
Abstract

Graves' disease results in hypothyroidism in about 20% of patients who enter remission after antithyroid drug therapy. Hypothyroidism appears to be caused by two different mechanisms: an inhibitory effect on thyrotropin (TSH) receptor activity due to the presence of TSH-blocking antibodies (TSBAb), and thyroid tissue destruction by the autoimmune process of chronic thyroiditis (1). Here we present a case of Graves' disease evolving rapidly to hypothyroidism and persistent thyroid enlargement. We suggest that this unusual outcome was because of the coexistence of immunoglobulin G4 (IgG4) thyroiditis.
In February 2007, a 47-year-old woman was found to have Graves' hyperthyroidism (free thyroxine >7.80 ng/dL, TSH <0.01 μIU/mL, TSH receptor antibodies [TRAb]=65.6%), and started on methimazole therapy. She continued medication to maintain a euthyroid state for 50 months. Six months after the withdrawal of methimazole therapy, she presented with hypothyroidism (free thyroxine=0.29 ng/dL, free triiodothyronine=1.21 pg/mL, TSH=58.8 μIU/mL). The titers of TRAb, antithyroglobulin antibodies (TgAb), and anti–thyroid peroxidase antibodies (TPOAb) were 75.3 IU/L, >4000 U/mL, and >600 U/mL, respectively. Neck computed tomography showed diffuse enlargement of the thyroid gland (Fig. 1A). Two months after levothyroxine replacement (75 μg daily), thyroid function tests showed subclinical hypothyroidism (free thyroxine=1.10 ng/dL, free triiodothyronine=2.45 pg/mL, TSH=8.3 μIU/mL) with weakly positive TSBAb (48.3%; a cutoff value of 45.6%) but negative thyroid-stimulating antibodies (169%; a cutoff value of 180%). She underwent total thyroidectomy for a persistently large goiter. The weight of the resected thyroid tissue was 282 g. Subsequent histopathological findings of thyroid specimens showed high-grade lymphoplasmacytic infiltration with stromal fibrosis and Hürthle cell changes (Fig. 1B). Immunohistochemical analysis showed approximately 200 IgG4-positive plasma cells per high-power field, with an IgG4/IgG rate of 40% (Fig. 1C). Evaluation of serum IgG4 just before thyroidectomy showed a high concentration of IgG4 (292 mg/dL). Three months after thyroidectomy, levels of serum IgG4 and titers of TRAb decreased to 39.1 mg/dL and 6.3 IU/L, respectively, but TgAb and TPOAb remained above the upper limits of the assay.
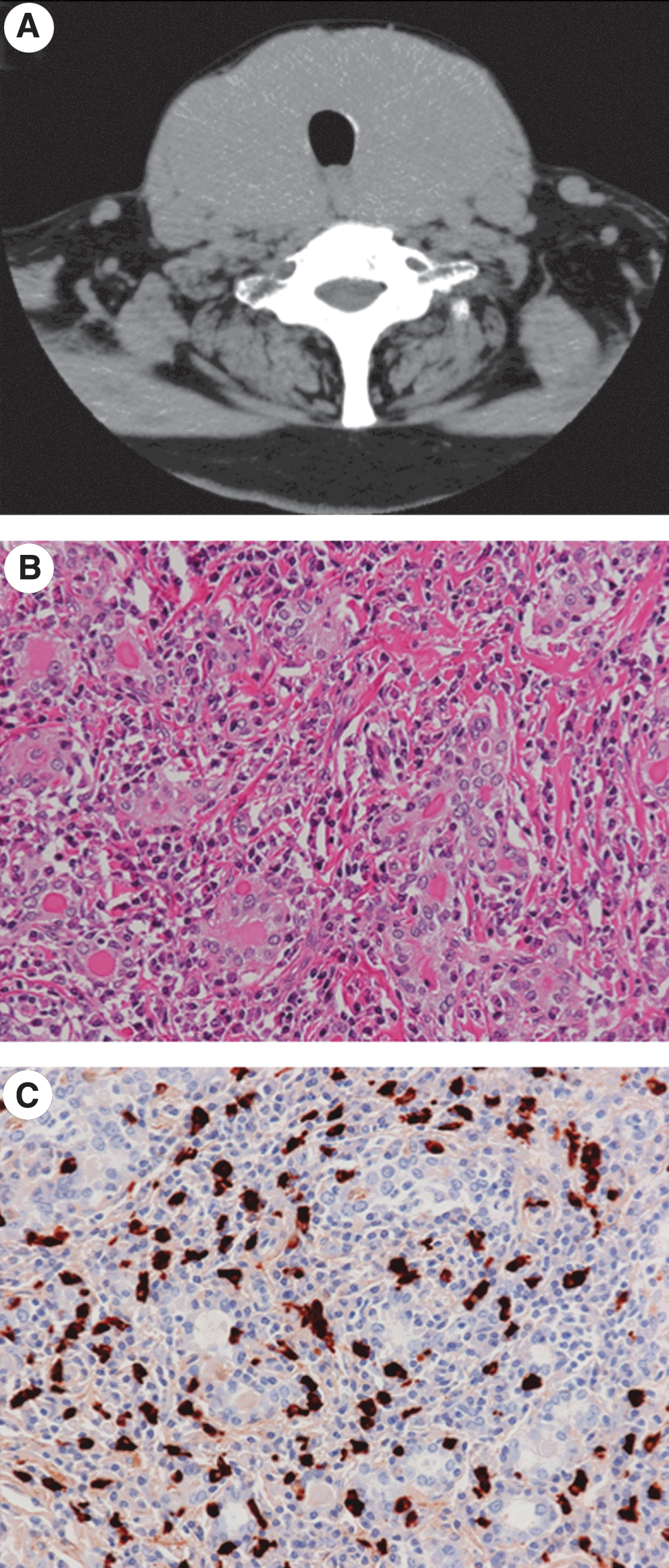
Imaging study and histopathological analysis.
