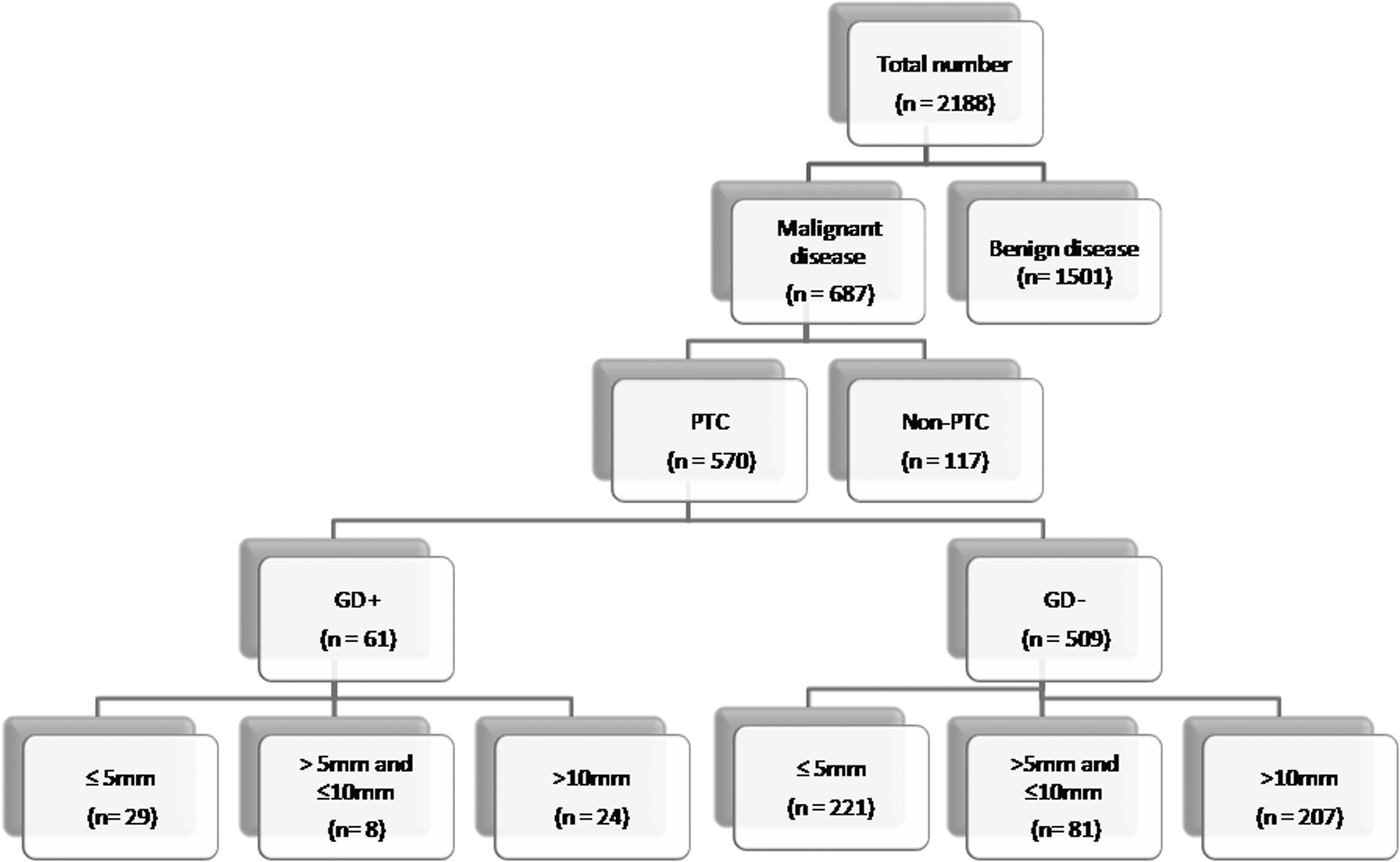
Groups of patients included in the study.
