
Abstract
Aim:
We aimed to analyze the prognostic factors affecting disease-specific survival in patients with recurrent and/or metastatic differentiated thyroid carcinoma.
Methods:
Seventy-seven patients with recurrent/metastatic differentiated thyroid carcinoma who were previously treated with total thyroidectomy followed by radioactive iodine therapy were enrolled. Recurrent/metastatic disease was detected by positron emission tomography/computed tomography. At the time of last follow-up (mean 4.8±1.3 years), patients were grouped as having (i) clinical remission (n=17), (ii) stable disease (n=22), or (iii) progressive disease (n=38). We retrospectively examined the prognostic impact of clinical factors (age, sex, TNM stage), histopathological factors of the primary tumor (tumor size, histology, the presence of vascular invasion, extrathyroidal spread, and lymph node metastasis), serum thyroglobulin levels, and metabolic parameters of recurrent/metastatic disease such as radioactive iodine avidity, F18-fluorodeoxyglucose uptake (SUVmax) in metastatic deposits, number and location of F18-fluorodeoxyglucose–avid lesions (locoregional vs. distant), and the impact of surgery on disease-specific survival.
Results:
Lack of vascular invasion (p=0.04), presence of surgically amenable recurrence/metastasis (p=0.0001), and suppressible on-therapy serum thyroglobulin levels at the time of recurrent/metastatic disease (p=0.01) were strong predictors of clinical remission and good prognosis on multivariate analysis. Lesional SUVmax, number or location of F18-fluorodeoxyglucose–avid lesions, and TNM stage did not correlate with clinical outcome. Clinical remission could only be achieved by curative surgery. Patients without curative surgery for recurrence/metastasis had a 43 times higher risk to develop progressive disease than patients with disease amenable to surgery.
Conclusions:
Curative surgery is an essential therapeutic modality to achieve clinical remission in metastatic/recurrent differentiated thyroid carcinoma. Positron emission tomography/computed tomography is a powerful method to detect surgically resectable disease for the selection of patients who may benefit from curative surgery.
Introduction
D
Up to date, several histological and clinical factors are reported to associate with poor prognosis in thyroid cancer patients (2,3). Higher patient age, large tumor size, gross tumor invasion, the presence of bulky distant metastases, and tumor dedifferentiation are the most widely accepted poor prognostic factors (2,3). However, in the absence of these features, prognostication of outcomes in thyroid cancer is difficult, even for patients with wide spread metastatic disease.
In the last decade, F18-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) has proved its value in successfully identifying the site of recurrent or persistent disease in patients who have increased serum thyroglobulin (Tg) levels and negative iodine whole-body scans (WBS). Today, evidence from a growing number of research studies supports the use of FDG PET/CT in the follow-up of patients with DTC limited not only for situations where serum Tg elevation coexists with negative radioactive iodine (131I) uptake, but also for prognostication (5,6). However, the prognostic factors after the diagnosis of FDG PET–positive recurrent and/or metastatic disease on follow-up remain incompletely understood. Moreover, the aggressive nature of these PET-positive DTCs may warrant more aggressive surgical therapy, and this issue is still subject to further evaluation.
The aim of this study was to establish a clinical, histological, and a combined radiological imaging profile to identify prognostic factors associated with clinical outcomes and disease-specific survival in a series of 77 patients treated and followed up in our institution.
Materials and Methods
Seventy-seven patients (32 males and 45 females) with DTC who were previously treated with total thyroidectomy and 131I therapy and have recurrent and/or metastatic disease detected by FDG PET/CT on follow-up were enrolled in this retrospective study. Patients with a prior diagnosis of another malignant disease were excluded from the study.
The TNM staging was performed based on the final edition of the American Joint Committee on Cancer staging manual (7). All patients were previously treated with total thyroidectomy followed by central compartment clearance, 131I therapy for remnant ablation, and thyrotropin (TSH)-suppressive therapy with L-thyroxine (TSH <0.1 mU/L). The cumulative 131I ablation/therapy doses ranged from 5.55 to 55.5 GBq (150–1500 mCi). Five patients received 131I therapy once or twice, whereas others received three or more repeated doses. L-thyroxine replacement was withdrawn 4 weeks before the 131I therapy. Recombinant human TSH was not used because of reimbursement issues. None of the patients had circulating anti-Tg antibodies in this study group. Quantitative measurements of serum TSH, Tg, and anti-Tg antibody levels were performed by chemiluminescent immunometric analysis using an Immulite 2000 System Analyzer (Siemens).
