
Abstract
Background:
Ultrasonography is the most frequently used clinical tool for the identification, assessment, and follow-up of thyroid nodules. The purpose of this research was to evaluate the value of diagnostic ultrasonography indicators, to obtain rankings of the most valuable indicators in the differential diagnosis of thyroid nodules, and to analyze the optimal diagnostic points and clinical values.
Methods:
One hundred forty-four patients with 172 thyroid nodules underwent preoperative ultrasonography examinations, including gray-scale ultrasonography (GSUS), color Doppler ultrasonography (CDUS), and contrast-enhanced ultrasonography (CEUS). Fourteen indicators of thyroid nodules on GSUS, CDUS, and CEUS were selected to evaluate all thyroid nodules. The differences between the benign and malignant thyroid nodules in all indicators were analyzed by the chi-squared test; the diagnostic ultrasonography values were obtained by logistic regression; and the optimal diagnostic points were explored by receiver operating characteristic curve analysis.
Results:
Of the 172 thyroid nodules that were surgically removed, 78 were benign and 94 were malignant. Ten indicators of GSUS and CEUS showed significant differences between the benign and malignant nodules (p<0.05), whereas four CDUS indicators had no value. The rankings of the valuable indicators were obtained according to their odds ratios (ORs). The top four indicators were ring enhancement and homogeneity of enhancement on CEUS, and microcalcification and halo on GSUS. These indicators were the most valuable, with ORs of greater than 20 in the differential diagnosis of benign and malignant thyroid nodules. The other six indicators—the relative arrival time of the nodule on CEUS, interior echogenicity on GSUS, peak interior echogenicity on CEUS, shape on GSUS, peak peripheral echogenicity on CEUS, and orientation on GSUS—were also valuable, with ORs less than 20. The areas under the receiver operating characteristic curves for GSUS, CEUS, and the combination of GSUS and CEUS in the diagnosis of thyroid nodules were 0.936, 0.910, and 0.966, respectively. Five positive features of the 10 valuable indicators on GSUS and CEUS defined the cut-off for the diagnosis of malignant thyroid nodules, with a sensitivity of 89.4% (84/94), specificity of 93.6% (73/78), and accuracy of 91.3% (157/172).
Conclusions:
The ring enhancement and homogeneity of enhancement of thyroid nodules on CEUS and the microcalcification and halo on GSUS were the four most valuable indicators in the differential diagnosis of thyroid nodules. Conjoint analysis of specific features of thyroid nodules on GSUS and CEUS could enhance the diagnostic value of thyroid nodules.
Introduction
T
The gray-scale ultrasonography (GSUS) and color Doppler ultrasonography (CDUS) are the conventional imaging methods used to detect thyroid nodules and are considered valuable in the differential diagnosis of benign and malignant thyroid nodules. However, interpretative pitfalls remain. Previous studies have demonstrated that the characteristics of thyroid nodules on GSUS (i.e., microcalcifications, marked hypoechogenicity, and the absence of a hypoechoic halo around the nodule) are associated with an increased risk of malignancy (9). The sensitivity and specificity of GSUS were not high (10), demonstrating limited performance for detecting malignancies. The assessment of color flow signals on CDUS has yielded controversial results. Some results have shown that benign thyroid nodules tend to have no internal flow or minimal internal flow, with the presence or absence of a peripheral ring, and malignant nodules tend to have a peripheral ring with an extensive internal flow (11). Researchers have expressed different opinions regarding a potential correlation between color Doppler patterns and the malignancy rate of thyroid nodules (12). They have questioned whether CDUS is useful in the differential diagnosis of thyroid nodules. A relatively new technique, contrast-enhanced ultrasonography (CEUS), has been introduced to display the hemodynamics of thyroid nodules. CEUS provides a better representation of the vascular pattern than CDUS. Researchers are divided over the value of CEUS in the differential diagnosis of benign and malignant nodules. CEUS studies of thyroid nodules, conducted by analyzing the increase in the echogenicity of the nodule because of perfusion, have proven to be effective in differentiating benign from malignant nodules (13 –15). Some researchers have stated that CEUS is not clinically valuable (16). A more thorough and meticulous analysis is necessary to assess the role of ultrasonography in the differential diagnosis of thyroid nodules.
