
Abstract
Background:
Non–islet cell tumor-induced hypoglycemia (NICTH), a major cause of fasting hypoglycemia, is caused by the overproduction of incompletely processed, high molecular-weight insulin-like growth factor-II (IGF-II), termed “big” IGF-II. To the best of our knowledge, only two cases of thyroid carcinoma associated with NICTH have been documented.
Patient Findings:
We report the case of a 72-year-old woman who was brought to the emergency department with impaired consciousness. The patient had a history of pulmonary metastases from poorly differentiated thyroid carcinoma (PDTC), spanning 12 years since initial treatment. Laboratory tests showed decreased plasma glucose levels even though immunoreactive insulin, IGF-I, and growth hormone (GH) were undetectable. Computed tomography (CT) scan revealed macronodular pulmonary metastases the estimated volume of which was 456 mL. Both the biochemical data and imaging results suggested NICTH. The results of Western blot analysis performed on a fractionated serum sample showed an increased expression of big IGF-II, an important indicator in the diagnosis of NICTH. Because the massive pulmonary metastases were considered inoperable, immunohistochemical analysis of stored formalin-fixed, paraffin-embedded tissues was performed. The analysis revealed that the tumor cells were positive for both IGF-II and thyroglobulin. A whole-body CT excluded extrapulmonary metastatic lesions. A retrospective review revealed a gradual decrease in glycohemoglobin levels accompanied by an increase in the estimated volume of pulmonary metastases. These findings suggested that NICTH had been caused by pulmonary metastases from PDTC.
Conclusions:
We describe here the third reported case of NICTH associated with thyroid carcinoma. This is also the first case reporting big IGF-II in the serum of a patient with thyroid carcinoma.
Introduction
N
Poorly differentiated thyroid carcinoma (PDTC) is rare, comprising less than 1% of all thyroid malignancies in Japan (6). These tumors follow an aggressive course and tend to present with higher rates of gross extrathyroidal extension than differentiated thyroid carcinomas such as papillary thyroid carcinoma (PTC) and follicular thyroid carcinoma (FTC) (7). We report here an unusual case of a patient with IGF-II–producing NICTH associated with macronodular pulmonary metastases from PDTC.
Patient
In March 2000, a 60-year-old woman with respiratory distress caused by a rapid enlargement of goiter was admitted to our hospital. A total thyroidectomy had been performed at another hospital, and the histological examination revealed FTC. Because the serum thyroglobulin (Tg) levels remained elevated, radioactive iodine ablation (100 mCi) was administered twice. However, pulmonary metastases developed later, and surgical resections were performed three times between 2004 and 2006. The histological sections demonstrated a solid trabecular growth with scanty formation of colloid-containing follicles (Fig. 1A, D), tumor necrosis, and increased mitoses. These findings confirmed the diagnosis of PDTC according to the World Health Organization definition. In spite of repeated treatment, the pulmonary metastases recurred for the fourth time and gradually grew larger (Fig. 2A). The patient refused surgery and lived for 12 years after initial treatment without any symptoms of pulmonary involvement.