All patients underwent FDG PET/CT imaging one or two weeks after a post-therapeutic 131I WBS in order to detect lesions responsible for elevated serum Tg levels in patients with a negative post-therapy 131I WBS, or to determine disease extent in patients with positive post-therapy scans along with elevated serum Tg levels out of proportion to the identified disease.
Patients were imaged by an integrated PET/CT scanner (Siemens Biograph 6–True Point PET/CT). After fasting for at least 6 hours, all patients were injected 5.3 MBq/kg (144 μCi/kg) F-18 FDG. The blood glucose levels were <150 mg/dL in all patients before FDG injection. PET/CT scan was performed 60 minutes after intravenous FDG injection. Unenhanced CT images were acquired for attenuation correction from the skull vertex to the distal thigh using 3 mm slice thickness and calculated effective milliampere second based on patient weight. The PET and CT images were reviewed on a workstation (Leonardo, Siemens Medical Solutions) visually and quantitatively by two reviewers experienced in interpreting PET/CT scans.
PET/CT findings were proved to be true-positive by histopathological diagnosis in patients who were referred to surgery. In patients with multiple metastases, positive PET/CT findings were correlated with clinical and laboratory findings along with other imaging modalities.
Patient management was performed according to the combined results of clinical findings, post-131I WBS, and FDG PET/CT imaging. On follow-up, physical examination of the head and neck region, neck ultrasonography, and serial measurements of serum Tg, anti-Tg antibodies, and TSH levels were evaluated. PET/CT was repeated on follow-up in 33 patients to confirm or to monitor progressive disease.
Response to treatment was based on combined results consisting of Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria, serum Tg levels (in both on-therapy and off-therapy conditions), post-therapy 131I WBS, and PET/CT studies (8). On the basis of the clinical outcome results, patients were grouped as having (i) clinical remission (n=17), (ii) stable disease (n=22), or (iii) progressive disease (n=38). Patients with clinical remission were re-grouped as patients with complete remission (n=6) and patients with partial remission (n=11). Complete remission was defined as having no evidence of disease on both clinical and radiological examinations along with undetectable off-therapy serum Tg levels (Tg <1 ng/mL). Partial remission was as having serum Tg levels that are suppressible (<1 ng/mL) with L-thyroxine therapy and >10 ng/mL off L-thyroxine therapy, along with no evidence of disease on imaging techniques. Stable disease was defined when there was no significant change in serum Tg levels and in the extent of disease. Progressive disease was defined as at least 20% increase both in disease extent and in serum Tg levels.
We retrospectively examined the prognostic value of sex, age, serum Tg, TNM stage, tumor size, histology, 131I avidity, the presence of vascular invasion and extrathyroidal spread at initial diagnosis, number of FDG-avid metastatic/recurrent lesions, the location of FDG-avid lesions (locoregional or distant), the glycolytic rate of the most active lesion, and the presence of disease amenable to surgery on patient prognosis. “Disease amenable to surgery” was defined as situations in which curative surgery (with no residual tumor) could be performed. Surgical operations in which metastatic deposits could not be completely resected because of scarring from prior surgeries were defined as noncurative surgery.
This study was approved by the ethics committee of our institution.
Statistical analysis
Clinical characteristics and PET/CT findings were analyzed for correlation with outcome data. The chi-square test and the Kruskal–Wallis test were used for univariate analysis of the associations between clinical data, histopathological characteristics, and follow-up results. The Cox proportional hazards model was used to determine the best independent predictors that mostly affected the patients' clinical outcome. p-Values <0.05 were considered to be statistically significant. Disease-specific survival was calculated by using the Kaplan–Meier method.
Results
Clinical characteristics
Detailed patient information is given in Table 1.
FDG, F18-fluorodeoxyglucose; R/M, at the time of recurrence/metastasis; Tg, thyroglobulin.