As Table 1 illustrates, 452 (79.3%) of the 570 patients were female and 118 (20.7%) were male. The male/female ratio was 1/4. The mean patient age at diagnosis was 49.64±14.03 years (range 18–88 years). There were 341 (59.8%) patients over 45 years of age and 229 (40.2%) patients under 45 years of age. Differences in clinicopathological features were observed between the two main groups. The mean tumor diameter was 9.77±8.70 mm (range 1–52 mm), and the mean weight of thyroid glands was 33.09±24.73 g, with a range of 6–350 g. Among all of the patients with PTC, bilaterality was found in 140 (24.6%) patients, multifocality in 199 (34.9%), lymph node metastasis in 113 (19.8%), and thyroid capsular invasion in 127 (22.3%) patients. The most common histological variant was the pure papillary variant (n=447, 78.4%). Other variants found in the histopathological examinations included the follicular variant (n=58, 10.2%), sclerosing variant (n=23, 4.0%), and TCV (n=42, 7.4%) of PTC.
GD, Graves' disease; PTC, papillary thyroid carcinoma.
In 193 (33.7%) PTC patients, the malignancy was detected preoperatively by a positive FNAB and/or cervical lymph node metastasis. These patients represented the nonincidental group. The remaining 377 (66.3%) patients represented the incidental group, in which the thyroid nodule or nodules were not palpable and were detected either incidentally during diagnostic procedures for thyroid disease or by postoperative pathological examination of the specimens after thyroid resection for benign diseases.
PTC subgroups in relation to GD
In group 1 of GD+ PTC patients, 47 (79.3%) were female and 14 (20.7%) were male. The mean age at diagnosis was 52.57±13.87 years, and the mean size of the tumor was 9.16±8.52 mm. The mean weight of the thyroid gland was 39.95±24.18 g. Bilaterality was found in 16 patients (26.2%), multifocality in 24 (39.4%), lymph node metastasis in 18 (29.5%) and thyroid capsular invasion in 15 (24.6%; Table 1). Among the GD+ PTC patients, 36 (59.0%) had pure papillary variant, 12 (19.7%) follicular variant, 4 (6.6%) sclerosing variant, and 11 (18.0%) TCV of PTC.
In group 2 of GD− PTC patients, 405 (79.6%) were female and 104 (20.4%) were male. The mean age at diagnosis was 49.29±14.02 years, and the mean size of the tumor was 9.84±8.73 mm. The mean weight of the thyroid gland was 32.27±24.74 g. Bilaterality was found in 124 patients (24.4%), multifocality in 175 (34.4%), lymph node metastasis in 95 (18.7%), and thyroid capsular invasion in 112 (22.0%; Table 1). Among the GD− PTC patients, 411 (80.6%) presented with the pure papillary variant, 46 (9.0%) with the follicular variant, 19 (3.7%) with the sclerosing variant, and 31 with the (6.1%) TCV.
Univariate analysis of the groups
Univariate analysis showed that age at diagnosis ≥45 years (p=0.038), weight of the thyroid gland >30 g (p<0.001), lymph node metastasis (p=0.045), and TCV type (p=0.009) were features that were significantly more common in patients with GD. No differences were observed between GD+ PTC and GD− PTC patients in terms of sex, bilaterality, multifocality, size of tumor, and thyroid capsular invasion (Table 2).
A further analysis demonstrated differences between GD+ and GD− PTC patients with respect to the size of tumors. Univariate analysis in patients of subgroup A (tumor size ≤5 mm) showed that there was no difference between GD+ PTC and GD− PTC patients with relation to sex, age, bilaterality, multifocality, lymph node metastasis, thyroid capsular invasion, and histological variant (Table 3). The weight of the thyroid gland of GD+ PTC patients within subgroup A was significantly higher than that in GD− PTC patients (p=0.001; Table 3). In subgroup B, the tumors from patients with GD demonstrated a higher frequency of lymph node metastases (p=0.001) and TCV histology (p=0.003) than the GD− tumors.
