
Abstract

In the January issue of Thyroid, Makita and Iiri (1) discussed the potential mechanisms of thyroid disorders that are associated with the treatment of tyrosine kinase inhibitors (TKIs). As an increasing number of cancer patients are treated with these agents, better understanding of the underlying mechanisms is required for optimal management of this side effect. Among the approved TKIs, the incidence of thyroid disorders appears to be highest in sunitinib-treated patients (1). Therefore, the authors focused on thyroid disorders caused by the TKI sunitinib, which targets several receptors, including vascular endothelial growth factor receptors (VEGFR)-1, VEGFR-2, and VEGFR-3, platelet-derived growth factor receptor-α and -β, c-Kit protein, and FMS-like tyrosine kinase-3 (2). Among these targets, signaling of the vascular endothelial growth factor (VEGF) is an important pathway of angiogenesis in tumors and in normal tissues (3). Apart from TKIs, the humanized monoclonal antibody bevacizumab also targets VEGF signaling. Bevacizumab targets circulating VEGF and subsequently prevents binding of VEGF to its receptors (4). In combination with cytotoxic agents, bevacizumab has been approved for the treatment of several advanced malignancies, including renal cell, colorectal, breast, and non-small cell lung cancer (NSCLC). Although bevacizumab has fewer targets than the TKIs (i.e., one target vs. multiple targets) and the incidence of bevacizumab-induced hypothyroidism appears to be relatively low as compared to that of sunitinib, the effects of bevacizumab on the thyroid gland should not be underestimated (1). The thyroid gland is a hypervascularized organ and is highly sensitive to anti-VEGF therapy. In a study in mice, Kamba et al. (5) have shown that the thyroid gland shows extensive capillary regression after anti-VEGF therapy. In humans, tissue perfusion can be assessed using dynamic positron emission tomography (PET) and radioactive water ([15O]H2O), which is a freely diffusible PET tracer (6). Using [15O]H2O PET, we have previously evaluated changes in tumor perfusion in 10 NSCLC patients at 2 hours, 5 hours, and 4 days after intravenous administration of bevacizumab (7). In four patients with a lung tumor in the upper lobes, the thyroid gland was in the field of view of the dynamic PET scan. As a result, it was also possible to evaluate the effect of bevacizumab on thyroid perfusion. For quantification of thyroid perfusion, kinetic models and parametric perfusion images were applied, as described previously (6). In these four NSCLC patients, the median perfusion in the thyroid gland decreased from 1.32mL/cm3 per minute at baseline to 0.59mL/cm3 per minute at 4 days after intravenous administration of bevacizumab. Remarkably, one of these patients showed an impressive and rapid reduction in thyroid perfusion. This female patient was known to have pre-existent hypothyroidism and was regularly treated with levothyroxine (50 μg daily). At the time of the study, the patient was euthyroid. Within a few hours after bevacizumab administration, the patient had a significant reduction in thyroid perfusion, which persisted until day 4 (Fig. 1). As it was ethically unacceptable to perform more [15O]H2O PET scans in this clinical study, no information could be obtained on thyroid perfusion at later time points. Since bevacizumab has a long terminal half-life of 17–21 days (4), a decreased thyroid perfusion could also be expected at later time points.
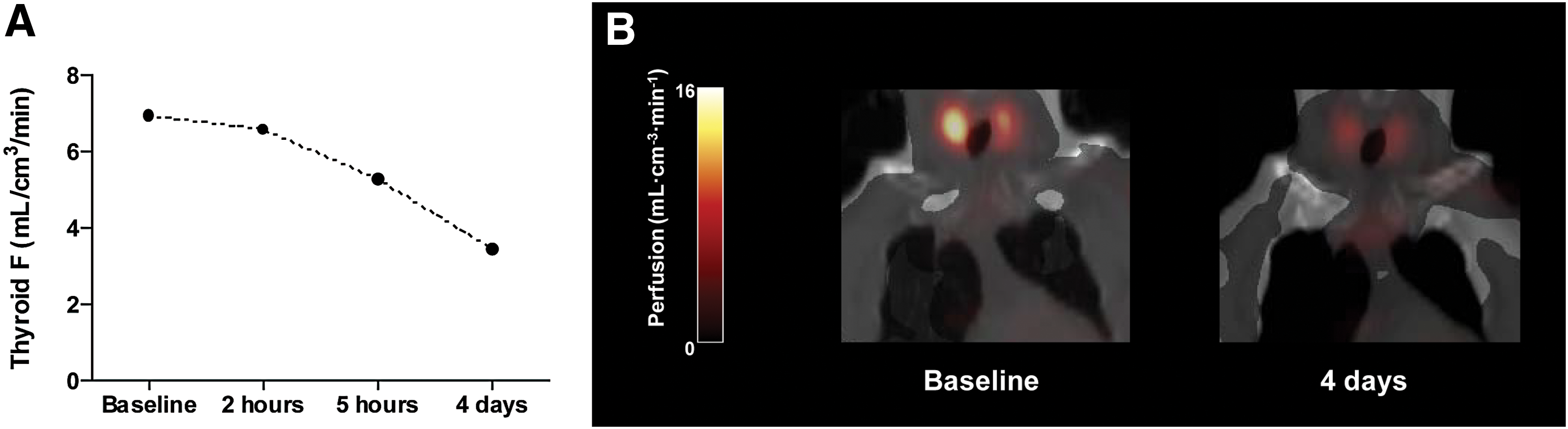
Changes in thyroid perfusion after administration of bevacizumab in a patient with pre-existent hypothyroidism.
As the bevacizumab-induced reduction in thyroid perfusion appears to be rapid, mechanisms other than inhibition of angiogenesis should be considered. Besides inhibition of angiogenesis, bevacizumab may decrease vascular permeability (8) and may induce capillary vasoconstriction in the thyroid gland (9). The lower incidence of thyroid disorders in bevacizumab-treated patients as compared to sunitinib-treated patients may be caused by a potential protective effect of placenta growth factor (PlGF) (10). Since PlGF binds to VEGFR-1, its signaling is targeted by sunitinib, but not by bevacizumab. As proposed by Makita and Iiri (1), antiangiogenic therapy may upregulate thyroidal expression of PlGF, thereby restoring the vascularity in the thyroid gland and subsequently explaining the lower incidence of thyroid disorders in bevacizumab-treated patients.
In the present case, it was not possible to evaluate whether the measured decrease in thyroid perfusion was associated with changes in thyroid function, as the patient died because of progressive disease of NSCLC. Therefore, it is not clear whether the observed decline in thyroid perfusion has clinical consequences. Nevertheless, the present example shows that bevacizumab can induce a significant decline in thyroid perfusion. It is conceivable that patients with pre-existent thyroid disorders may be more susceptible to bevacizumab treatment. The present findings suggest that monitoring thyroid function is not only required in patients who are treated with TKIs, but may also be necessary in patients who are treated with the monoclonal antibody bevacizumab.
Footnotes
Author Disclosure Statement
No conflicts of interest to disclose.