By analyzing previous studies, we found that most indicators for the use of ultrasonography for thyroid nodules were limited and incomplete, and they failed to reflect all of the characteristics associated with thyroid nodules. We analyzed all indicators that had been reported to have merit and added other indicators that might be valuable. The preliminary intention of the current study was to screen valuable indicators and to obtain rankings of the most valuable indicators by statistically analyzing complete GSUS, CDUS, and CEUS imaging information with the pathological diagnosis as the reference standard. The diagnostic value of the combination of valuable indicators was analyzed using the receiver operating characteristic (ROC) curve (17). The ultimate aim was to explore the optimal diagnostic points of the valuable indicators in the differential diagnosis of thyroid nodules.
Materials and Methods
Patients
The study was performed in accordance with the ethics guidelines of the Helsinki Declaration and approved by the ethics committee of our institute. From August 2008 to September 2012, patients who presented to our hospital for workup of thyroid nodules were evaluated for inclusion in the study. The inclusion criteria were as follows: age over 18 years, presence of solid or mainly solid thyroid nodules on GSUS and CDUS, and nodule size greater than 0.5 cm (with nodules smaller than 0.5 cm, it is difficult to maintain the same imaging sections during CEUS examination because of arterial pulsations and breathing). The exclusion criteria were as follows: dominant cystic nodules, pregnancy, grade III–IV cardiac function (New York Heart Association), severe pulmonary hypertension, and no surgical pathology of the thyroid nodule within the study period.
One hundred forty-eight patients underwent preoperative GSUS, CDUS, and CEUS examinations of the thyroid gland. One patient dropped out of the study after CEUS and did not have thyroid surgery. One case was excluded because of unsatisfactory image quality. A case with a parathyroid adenoma according to the pathology was excluded, as was one with a parathyroid cyst. A total of 172 nodules in 144 patients (105 women, age range 25–74 years, mean age 48.0±13.1 years; 39 men, age range28–73 years, mean age 50.4±10.7 years) were included in this prospective study. The patients who were found to have thyroid carcinoma underwent unilateral lobectomy or bilateral subtotal thyroidectomy according to the nodule size and enlargement of cervical lymph nodes. In the preoperative examinations, we focused on malignant and benign nodules in the same lobe of the thyroid. The surgical indications for the patients with benign thyroid nodules included (i) patients with obvious clinical symptoms, including shortness of breath, hoarseness, or pain in the neck; (ii) patients with obvious compression of and invasion into the surrounding organs, such as the trachea and carotid, and rapid growth of the nodule; and (iii) patients who were excessively worried about the nodule.
Conventional ultrasonography (GSUS and CDUS)
All ultrasonography examinations were performed with two commercially available scanners (Philips iU22 [Bothell, WA], equipped with an L12-5 transducer for conventional ultrasonography and an L9-3 for CEUS; LOGIQ E9 [GE Healthcare, Chalfont St. Giles, United Kingdom], equipped with an ML6-15 transducer for conventional ultrasonography and a 9L for CEUS). On the conventional ultrasonography, the focus zone was always placed at the same level as the thyroid nodules under examination. The GSUS parameters were modified for each nodule to obtain the optimum image quality. The sensitive pulse repetition frequency was used and remained consistent for all patients.
On GSUS, the thyroid nodules were evaluated for the following characteristics: shape (oval, round, or irregular); orientation (wider than tall, round, or taller than wide) (18); interior echogenicity (with respect to a normal thyroid parenchyma), classified as hyperechoic, isoechoic, or hypoechoic; halo (any hypoechoic rim in the periphery of a nodule) (19), classified as complete, incomplete, or none; and the presence or absence of microcalcification (hyperechoic spots less than 1 mm without acoustic shadowing in solid tissue).
CDUS was performed after GSUS. The thyroid nodules were evaluated for vascular distribution, which was classified into the following four patterns (11): none, mainly periphery, mainly interior, or both periphery and interior. Other criteria included perforating branches (presence or absence); grades of vascularization (grade I [none], grade II [less than five vessels on one scan slice], grade III [more than five vessels on one scan slice]); and the resistance index (usually, the greater value of vessels in the periphery and interior of a nodule) ≥0.75 or <0.75 (20).