PTMC, papillary thyroid microcarcinomas.
Additionally, multifocality was observed much more frequently in GD+ PTC, although this finding was not statistically significant (p=0.07). No differences were observed between GD+ and GD− patients of subgroup B in terms of sex, age, bilaterality, thyroid capsular invasion, and weight of the thyroid gland (Table 4). In subgroup C, the analysis showed that age at diagnosis≥45 years (p=0.041), the weight of thyroid gland >30 g (p=0.011), and the follicular variant of PTC (p=0.018) were significantly more frequent in GD+ patients than in GD− patients. There was no significant difference between GD+ and GD− patients of subgroup C in terms of sex, bilaterality, multifocality, lymph node metastasis, thyroid capsular invasion, and TCV (Table 5).
Multivariate analysis
Multivariate analysis showed that only in subgroup B, male sex (p=0.05), lymph node metastasis (0.012), and TCV (0.002) were independent risk factors associated with GD.
Recurrence of disease
Disease recurrence was observed in 41 patients (7.2%). Of these, 5 (8.2%) patients were from group 1, and 36 (7.1%) patients were from group 2. No significant difference between the two groups was observed. Recurrence was found in 5 (2%) patients from subgroup A, in 4 (4.5%) patients from subgroup B, and in 31 (13.4%) patients from subgroup C. Univariate analysis showed that the risk factors for recurrence were tumor size (p<0.001), multifocality (p=0.014), thyroid capsule invasion (p=0.023), lymph node metastasis (p<0.001), and TCV (p=0.003; Table 6).
Discussion
In the last decade, the rising incidence of thyroid carcinoma can be accounted for by a marked increase in the incidence of well-differentiated tumors. The rate of incidentally discovered papillary microcarcinomas is high because of the advances in ultrasonographic screening and ultrasonography-guided FNAB. These have facilitated the detection and the diagnosis of PTC, resulting in a marked increase in the number of patients diagnosed with PTMC. The most significant increase has been observed in the uncommon histological variants of PTC, such as the TCV, which can be associated with a more aggressive behavior (15,21 –24). Our study investigated the incidence of PTC in patients with GD and the relation of GD with aggressive histological variants. On the basis of this, our working hypothesis was to reevaluate the need for earlier surgical treatment in cases of suspicious nodular GD.
More than 99% of patients with papillary thyroid microcarcinoma are not at risk of distant spread or carcinoma mortality (25). However, in a previous study, we showed that patients presenting multifocal, bilateral PTMC >5 mm, and thyroid capsule invasion may have an increased risk of lymph node metastasis (26).
The decision for surgery in patients with GD was determined by various factors based on clinical indications such as medical comorbidities and patient's preference, relapsing thyrotoxicosis, an inability to take antithyroid medications, side effects from medications, large retrosternal goiters, and suspicious cytological findings after FNAB.
Our data clearly show an increased incidence (33.7%) of PTC in GD in the Greek population compared with other studies that reported an incidence from 3.6% to 17% (6,7). Tamatea et al. (6) demonstrated the predominance of micro-PTC compared with macro-PTC (4.2% vs. 1.8%). Accordingly, in the present study, we found that papillary carcinoma was diagnosed in 26.1% of patients, of whom 15.5% had microcarcinoma (≤10 mm) and 10.56% had a carcinoma greater than 10 mm (6). The higher incidence of PTC in patients with GD in our population could be explained by the fact that surgery was more frequently a treatment option for patients with GD with nodules, compared with patients with nodular thyroid disease without GD. Furthermore, it has been shown that nodular GD harbors a 42% risk for PTC (7).
In comparison to PTC patients without GD, those with GD were significantly older, had heavier thyroid glands, and presented with lymph node metastases at diagnosis. The incidence of the diffuse sclerosing variant was not significantly different between GD+ and GD− PTC patients (Table 5). Furthermore, our analysis showed that the diffuse sclerosing variant was not an independent risk factor for recurrence in PTC patients. This result is in accordance with other studies (27).
