
Abstract
Background:
Predicting locoregional metastasis in well-differentiated thyroid carcinoma (WDTC) is a challenge for thyroid cancer surgeons. Sentinel lymph node biopsy (SLNB) has been shown to be an effective predictive tool. To our knowledge, primary tumor (T) classification has yet to be studied with regard to SLNB. We hypothesized that larger primary tumors would correlate with the rate of malignancy in SLNBs.
Methods:
A retrospective chart review was conducted on patients operated for WDTC at the McGill Thyroid Cancer Center over a 36-month period. Patients who underwent a total thyroidectomy and SLNB for WDTC were included in this study.
Results:
A total of 311 patients were included and separated into two groups (236 negative and 75 positive SLNBs). Among patients with negative SLNBs, 65% had T1 primary tumors, 17% T2, 16% T3, and 2% T4, whereas 18% of patients with positive SLNBs had T1 primary tumors, 5% T2, 45% T3, and 32% T4 (p<0.001). Patients under the age of 45 years had a higher rate of positive SLNs (36% in those <45 years vs. 17% in those ≥45 years; p<0.001).
Conclusions:
Age (<45 years) and higher T category were found to be associated with a higher rate of positive SLNBs.
Introduction
T
Well-differentiated thyroid carcinomas (WDTC) are known to predominantly spread through the lymphatics to local draining nodes, rendering the use of a sentinel lymph node biopsy (SLNB) beneficial when investigating locoregional nodal metastasis (LRNM). Since Kelemen et al. (8) first reported it for thyroid cancers in 1988, SLNB has become more and more commonly used in the management of WDTC (9 –13).
Currently, predictive factors for the presence of malignancy in thyroid nodules have been reported, ranging from clinical parameters, such as age and sex, to ultrasound findings and cytology findings (14). Furthermore, older age, male sex, and size of primary tumors have been associated with a higher risk of distant metastasis (15). As for LRNM, larger primary tumor sizes (T) as well as extrathyroidal extensions have been found to correlate with a higher risk of lymph node metastasis (16 –18).
The objectives of this study were to evaluate the current state of our Thyroid Cancer Center's SLNB practice and assess the correlation between primary tumor classification and SLNB outcomes. We hypothesized that larger tumors were associated with a greater risk of having a positive SLNB.
Materials and Methods
Data collection
We performed a retrospective study of all patients operated for a thyroid mass with SLNB at the McGill Thyroid Cancer Center between June 2008 and June 2012. Characteristics such as age, sex, SLNB status, and histopathological features of the primary tumors were retrieved. T classification of the tumor was determined according to the criteria of the American Joint Committee on Cancer (AJCC) staging for thyroid cancer (19).
Inclusion and exclusion criteria
Patients included in this study had a total thyroidectomy, a WDTC on the final histopathology report, and no distant metastasis. We excluded patients who had a benign tumor, a completion thyroidectomy, or a preoperative positive lymphadenopathy.
Surgical approach
All patients were operated on by a single surgeon (R.J.P.). Once thyroid nodules were localized, 0.2 mL of 1% methylene blue dye was injected at 5 and 7 o'clock for small nodules and 12, 3, 6, and 9 o'clock for large nodules, using a 27-gauge, 1.25-inch needle. Little to no nodule mobilization was assured prior to and during the injection to avoid any compromise of lymphatic drainage. Once identified, SLNs were excised and sent for frozen section analysis. Central neck dissections were routinely performed on all patients.
Statistical analyses
All data were tabulated using Microsoft Excel, and all statistical analyses were performed using SPSS v19.0 (IBM Corp., Armonk, NY). Patients were separated into two groups: “positive” SLNB and “negative” SLNB. The two-tailed Pearson chi-square test was performed to compare the descriptive and histopathological findings of both groups, while the Pearson correlation coefficient was used to identify any correlative SLNB predictive factors. For all statistical analyses, p<0.05 was considered statistically significant.