Contrast-enhanced ultrasonography
After the conventional ultrasonography examination, the largest plane of the nodule was selected before the transducer was switched to the harmonic CEUS mode. The focus zone was always placed at the bottom level of the nodule being examined to adhere to the comparability principle. CEUS was performed using low intonation signal intensities (low-mechanical index imaging; low-mechanical index <0.10) to minimize microbubble destruction and artificial signal loss.
The contrast medium was SonoVue (BR1; Bracco, Milan, Italy), which is a sulfur-hexafluoride-filled microbubble contrast agent encapsulated by a flexible phospholipid shell. A white, milky suspension of sulfur hexafluoride microbubbles was obtained by adding 5 mL of physiological saline (0.9% sodium chloride) to the powder (25 mg), using standard clinical aseptic techniques, followed by hand agitation for at least 20 seconds. The contrast agent exhibits an elimination half-life of 6 hours, and more than 80% of the microbubbles can be exhaled through the lungs in 11 minutes (21). SonoVue was injected intravenously as a bolus at a 1.5 mL dose, followed by 5 mL of normal saline flush. The timer on the ultrasonography machine was started and the imaging plane was kept as stable as possible. Each contrast imaging acquisition lasted at least 2 minutes after the bolus injection and was digitally stored as raw data.
The thyroid nodules on CEUS were evaluated for the relative arrival time of the microbubbles in the nodule using the following criteria: earlier, at the same time, or later, relative to a normal thyroid parenchyma. Other evaluation criteria included peak peripheral echogenicity (with respect to thyroid parenchyma), classified as hyperechoic, isoechoic, or hypoechoic; peak interior echogenicity (with respect to normal thyroid parenchyma), classified as hyperechoic, isoechoic, or hypoechoic; peripheral ring enhancement (any hyperechoic rim in the periphery of a nodule at the peak time), classified as complete, incomplete, or none; and homogeneity of enhancement (interior solid portion of nodules), classified as homogeneous or heterogeneous.
The ultrasonography examination was performed by one of two experienced examiners. Digital video clips stored in a personal-computer-based workstation were reviewed in a random order on a screen by two radiologists blinded to the clinical and pathological patient data. Initially, each reader independently analyzed the ultrasonography images and provided a score for every nodule. The scores for GSUS, CEUS, and the combination of GSUS and CEUS were scored by giving one point for each positive indicator. Subsequently, two readers jointly reviewed and discussed the images for those nodules with scoring discrepancies to reach a consensus on their characterization.
Histological analysis
All surgical specimens were categorized according to the World Health Organization (2003) histological classification of tumors of the thyroid (22) by experienced pathologists who were blinded to the medical history and ultrasonography findings. The pathological diagnosis was used as a reference standard for the study.
Statistical analysis
The statistical analysis was performed using a statistical package (SPSS 17.0, Chicago, IL). The quantitative data were expressed as means with standard deviations, and the groups were compared using the Student's t-test. The chi-squared test and Fisher's exact test were used to compare the categorical data. The rankings of valuable indicators were assessed according to the odds ratios (ORs).
The values of the scoring method in the differential diagnosis of benign and malignant nodules were statistically analyzed using the Kruskal–Wallis test. The values of GSUS, CEUS, and the combination of GSUS and CEUS were estimated using areas under the ROC curve, which is widely accepted as the standard for describing and comparing the accuracy of diagnostic tests. The cut-off point in the ROC curve was regarded as optimally diagnostic for the differential diagnosis of benign and malignant nodules.
In all cases, p<0.05 was considered statistically significant.
Results
Histological results
Among the 172 thyroid nodules that were surgically removed, 78 were benign (48 nodular goiters, 28 follicular adenomas, and 2 granulomas) and 94 were malignant (91 papillary carcinomas, 2 medullary carcinoma, and 1 metastatic carcinoma). Some patients suffered from thyroid carcinoma and nodular goiters.