The mean age of our patient population was 53.7±15 years, with a range of 19–83. Initial clinical TNM stages were as follows: stage I, 23 patients; stage II, 9 patients; stage III, 15 patients; stage IVa, 22 patients; stage IVc, 8 patients. Sixty-four patients had papillary thyroid cancer, six patients had follicular cancer, and seven patients had Hürthle cell carcinoma.
In all patients, serum Tg levels were significantly elevated at the time of final 131I therapy administration (mean stimulated Tg=418.5±1290 ng/mL). Ten patients had positive WBS findings suggestive of disease on the final post-131I therapy WBS, whereas 67 patients had no pathological uptake despite significantly elevated serum Tg levels (227.5±620 ng/mL).
PET/CT demonstrated recurrent or metastatic disease in all patients. PET/CT detected local recurrence in 16 patients, lymph node metastasis in 12 patients, both local recurrence and cervical lymph node metastasis in 9 patients, macronodular lung metastasis in 16 patients, micronodular lung metastasis in 13 patients, bone and soft tissue metastasis in 4 patients, brain metastasis in 1 patient, and multiple sites of metastasis (including lungs, bones, and cervical and mediastinal lymph nodes) in 6 patients.
Detailed information for PET/CT-guided patient management is shown in Figure 1. Based on the PET/CT findings, 55 patients were inoperable because of unresectable local recurrences or widespread metastatic disease. Of these, 13 patients were referred for further 131I therapy, 3 patients received external beam radiation therapy, 8 patients were considered for re-differentiation therapy with peroxisome proliferator–activated receptor agonists, and 31 patients received TSH suppressive therapy with L-thyroxine.
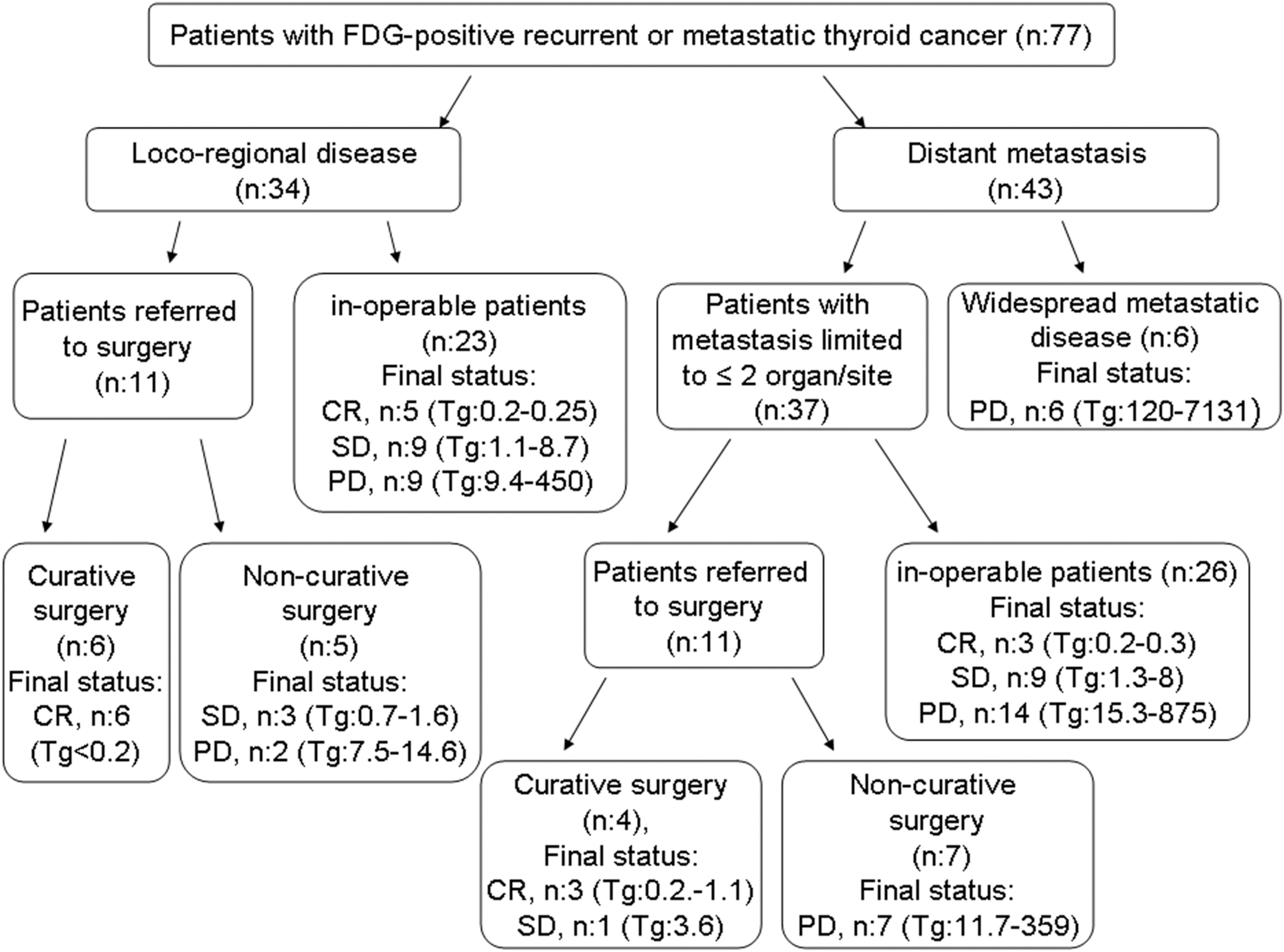