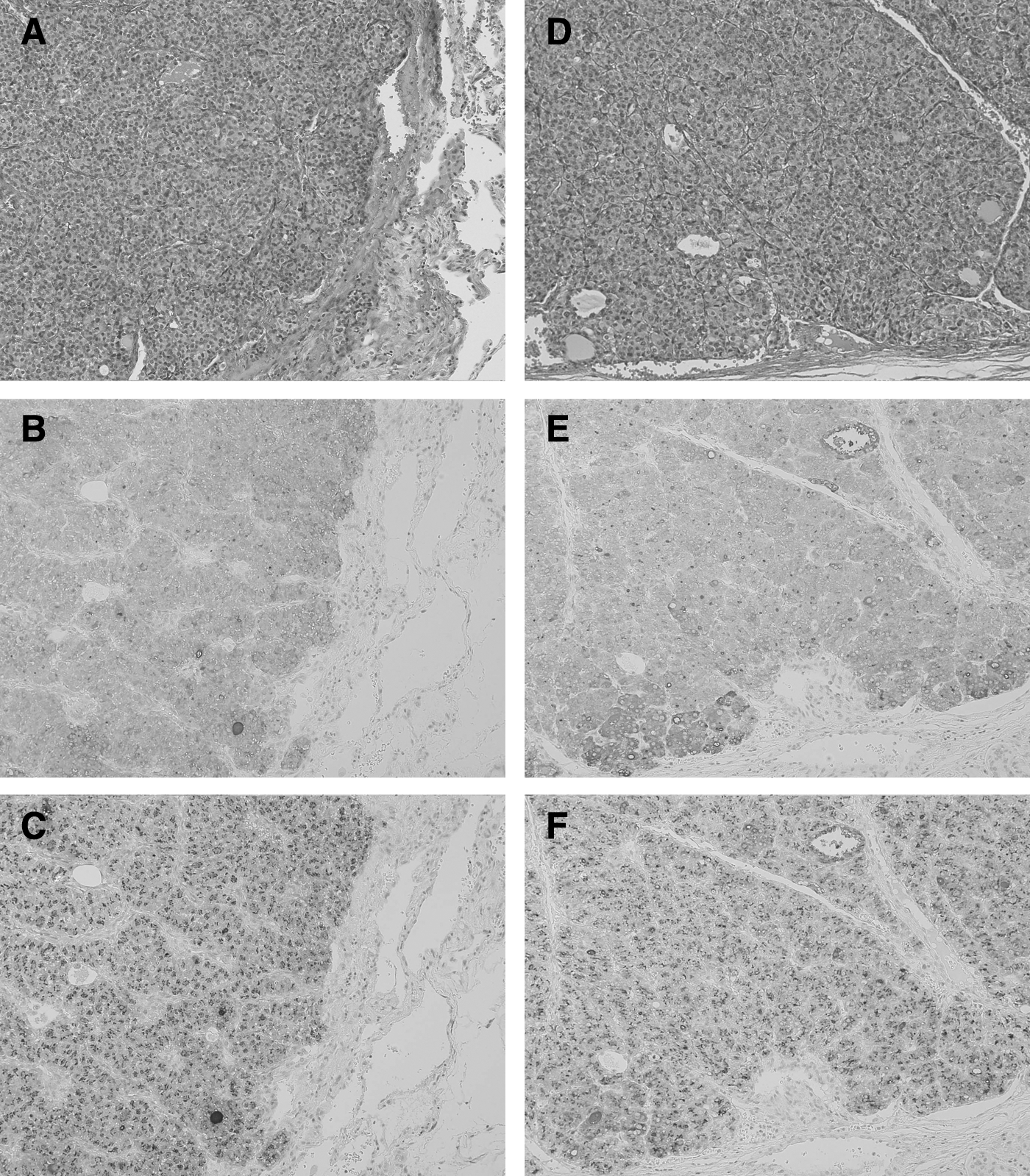
Histological analysis of the metastatic, poorly differentiated thyroid carcinoma in the lungs resected in 2004

Clinical course of the estimated tumor volume and glycohemoglobin (HbA1c) levels after the last surgical treatment performed in 2006
In April 2012, the patient was brought to the emergency department of our hospital because of impaired consciousness (Glasgow Coma Scale 11). Hypoglycemia was diagnosed and corrected by intravenous glucose administration. The patient had a history of diabetes mellitus diagnosed at the age of 56 years but had never been treated with antidiabetic medications. She was 154 cm tall and weighed 44.5 kg (body mass index, 18.7 kg/m2). Chest X-ray and computed tomography (CT) scan revealed multiple large tumors in the pulmonary fields (Fig. 2B, C). The patient was admitted for further evaluation.
Methods
Written informed consent was obtained from the patient for the publication of this case report. On the basis of the CT scan data, the estimated tumor volume was calculated as the sum of the lesion area in all sections multiplied by the section thickness of 5 mm. Glucose level was measured using the glucose oxidase method and glycohemoglobin (HbA1c) was measured by high-performance liquid chromatography (Tosoh Corporation, Tokyo, Japan). The levels of serum insulin, immunoreactive insulin (IRI), growth hormone (GH), Tg, and anti-Tg antibodies were determined by electrochemiluminescent immunoassay (Roche Diagnostics K.K., Tokyo, Japan). Total IGF-I was measured using an immunoradiometric assay (TFB Inc., Tokyo, Japan).