Results
Between 2008 and 2012, a total of 851 patients were operated on for a thyroid mass. Of these, 398 had a hemi- or a total thyroidectomy, 83 had no SLNB performed, and 59 had benign tumors, leaving us with 311 patients eligible for our study.
Patient characteristics
The patient series comprised 263 females (84.6%) and 48 males (15.4%) with a mean age at the time of surgery of 50 years (range 17–87 years). There were 75 patients (24.1%) with a positive SLNB, of which 59 (78.7%) were females and 16 (21.3%) were males, with a mean age of 45 years. Of the 236 patients with negative SLNBs, 204 (86.4%) were females and 32 (13.6%) were males, with a mean age of 51 years. There was no statistically significant difference between the two groups in terms of sex (p=0.105). Dividing the patients according to age (<45 or ≥45 years), 41 of 75 (54.7%) patients with a positive SLNB were younger than 45 years, while only 74 of 236 (31.4%) were younger than 45 years in the negative SLNB group—a statistically significant difference (p<0.001; Fig. 1).
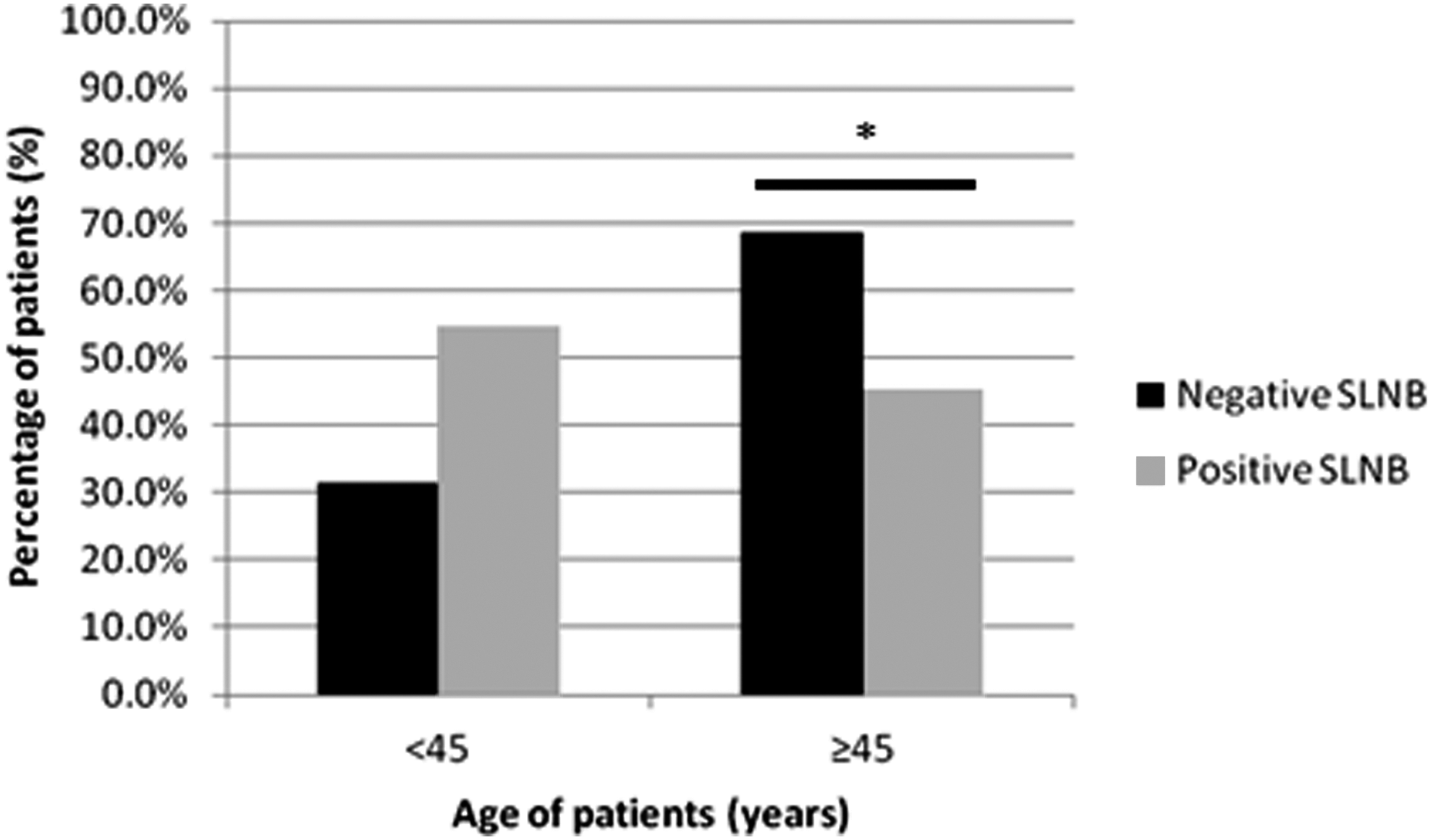
Sentinel lymph node biopsy (SLNB) outcome according to age (<45 or ≥45 years). * indicates statistical significance.
A total of 1906 lymph nodes were resected from this patient series, 1339 (70.3%) of which were from the central compartment. Patients with positive SLNs had 844 lymph nodes resected, of which 513 were from the central compartment, while patients with negative SLNs had 1062 lymph nodes resected, of which 826 were from the central compartment.
A total of 181 SLNs were identified and resected in the 75 patients with positive SLNs, with sizes ranging from 0.1 to 5 cm. These nodes were found 89% of the time in the central compartment, while the remaining 11% were ipsilateral (between levels 2 and 6) to the thyroid nodule. In addition to the 161 SLNs resected from the central compartment, 352 lymph nodes were resected from the central compartment in these patients, of which 88 were positive. An ipsilateral neck dissection was performed in 14 (18.7%) patients, while a bilateral neck dissection was done in 11 patients (14.7%). A total of 331 lymph nodes were resected from these 25 patients with more extensive dissections, of which 89 were positive.