Flow chart with detailed information for PET/CT-guided patient management. CR, clinical remission; FDG, F18-fluorodeoxyglucose; PD, progressive disease; PET/CT, positron emission tomography/computed tomography; SD, stable disease; Tg, final on-therapy Tg (ng/mL).
After PET/CT, 22 patients were referred to surgery (Fig. 1). Among them, 10 patients had disease amenable to surgery based on the PET/CT findings (isolated local recurrence in 6 patients, local recurrence in addition to resectable distant metastasis in 3 patients, and solitary soft tissue metastasis in 1 patient) (Fig. 2). Patients with local recurrence underwent formal central (VI), lateral (levels II–V), or both neck dissections for lymph node recurrence on the basis of preoperative neck ultrasonography and PET/CT findings. The central compartment was explored at the time of re-operation if there was suspected disease. An en-bloc or compartmental neck dissection was preferred unless certain compartments had been previously dissected, or a focused neck dissection or completion compartmental neck dissection was performed. One patient underwent metastasectomy of the solitary soft tissue metastasis after PET/CT.
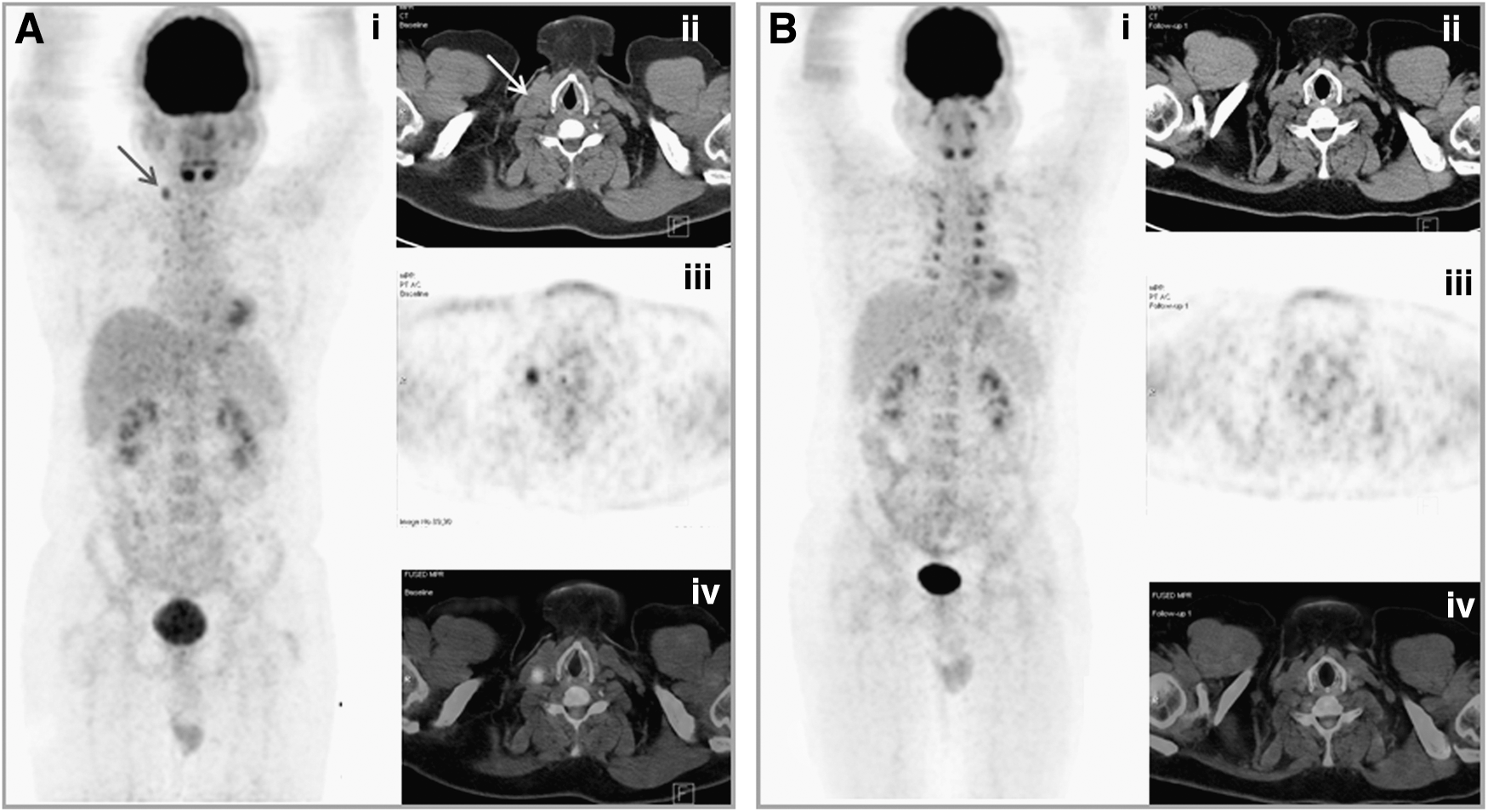
The figure demonstrates two sequential PET/CT scans of a 42-year-old male patient who had been previously treated with total thyroidectomy followed by 100 mCi 131I ablation therapy for papillary thyroid cancer. A biopsy-proven metastasis to right cervical lymph nodes was detected by neck ultrasonography on follow-up.
Among those who were referred to surgery, 12 patients had noncurative or palliative surgery. Of these, all metastatic cervical lymph nodes could not be completely resected because of adhesions originating from previous surgeries in four patients, palliative surgery was indicated because of tracheal obstruction in four patients, and residual mediastinal tumor was left in four patients who underwent metastasectomy for brain and bone metastasis.