Valuable indicators of GSUS, CDUS, and CEUS
The values of five GSUS indicators in the differential diagnosis of benign and malignant thyroid nodules are shown in Table 1. The following ultrasonography features were increasingly found in the malignant nodules: roundness or irregularity in shape, round or taller-than-wide orientation, interior hypoechogenicity, absent or incomplete halo, and microcalcifications (Fig. 1). These qualities were significantly different between the benign and the malignant nodules (p<0.05).
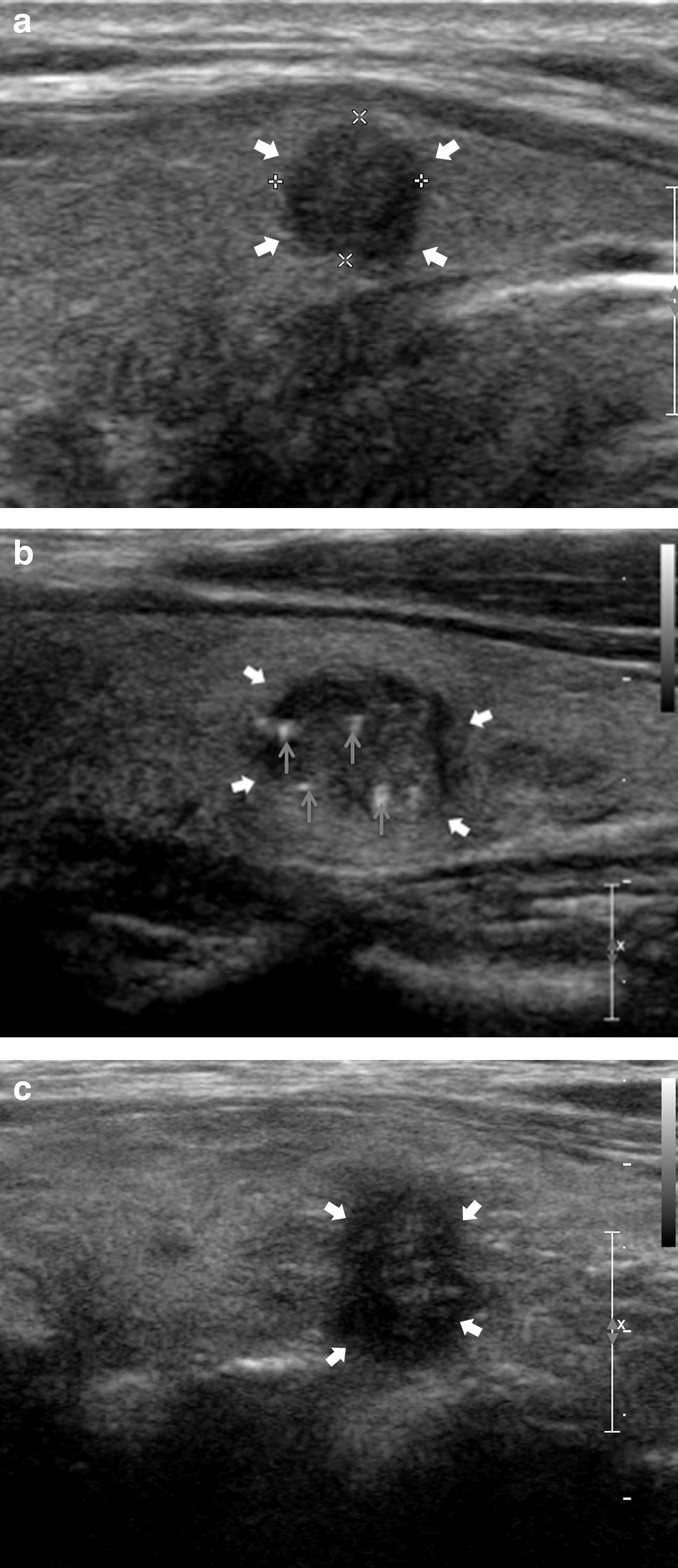
Gray-scale ultrasonography features of the malignant nodules (bold arrows): round
p<0.05 by chi-squared analysis comparing GSUS and CEUS indicators of benign nodules with malignant nodules.
CEUS, contrast-enhanced ultrasonography; GSUS, gray-scale ultrasonography.
The values of four CDUS indicators in the differential diagnosis of benign and malignant thyroid nodules are shown in Table 2. None of the CDUS indicators were significantly different between the benign and malignant nodules.