Western blot analysis
Recombinant human IGF-II (750 pg) and 15 μL of diluted serum (1:10, in the sample diluent buffer) were fractionated on a 15% sodium dodecyl sulfate polyacrylamide gel and electrophoretically transferred to a nitrocellulose membrane. The membrane was incubated with biotinylated antihuman IGF-II antibody and probed with avidin–biotin-peroxidase complex (Boster Biological Technology, Ltd., CA). Peroxidase enzymatic reaction was visualized using a chemiluminescence detection system (GE Healthcare, Buckinghamshire, United Kingdom).
Immunohistochemistry
Immunohistochemistry was performed using antibodies against IGF-II (anti–IGF-II clone S1F2, Upstate Biotechnology, Inc., Lake Placid, NY) and Tg (rabbit antihuman thyroglobulin, Dako, Glostrup, Denmark). All immunohistochemical analyses were performed by technical specialists at Kyodo Byori, Kobe, Japan.
Results
Laboratory tests showed a low plasma glucose level (24 mg/dL) even though IRI, GH, and IGF-I were undetectable. The serum Tg on levothyroxine was 721 ng/mL, and anti-Tg antibodies were undetectable. Liver, kidney, and adrenal function were unimpaired. Because IGF-II–producing NICTH was suggested by the results of the biochemical tests and imaging data, a serum sample was fractionated and subjected to Western blot analysis with an anti-IGF-II antibody. The results demonstrated that most of the IGF-II was detectable as high-molecular-weight bands (Fig. 3, lane 2). The increased levels of big IGF-II in the serum, accompanied by the decreased plasma IRI, GH, and IGF-I levels led to the diagnosis of NICTH. The serum concentration of IGF-II was not determined but the expression level of total serum (i.e., mature and big) IGF-II in the patient was higher than in the control subject (Fig. 3, lanes 2 and 3). The measurement of IGF-BP2, IGF-BP3, of the acid labile subunit (ALS) as well as IGF-II might be valuable in the diagnosis of NICTH. However, this was not performed due to technical problems (unavailability of the commercial kits in Japan).
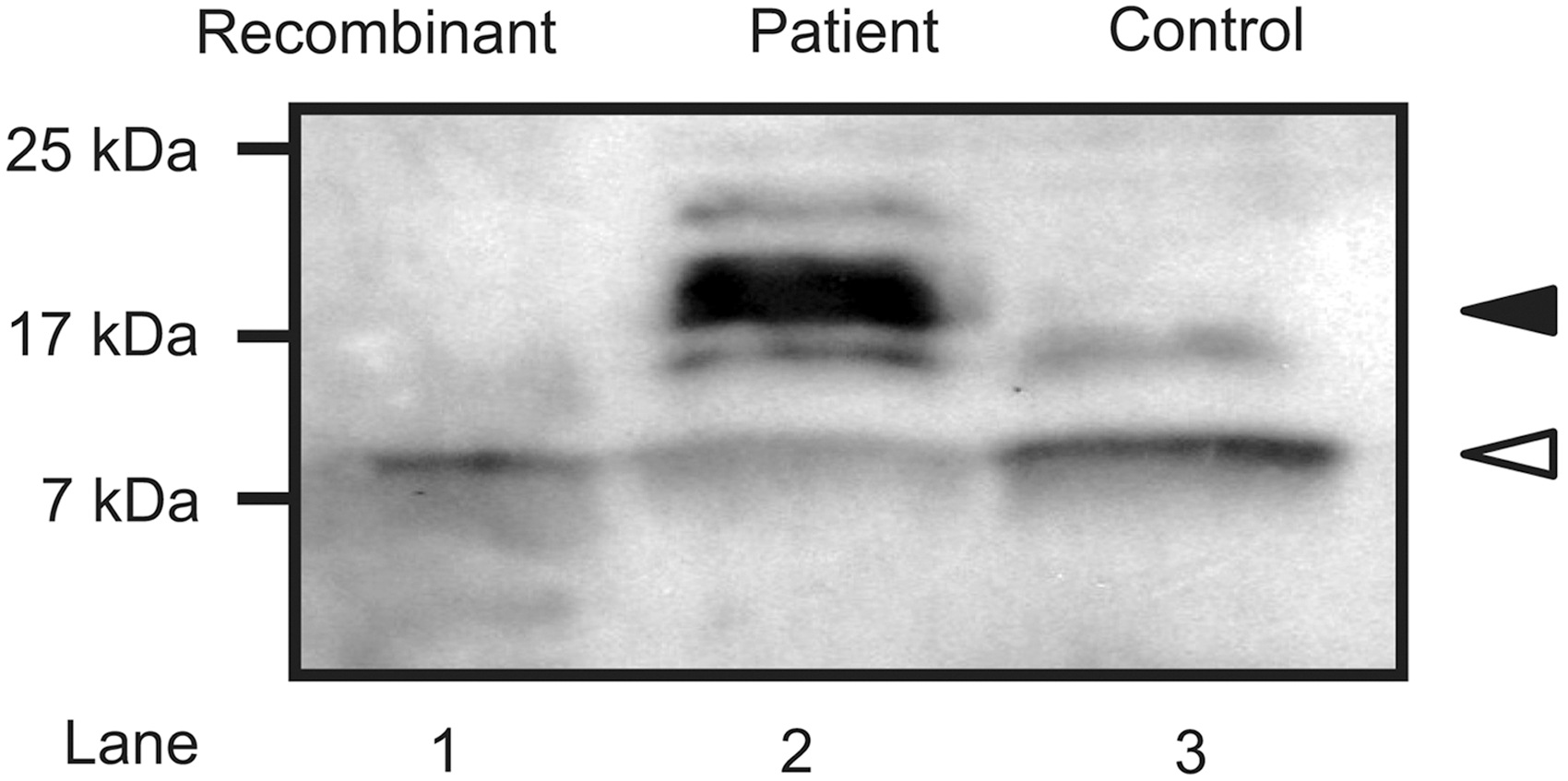
Western blot analysis of recombinant human insulin-like growth factor (IGF)-II (lane 1) and serum IGF-II in the patient (lane 2), compared with that of a sample obtained from a control subject (lane 3). Black arrowhead, “big” IGF-II; white arrowhead; mature IGF-II.