The mean follow-up duration after the PET/CT imaging was 4.8±1.3 years. At the time of final follow-up, 17 patients were in remission, 22 patients had stable disease, and 38 patients had progressive disease. Among patients with progressive disease, seven patients died because of cancer-related causes (Fig. 3).

Figure demonstrates two sequential PET/CT scans of a 51-year-old male patient who had been previously treated with total thyroidectomy plus partial tracheal resection followed by 150 mCi 131I ablation therapy for thyroid papillary carcinoma. Serum Tg levels were 0.7 ng/mL on-therapy; neck ultrasonography and 131I diagnostic whole-body scan were negative at the first year of follow-up. However, the Tg level was elevated to 4.9 ng/mL at the second year and a re-staging PET/CT scan was performed.
Results of the univariate analysis
The results of the univariate analysis are summarized in Table 2.
Univariate and multivariate analysis of patient characteristics, primary tumor characteristics, and metabolic parameters.
One patient has limited follow-up data for he died from acute myocardial infarction six months after surgery.
CR, clinical remission; ns, not significant; PD, progressive disease; SD, stable disease.
In this study, we observed that patient age (<45 years vs. >45 years) differed between groups. We observed that the frequency of patients over 45 years of age was significantly higher in patients with progressive disease than in patients with stable disease and patients in remission (p=0.01). The mean age of patients with progressive disease (59.6±14.5 years) was significantly higher than that of patients with stable disease (49.8±14.9 years) and patients in remission (45.5±11.7 years), p=0.002. However, clinical factors such as sex and TNM stage did not correlate with clinical outcome results (Table 2).