CDUS, color Doppler ultrasonography; RI, resistance index.
The values of five CEUS indicators in the differential diagnosis of benign and malignant thyroid nodules are shown in Table 1. In most malignant nodules, the relative arrival time of enhancement was delayed, and the peak peripheral and interior echogenicity were hypoechoic and exhibited absent or incomplete ring enhancement, as well as heterogeneous enhancement on CEUS (Fig. 2). The relative arrival time of the nodule, peak peripheral echogenicity, peak interior echogenicity, hypoechoic ring enhancement, and enhancement homogeneity on CEUS were significantly different between the benign and malignant nodules (p<0.05).
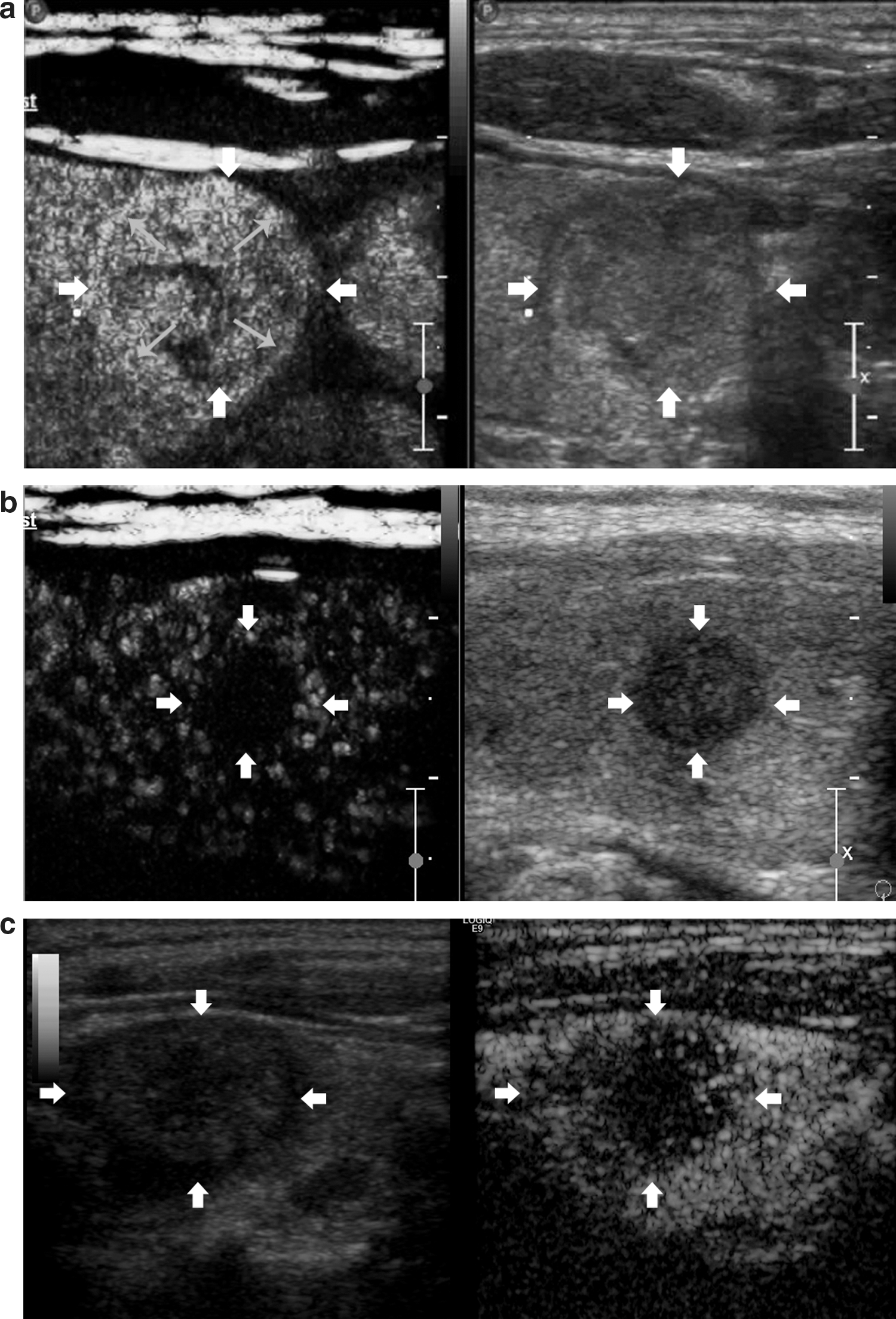
Contrast-enhanced ultrasonography features of the malignant nodules (bold arrows): the nodule
Rankings of the valuable indicators
Ten indicators of GSUS and CEUS displayed significant differences between the benign and malignant nodules. The rankings of the valuable indicators were obtained according to their ORs. The four top indicators were the ring enhancement on CEUS, the homogeneity of enhancement on CEUS, the microcalcification on GSUS, and the halo on GSUS. These indicators were the most valuable, with ORs of greater than 20 in the differential diagnosis of benign and malignant thyroid nodules. The other six indicators—the relative arrival time of the nodule on CEUS, the interior echogenicity on GSUS, the peak interior echogenicity on CEUS, the shape on GSUS, the peak peripheral echogenicity on CEUS, and the orientation on GSUS—were valuable, with ORs less than 20 (Table 3).