Of the 236 patients with negative SLNBs, 10 (4.2%) had LRNM while having negative SLNs in the final pathology reports, yielding a negative predictive value of 95.7% for this procedure. Of these 10 patients, six had positive nodes in the central compartment, one had positive nodes in the central compartment as well as ipsilateral to the thyroid nodule, two had positive nodes only ipsilateral to the thyroid nodule, and one had positive lymph nodes lateral to the isthmus nodule. A summary of the patient characteristics can be found in Table 1.
SLNB, sentinel lymph node biopsy; T, primary tumor classification.
No parathyroid glands were stained with the methylene blue injection, nor were any patients left with transient skin stains. Transient hypocalcemia was seen in 4% of patients, while there were no cases of permanent hypocalcemia or hypoparathyroidism. Transient vocal cord palsy was seen in 1% of patients, while there was no permanent injury to the recurrent laryngeal nerve (RLN) directly due to surgery. Three patients had permanent vocal cord palsy that was due to RLN tumor invasion, which consequently led to its resection. There were no postoperative cases of hematoma formation in this group of patients.
Primary tumor classification and SLNB
Of the 75 patients with positive SLNBs, 15 (20%) had a T1 class primary tumor, 10 (13.3%) a T2, 35 (46.7%) a T3, and 15 (20%) a T4, while 138 (58.5%) of those with negative SLNBs had a T1, 63 (26.7%) a T2, 32 (13.6%) a T3, and 3 (1.2%) a T4, yielding a statistically significant difference between the two groups (p<0.001; Fig. 2). Likewise, a direct correlation was seen between T class and SLNB outcomes when comparing the two variables (r=0.488; p<0.001). Extrathyroidal extension (ETE) was a statistically significant factor in predicting positive SLNBs, with 46 of 75 (61.3%) patients with positive SLNBs having ETE, as compared to 20 of 236 (8.5%) patients with negative SLNBs (p<0.001).