The results of the univariate analysis revealed that post-ablation off-therapy serum Tg levels at the time of initial diagnosis did not correlate with clinical outcome results (Table 2). However, serum Tg levels at the time of recurrent and/or metastatic disease differed significantly between clinical outcome groups. Specifically, on-therapy Tg levels were significantly higher in patients with progressive disease than in patients with stable disease and patients who are in clinical remission (283±1150 ng/mL vs. 6.3±6.1 ng/mL vs. 1.9±1.8 ng/mL, respectively; p=0.0001) (Table 2). Similarly, the average of serum Tg levels off L-thyroxine was significantly higher in patients with progressive disease than in patients with stable disease and patients in clinical remission (756.5±1774 ng/mL vs. 104±113 ng/mL vs. 47.8±44.8 ng/mL, respectively; p=0.001).
In terms of histopathological factors, we observed that tumor size, the presence of extrathyroidal spread, and the presence of vascular invasion at initial diagnosis differed among patients groups. The average tumor size was 2.5±1.7 cm in patients with clinical remission and 2.4±1.6 cm in patients with stable disease, whereas it was 4.1±2.1 cm in patients with progressive disease (p=0.03). We observed that the incidence of extrathyroidal spread (p=0.01) and vascular invasion (p=0.001) at initial diagnosis was significantly higher in patients with progressive disease compared with patients with stable disease on follow-up. However, histopathological factors such as tumor type (papillary vs. nonpapillary tumor), presence of lymph node metastases at the time of diagnosis, multifocal tumor, and 131I avidity at the time of detection of recurrent/metastatic disease did not correlate with clinical outcome results (Table 2).
When we compared PET/CT findings with clinical outcome results, we observed that FDG uptake in the most active lesion, the number of FDG-avid metastatic/recurrent lesions, and the location of FDG-avid lesions (locoregional vs. distant disease) did not correlate with clinical outcome results. We observed that SUVmax of the most active lesion was 12.2±9.1 in patients with clinical remission, 7.5±3.9 in patients with stable disease, and 13.6±9.4 in patients with progressive disease. In addition, the number of FDG-avid lesions and the location of disease (whether local recurrence or distant disease) did not differ among patient groups.
In this study, we observed that complete or partial remission could only be achieved by curative surgery. Among patients who had disease amenable to surgery, six had complete remission and three had partial remission on follow-up. One patient died from acute myocardial infarction six months after surgery; hence, follow-up information was limited. Complete or partial remission could not be achieved in the subgroup of patients who could not undergo curative surgery. Of these, nine patients had progressive disease and three patients had stable disease.
Results of the multivariate analysis
A Cox proportional hazards model for progressive disease was performed including factors that have significance on univariate analysis. The results of the multivariate analysis by Cox regression revealed that the lack of vascular invasion at the time of diagnosis (p=0.04), the presence of surgically amenable metastatic disease (p=0.0001), and lower on-therapy serum Tg levels (p=0.01) at the time of recurrence/metastasis continued to be strong predictors of clinical remission and good prognosis in patients with recurrent/metastatic DTC (Table 2). We found that patients without curative surgery for recurrence or metastasis had a 43 times higher risk to develop progressive disease than patients with disease amenable to surgery (p=0.03, odds ratio=42.5 [95% CI 3.3–500]).
The Kaplan–Meier curves for disease-specific survival indicated better outcomes for patients with disease amenable to surgery compared with patients with noncurative or palliative surgery, and inoperable patients (Fig. 4).

The Kaplan–Meier curves for disease-specific survival for patients with recurrent/metastatic thyroid cancer.
Discussion
Metastatic thyroid cancer represents a heterogeneous disease with different outcomes. The presence of distant metastases at initial diagnosis is a negative prognostic factor in all staging systems for DTC. However, there are no provisions to restage or update the prognosis assessment schemes when recurrence or metastases develop on follow-up. We believe that patients with metastatic thyroid carcinoma must be accurately characterized concerning all clinical, histopathological, and metabolic prognostic indicators. In this regard, we aimed to shed additional light on this issue to better define indicators related to poor prognosis in patients with recurrent/metastatic DTC.