Because the massive pulmonary metastases were unresectable, treatment with oral dexamethasone (0.5 mg/day) and continuous intravenous infusion of glucose (75 g/day) was started. The administration of somatostatin analogues was not attempted because the octreotide suppression test did not increase the serum glucose. Dexamethasone and glucose doses were gradually increased to 4 mg/day and 175 g/day, respectively, to prevent recurrent hypoglycemic episodes, and the patient was discharged from the hospital.
Immunohistochemical analysis of stored formalin-fixed, paraffin-embedded tissues obtained in 2004 and 2006 revealed that the tumor cells were positive for both IGF-II and thyroglobulin (Fig. 1D, E); no analysis of the unresectable metastatic tissue was performed. A gradual decrease in HbA1c accompanied by an elevation in the estimated tumor volume (Fig. 2A), in the absence of any other suspicious tumors on the whole-body CT, supported the conclusion that NICTH had been caused by pulmonary metastases from PDTC.
Discussion
IGF-II–producing NICTH is now regarded as a major cause of fasting hypoglycemia (8). To the best of our knowledge, only two reports of thyroid carcinoma associated with IGF-II expression have been published to date (Table 1). The first patient, described by Rosario et al., was a 57-year-old man with massive pulmonary metastases from PDTC (9). The diagnosis of NICTH has been made on the basis of unusually high total IGF-II level accompanied by a low serum IGF-I level and suppressed GH, IRI, and C-peptide levels. Interestingly, a significant decrease in the total serum IGF-II and the resolution of hypoglycemic episodes have been observed after chemotherapy, making the association between thyroid carcinoma and NICTH more convincing. The second patient, reported by Himeno et al., was a 66-year-old man with massive metastases from PTC in the pelvis, inferior vena cava, and both kidneys. The results of laboratory tests for this patient revealed a high IGF-II:IGF-I ratio leading to the diagnosis of NICTH (10). Because metastatic lesions were inoperable, the primary thyroid lesion resected 6 years earlier was examined. In this case of NICTH associated with thyroid carcinoma, the immunohistochemical staining showed for the first time, an increased expression of IGF-II in tumor cells in comparison with the surrounding normal tissue.