In the present patient, Graves' disease with a large goiter progressed to hypothyroidism shortly after remission. In the presence of high titers of TgAb and TPOAb but weakly positive TSBAb with a large goiter, an autoimmune process of chronic (Hashimoto's) thyroiditis appears to be the main cause of hypothyroidism rather than TSH receptor–blocking activity. In general, the secretion of thyroid hormone in patients with chronic thyroiditis declines slowly, and the rate of progression from subclinical to overt hypothyroidism was reported to be 5% per year in the presence of high titers of antithyroid antibodies (2). TRAb is usually negative when chronic thyroiditis develops into overt hypothyroidism with a persistence of the goiter in the remission of Graves' hyperthyroidism (1). These findings indicate that progressive hypothyroidism with a large goiter in this patient may have been caused by additional factors in combination with chronic thyroiditis. Indeed, a unique immunological feature was defined by the presence of IgG4 thyroiditis based on levels of serum IgG4 and immunohistochemical analysis of infiltrative plasma cells in the thyroid. IgG4 thyroiditis is a recently subclassified category of chronic thyroiditis, and its etiology is still unclear (3). However, the clinical features of IgG4 thyroiditis are significantly associated with lower levels of thyroid hormone, broader areas of low echogenicity, and more rapid progression to a situation requiring thyroidectomy than those of non-IgG4 thyroiditis (3 –5).
Another interesting finding is that the TRAb titer was highly positive, while thyroid-stimulating antibodies and TSBAb were almost negative before thyroidectomy. When a binding assay such as TRAb is positive in a patient with Graves' disease, it usually indicates the presence of thyroid-stimulating antibodies and/or TSBAb; their relative levels determine the extent of stimulation of the TSH receptor. Our data do not allow determining whether the TRAb in this patient are IgG4 produced by the IgG4 plasma cell population. However, the evidence that both the titers of TRAb and the levels of serum IgG4 rapidly decreased after thyroidectomy indicates the possibility of IgG4 binding to the TSH receptor. Although TSH receptor autoantibodies in Graves' disease have been reported to be limited to the IgG1 subclass, both IgG1 and IgG4 can inhibit TSH binding to its receptor (6). If TRAb is indeed of the IgG4 subclass in this patient, Graves' disease itself may be a manifestation of IgG4-related diseases.
In autoimmune thyroid diseases, IgG4 thyroiditis may influence immunoreaction, thyroid function, and the thyroid volume of patients with Graves' disease. We should consider the presence of IgG4 thyroiditis if we encounter high levels of TRAb, progressive hypothyroidism, and persistence of a large goiter in patients with Graves' disease.
Footnotes
Author Disclosure Statement
The authors declare that no competing financial interests exist.