The optimal diagnostic point of the combination of GSUS and CEUS
The ultrasonography features that were more common in the malignant nodules, such as roundness or irregularity in shape, round or taller-than-wide orientation, interior hypoechogenicity, absent or incomplete halo, presence of microcalcification, delayed relative arrival time, peak peripheral hypoechogenicity and interior echogenicity, absent or incomplete ring enhancement, and heterogeneous enhancement, were regarded as positive features. Each positive feature was scored with one point, and the scores for GSUS, CEUS, and the combination of GSUS and CEUS were obtained as the sum of points awarded for positive features. Areas under the ROC curves for GSUS, CEUS, and the combination of GSUS and CEUS were 0.936, 0.910, and 0.966, respectively. The most valuable method in distinguishing the benign and malignant nodules was the combination of GSUS and CEUS. According to the ROC curves, the optimal number of diagnostic points for the combinations of valuable indicators in the differential diagnosis of benign and malignant nodules was five features on both GSUS and CEUS, with a sensitivity of 89.4% (84/94), specificity of 93.6% (73/78), and accuracy of 91.3% (157/172). A thyroid nodule with five positive features or more could be regarded as malignant (Fig. 3), whereas a thyroid nodule with fewer than five positive features could be regarded as benign.

A malignant nodule of a papillary thyroid carcinoma in a 32-year-old woman.
Discussion
This study analyzed 14 indicators of thyroid nodules on GSUS, CDUS, and CEUS, among which some proved to be valuable in differentiating thyroid nodules.
A total of 10 indicators (5 indicators of GSUS and 5 indicators of CEUS) were statistically valuable. Table 1 shows that some indicators had a high sensitivity and low specificity for thyroid nodules, whereas others had a low sensitivity and high specificity. It was difficult to distinguish which indicators were more valuable in the differential diagnosis of thyroid nodules. The rankings of the most valuable indicators were obtained based on the ORs.