TCV is estimated to account for 3.2–19% of all PTC, a rate that is comparable to our data (28,29). The prevalence of TCV in patients with PTC in GD has not been clearly documented. In the present study, the prevalence of TCV PTC was 18% in GD+ and 6.1% in GD− patients. Our data show that in patients with GD, TCV and lymph node metastases were significantly associated with tumor size. In addition, the TCV was more frequent in patients with nodular GD, specifically in those with microcarcinomas in the nodules (subgroup B). Although TCV was more frequent in all three subgroups of GD patients, the increased frequency achieved statistical significance only in the >5 mm to ≤10 mm group, which comprised only 8 cases of PTC. Further investigations are required to confirm this finding and to determine if increased TCV is also found in GD patients with larger PTC, and whether these GD-associated micro-TCVs actually have a worse prognosis.
Statistically, TCV in GD+ patients was also significantly associated with the occurrence of lymph node metastases compared with GD− PTC. Recent studies suggest that patients with TCV exhibit poorer survival than patients with classical PTC (30). Another study showed that TCV presents at a higher stage and with more advanced local disease in GD patients. TCV has been associated with a higher risk of locoregional and distant relapse and a worse overall survival (31). TCV alone remains a significant prognostic factor for disease-specific mortality (30).
Several authors have reported that lobectomy with or without isthmusectomy is an adequate conservative approach for patients with low-risk PTC (25,32,33). The current American Thyroid Association guidelines do not specifically address the extent of thyroidectomy for patients with aggressive variants of PTC (21). Recent studies have suggested that the TCV should be treated with more aggressive approach. This includes total thyroidectomy followed by central compartment neck dissection and radioactive iodine ablation, regardless of tumor size (27,34). The unfavorable effect of TCV PTC on prognosis may necessitate a cautious and more aggressive approach than the one that is followed in the majority of patients with pure PTC. Several studies have reported that PTC is more aggressive in GD patients than in euthyroid patients. The results of our study show that TCV was significantly more frequent in Graves' patients with PTC. TCV was also an independent risk factor for GD and recurrence.
The results of our analysis show that PTC GD+ patients had a significant increase in lymph node invasion as compared with PTC GD− patients. This could be explained by the incidence of the aggressive variants. It is likely that the autoimmune process of GD, in addition to the aggressive variant, may affect the clinical evolution of the thyroid carcinoma. Lymph node metastases were detected in 6/11 (54.5%) of TCV GD+ patients and in 9/31 (29.0%) of TCV GD− patients (p≤0.001).
The follicular variant of PTC was found to be more frequent in patients with macropapillary carcinoma (subgroup C) and GD than in patients in other subgroups. In this subgroup, the follicular variant of PTC was significantly more frequent in GD+ patients than in GD− patients. The follicular variant of PTC is classified into two distinct types: an infiltrative/diffuse (nonencapsulated) subvariant, which resembles pure papillary carcinoma in its metastatic lymph node pattern and invasive growth, and an encapsulated form, which typically has a more indolent course (35). Liu et al. showed that patients who have the noninvasive, encapsulated follicular variant PTC did not develop lymph node metastases or recurrences and could be treated by lobectomy alone (35). In our study, in subgroup C, the follicular variant in GD+ PTC was not associated with an increase in the presence of lymph node metastasis compared with GD− PTC.
Conclusions
Our study clearly shows that the incidence of PTC in GD+ patients is higher than that in patients without GD. Aggressive variants of PTC, like the TCV, were more frequent in nodular micro-PTC, especially in patients with nodules >5 and ≤10 mm.
An early evaluation of nodular GD with FNAB should be considered, regardless of tumor size because of the predominance of the TCV in micro-PTC. In patients with GD, it is more likely that the higher incidence of TCV carcinomas contributes to the aggressiveness of PTC tumors. These findings suggest that prompt and meticulous evaluation of nodules in any patient with GD associated with nodular alterations must be considered. Further studies with larger numbers of patients and long-term follow-up are needed to draw definitive conclusions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.