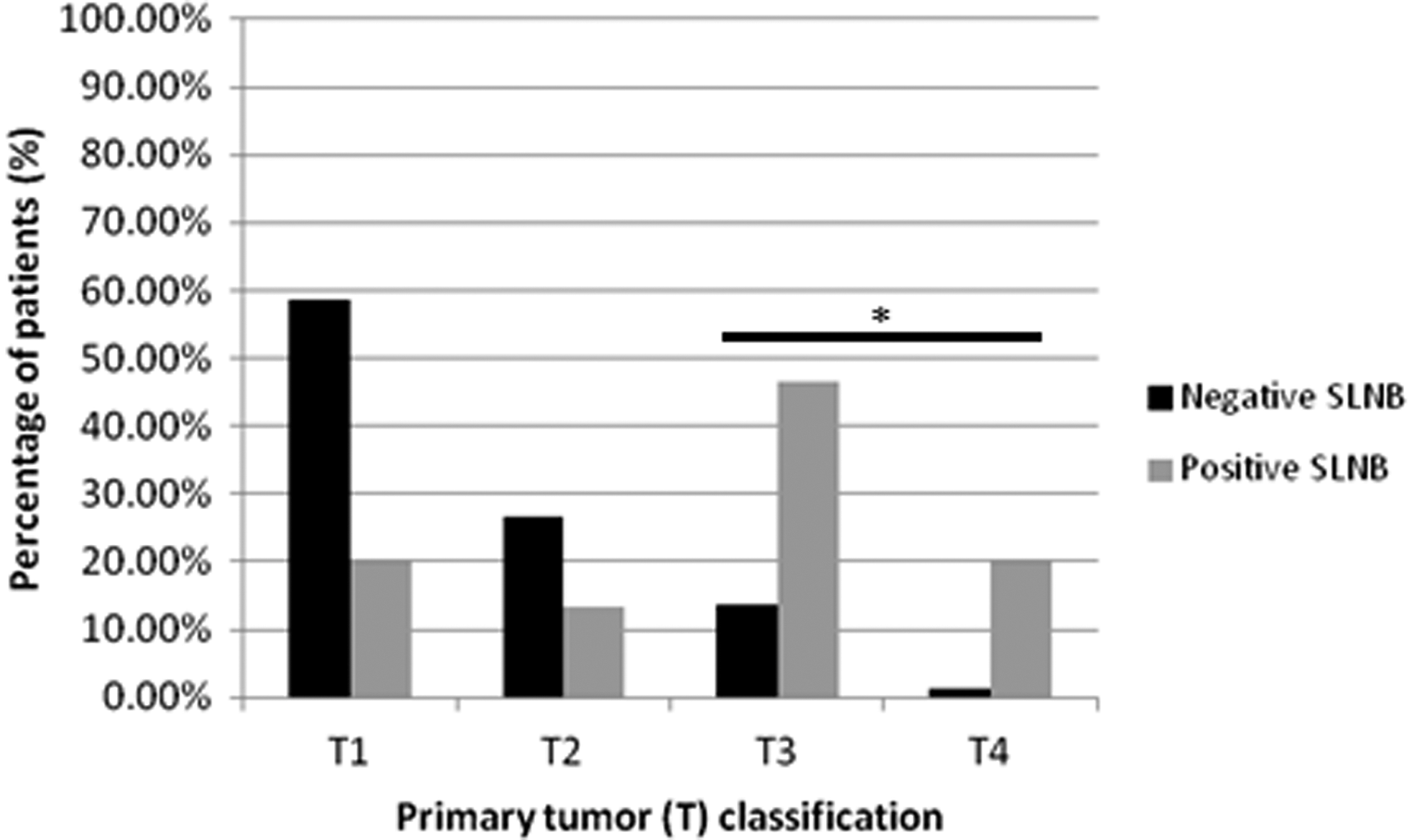
SLNB outcome according to primary tumor (T) classification. * indicates statistical significance.