According to Table 3, the most valuable indicator was ring enhancement. On histopathology, the benign thyroid nodules such as nodular goiters and follicular adenomas typically showed a complete capsule around the nodule, whereas the papillary carcinomas had no capsule. The infiltrative growth of malignant nodules to the surrounding tissue and peripheral compressed parenchymal vessels around the nodule might result in absent or incomplete ring enhancement on CEUS. The second indicator was homogeneity of enhancement. Benign nodules appeared homogeneous, whereas malignant nodules appeared heterogeneous. This observation may be related to the vasculature of the thyroid nodules. The blood vessels of malignant nodules are typically aberrant and tortuous, whereas the blood vessels of benign nodules are usually regular. Most malignant nodules contained areas of fibrosis, calcification, or focal necrosis, which may be too small to be distinguished by GSUS but could be detected by CEUS. The third indicator was microcalcification. A recent study showed that osteopontin, which plays an important role in the formation of microcalcification in papillary thyroid carcinoma, was significantly increased in malignant nodules compared with benign nodules (23). The fourth characteristic was halo. As the vessels were pushed to the circumference in most benign nodules, complete halos were observed with GSUS. In the malignant nodules, the vessels were not only pushed to the circumference but also infiltrated and destroyed, resulting in an incomplete or absent halo. The fifth indicator was the relative arrival time of the nodule, which was earlier in the benign nodules but delayed or concurrent in the malignant nodules. The benign nodules were hypervascular, whereas the malignant nodules were hypovascular. The sixth indicator was interior echogenicity, which was low in malignant nodules but high or moderate in benign nodules. This finding may be caused by histologic changes, such as the disappearance of the follicular epithelium, which was replaced by a rim of histiocytes and giant cells, interstitial fibrosis, infiltration of lymphocytes, and plasma cells (24). The seventh and ninth indicators were peak interior and peripheral echogenicity, respectively. Malignant nodules, especially small papillary carcinomas, were primarily hypovascular in nature. As such, the internal echogenicity of these malignant nodules always appeared to be hypoechoic relative to that of the thyroid parenchyma. In contrast, benign nodules were generally hypervascular; as such, the internal echogenicity of these nodules was typically high or moderate. In malignant nodules, the peripheral zones were mostly compressed, causing tissue ischemia; as such, the peripheral echogenicity of these nodules was usually lower than that of thyroid parenchyma. In some malignant nodules, internal echogenicity appeared to be low, whereas peripheral echogenicity appeared moderate. This observation might relate to the ill-defined margins of malignant nodules. Finally, the 8th and 10th indicators were shape and orientation, respectively. Some malignant nodules appeared to be irregular, round, or taller than wide, whereas benign nodules appeared to be oval and wider than tall. This particular aspect of tumor growth might occur because oxygen and nutrient delivery are crucial for tumor cell growth. Hypothetically, malignant tumors may configure their shape to maximize exposure and consumption of nutrients and thus optimize growth. Mathematically, surface area to volume is maximized by a spherical shape, allowing the greatest number of cells to access crucial nutritional factors in their ambient environment (25).
No single ultrasonography characteristic could conclusively distinguish benign and malignant thyroid nodules (26). From a practical standpoint, we would not make a diagnosis according to a single ultrasonography characteristic. Because GSUS was the basis for the ultrasonography, we would need to consider GSUS in any assessment. The combined value of CEUS and GSUS, but not the value of CEUS alone, was deemed necessary for the analysis. In this study, we established a scoring system of GSUS and CEUS to evaluate benign and malignant thyroid nodules with a counting score method. The use of 10 indicators to score and diagnose a thyroid nodule is impractical for clinicians, but it was difficult to choose a more statistically sound method such as multivariate logistic regression to limit the number of indicators in the small number of cases in this preliminary study. Another limitation of the scoring system is that the counting score method is too simple and less accurate than a weighting score method in the differential diagnosis of benign and malignant thyroid nodules. According to the results in this study, more than five positive indicators would indicate malignant nodules. Although an accuracy of 91.3% was achieved from this preliminary small-scale data, GSUS and CEUS cannot replace fine-needle aspiration in predicting malignancy.
In conclusion, the four most valuable ultrasonography indicators in the differential diagnosis of benign and malignant thyroid nodules were ring enhancement on CEUS, homogeneity of enhancement on CEUS, microcalcification on GSUS, and halo on GSUS. Relative arrival time of the nodule on CEUS, interior echogenicity on GSUS, peak interior echogenicity on CEUS, shape on GSUS, peak peripheral echogenicity on CEUS, and orientation on GSUS were also valuable. The CDUS indicators had no value. Analyzing the specific features of thyroid nodules on GSUS and CEUS can enhance the diagnostic accuracy. A conjoint analysis of GSUS and CEUS features was the most valuable method in distinguishing benign and malignant nodules. Five positive features represented the optimal number of diagnostic points for combined GSUS and CEUS to distinguish benign and malignant thyroid nodules, with a sensitivity of 89.4%, specificity of 93.6%, and accuracy of 91.3%.
Footnotes
Acknowledgment
This research was supported by the Shanghai Leading Academic Discipline Project, P.R. China (No: B112).
Author Disclosure Statement
No competing financial interests exist.