Pelvis represents pelvis, inferior vena cava and kidneys.
M, male; F, female; BMI, body mass index; N/A, not available; PDTC, poorly differentiated thyroid carcinoma; PTC, papillary thyroid carcinoma; IGF, insulin-like growth factor; IHC, immunohistochemistry; Pos., positive.
The crucial event in the development of NICTH is an aberrant secretion of big IGF-II by the tumor, resulting in a persistent, insulin-like activity (1,2). Mature IGF-II, comprising 80% to 90% of the total IGF-II in normal serum, is bound to a heterotrimetric 150 kDa complex consisting of IGF-II, IGF-binding protein (IGFBP), and an ALS. In contrast, big IGF-II forms a smaller 50 kDa complex with IGFBP; this smaller size makes it easier to reach insulin target organs through the capillaries (11). The examination of serum levels of big IGF-II is very useful in the diagnosis of NICTH (1,12); however, the methods for determining the big IGF-II levels are not routinely available in most Japanese clinical laboratories. To the best of our knowledge, ours is the first reported case showing increased serum levels of big IGF-II in a patient with NICTH and thyroid carcinoma. The findings reported here support the proposed association between NICTH and thyroid carcinoma. In the clinical setting, the diagnosis of NICTH must be considered when an elevated serum IGF-II/IGF-I ratio and decreased IGF-I levels are observed in patients with large tumors associated with hypoinsulinemic hypoglycemia. The measurement of the total IGF-II concentration is not sufficient for an accurate diagnosis because approximately half of the patients with NICTH show normal IGF-II levels (12).
To the best of our knowledge, this is the third documented case of NICTH associated with thyroid carcinoma. Taking into account the reported frequency of thyroid carcinoma (age-standardized incidence rate of 2.0–3.0 per 100,000 in the general population) (13), the number of cases with associated NICTH seems to be small. This discrepancy might have several explanations. First, NICTH could be occasionally caused by differentiated thyroid carcinomas, which is the common histological type of that cancer. Of the three reported cases with NICTH and thyroid carcinoma, the diagnosis of PDTC was confirmed in two cases, the case reported by Rosario et al. and the present case. In the remaining case reported by Himeno et al., the primary lesion has been diagnosed as PTC. However, a transformation of PTC to PDTC might have occurred; this possibility is suggested by an aggressive clinical behavior in that case. Second, the latest improvements in cancer treatments might prevent thyroid carcinoma from developing bulky lesions, which can produce large amounts of big IGF-II. As shown in Figure 2A, we observed a steep decrease in HbA1c levels once the estimated tumor volume exceeded 300 mL. Third, extensive metastases in the lymphatic, respiratory, and skeletal systems caused by a high-risk thyroid carcinoma initially manifest themselves with the symptoms specific to these organs rather than those specific to hypoglycemia.
Recently, several studies have reported that multiple molecular abnormalities involving the IGF system may have a role in thyroid carcinogenesis (14,15). For example, Vella et al. have found a high production of IGF-II in thyroid cancer cells, particularly in poorly dedifferentiated cells (16). A later study has demonstrated that an autocrine loop involving IGF-II and the insulin-receptor isoform-A sustains the growth and survival of cultured malignant thyrocytes (17). Unfortunately, neither the pathological characteristics nor the expression levels of IGF-II could be analyzed in the unresectable pulmonary metastases in the present case. Future studies should further elucidate the association between NICTH and tumor progression in thyroid carcinomas.
In conclusion, we describe an unusual patient with IGF-II–producing NICTH, probably caused by macronodular pulmonary metastases from PDTC. To the best of our knowledge, this is the first case demonstrating increased serum levels of big IGF-II in a patient with NICTH and thyroid carcinoma.
Footnotes
Acknowledgments
We are grateful to all the doctors who provided us with the opportunity to study the clinical course of this patient. We also thank Prof. Hirotoshi Nakamura for his valuable comments, Dr. Hiroki Mori for his advice on immunohistochemistry and Mrs. Hiroko Nakamura for examining Western blot analysis.
Author Disclosure Statement
All authors have nothing to declare.