Discussion
Rate of positive SLNs using the blue dye technique
In this study, 311 patients underwent a total thyroidectomy with a SLNB, of which 24.1% were positive. In a recent meta-analysis on SLNBs for thyroid carcinomas, it was reported that the overall rate of positive SLNBs was 42.8% (20), pooling 16 studies and their results on the methylene blue dye injection technique. Although this rate is significantly higher than the one reported in our study, it is important to note that only 4 of the 16 studies used for the meta-analysis contained more than 50 patients. In fact, the two largest studies of this meta-analysis reported positive SLNB rates closer to ours: 33.6%/107 patients (21) and 36.9%/192 patients (22). To the best of our knowledge, this study contains the largest series of reported SLNBs for WDTC to date, and we believe that the true rate of positive SLNBs is significantly lower than what the current literature brings forth. It is, however, important to note that performing a SLNB at the McGill Thyroid Cancer Center has become the standard of care for all thyroid masses, an approach that may likely differ from other centers where SLNBs are only used for “high-risk” patients. Overall, we believe that the status of the SLNB may be of clinical and surgical importance. Further studies are warranted, though, so as to help understand if SLNB can truly help to determine the extent of thyroid gland resection, whether it be a hemi- or total thyroidectomy, and of nodal dissection, whether it be a unilateral or bilateral central neck dissection, with or without a lateral neck dissection, or no dissection at all.
Predictive factors for positive SLNBs
It has been reported that age and/or sex are associated with LRNM. Some experts have shown that male sex correlates with an increased risk of LRNM (23,24). Others, such as Choi et al. (25), Lee et al. (26), and Cunningham et al. (22), have reported that male patients younger than 45 years were more likely to have LRNM.
In our study, a trend was found toward more positive SLNBs in male patients. With regards to age, there was a statistically significant increased risk of LRNM in patients younger than 45 years. As such, even though this study did look primarily at SLNB outcomes, the association between LRNM in WDTC and the age of the patient remains significant and should be taken into consideration when assessing the risk of LRNM. These findings therefore suggest that performing a SLNB, especially in younger patients, if not on all thyroid masses, provides valuable information on the status of lymph nodes in the central neck compartment.
Primary tumor classification and locoregional metastasis
In this study of 311 patients, we found that the T classification significantly correlated with the outcome of the SLNB. Primary tumor size and ETE have been previously associated with LRNM. Machens et al. have demonstrated that the larger the diameter of the primary tumor, specifically when larger than a T1 (>2.0 cm) (19), the higher the risk of LRNM (27). Similar findings on the elevated risk of local metastasis with larger tumors have been reported in the literature (22 –26,28,29). However, in the present study, the T classification of tumors containing positive SLNBs was not necessarily due to a large diameter (>4.0 cm). Although most patients with positive SLNBs had tumors classified as T3 or T4 (66.7%), only 8 of 75 patients (10.7%) had primary tumors larger than 4.0 cm. The remaining 42 patients had primary tumors between 0 and 4.0 cm but contained ETE, minor or extensive, thus rendering them T3 or T4. Our results are in keeping with previous reports that present ETE as an independent predictive factor of LRNM (25,30) as well as for positive SLNBs (22,31).
Conclusion
Performing a SLNB using the methylene blue dye technique remains an effective and efficient method for the detection of LRNM in patients presenting with WDTC. This study has shown that age (<45 or ≥45 years) is an important predictive factor in determining the risk of having a positive SLNB. Furthermore, the presence of an elevated T class primary tumor, especially with ETE, is directly correlated with the presence of a positive SLNB.
Footnotes
Author Disclosure Statement
No competing financial interests exist.