In this study, we retrospectively analyzed clinical outcome results of 77 patients with FDG-positive recurrent and/or metastatic thyroid cancer for clinical, histopathological, and metabolic factors that may be associated with poor prognosis. The majority of our patients (87%) had 131I-refractory thyroid carcinomas with non-131I avid tumors and positive FDG uptake. One may argue that this may lead to a selection bias. However, this study consisted of patients who were previously treated with total thyroidectomy followed by one or more cycles of 131I therapy that generally exceeded 22 GBq (600 mCi) and recurred or metastasized on follow-up. Thus, the higher incidence of patients with 131I-refractory tumors seems acceptable in this patient population (9). Another remarkable point to consider in our patient population is the higher frequency of some well-established poor prognostic factors compared to DTC at large (Table 1). As the present study consisted of DTC that recurred or metastasized on follow-up, we considered that these higher frequencies were not co-incidental in our patient population.
In this study, we observed that the presence of vascular invasion in the primary tumor at the time of initial diagnosis, high serum on-therapy Tg levels at the time of FDG-positive metastatic/recurrent disease, and the presence of surgically unresectable disease were associated with progressive disease on follow-up.
Our results show that, among histopathological characteristics of the primary tumor, only the presence of angioinvasion correlated with poor prognosis in metastatic/recurrent DTC. In the literature, there are conflicting results on the prognostic value of vascular invasion in patients with DTC (10 –13). Even though several reports have suggested that angioinvasion is not predictive of poor prognosis in thyroid carcinomas, pathologists agree that the controversies on this issue derive from the inappropriate identification of angioinvasion in DTC (11 –13). The results of recent research indicate that the application of rigid criteria to identify vascular invasion predicts distant metastasis in patients with thyroid carcinomas, especially in well-differentiated thyroid carcinomas. Mete and Asa (11) found that nearly 30% of angioinvasive well-differentiated thyroid carcinomas and 1/2 of angioinvasive poorly differentiated thyroid carcinomas developed distant metastases on follow-up.
In this study, we observed that sex, TNM stage, the presence of multifocal tumor, and lymph node metastasis at initial diagnosis were not related with progressive disease on univariate analysis. Even though age at the time of initial diagnosis, tumor size, and extrathyroidal spread of the primary tumor were found to have significant correlation with progressive disease on univariate analysis, the results of the multivariate analysis revealed that these factors did not associate with poor prognosis.
Extrathyroidal spread was previously found to correlate with FDG-avid recurrent/metastatic disease on follow-up by our group (6). Similarly, Spriano et al. (14) reported that extracapsular spread with margin infiltration was a predictive factor of either distant metastasis or regional recurrence in their series with 1503 patients with DTC. We considered that the presence of extrathyroidal tumor spread seems to lose its prognostic power when evaluated by multivariate analysis in combination with many parameters.
In this study, we observed that the intensity of FDG uptake, in terms of SUVmax, did not associate with clinical outcome results of our patients with FDG-avid tumor recurrence. Today, it is widely accepted that FDG uptake in thyroid cancers parallels with the loss of differentiated features and associates with aggressive clinical behavior (5,6,15). Both progression-free survival and overall survival decrease in patients with FDG-avid recurrent tumors compared with FDG-negative recurrence (6,15). In this regard, one may think that our findings are in contrast to previous reports. However, for the current study, only patients with FDG-avid recurrent tumors were enrolled and we did not specifically compare FDG-avid recurrent lesions versus non-FDG-avid tumors. We considered that once thyroid cancer recurs or develops distant metastasis on follow-up, from the metabolic point of view, the important prognostic indicator is the presence of FDG avidity itself, not the intensity of the FDG uptake.
In addition, our results indicate that neither the location of FDG-avid tumor recurrence (local recurrence vs. distant disease) nor the number of FDG-avid lesions associated with clinical outcome results. These findings may seem contradictory to previous reports (5). Robbins et al. (5) reported that the number of FDG-avid lesions in the initial PET scan significantly correlated with survival in patients with DTC. However, our study differs widely from the latter one in patient population (patients with FDG-positive recurrence/metastasis in the current study vs. all patients with DTC), the timing of PET/CT (restaging vs. staging), and the FDG-positive lesions (recurrent tumor vs. primary tumor). Moreover, in the current study, we evaluated the influence of surgery after the detection of metastatic disease on patient prognosis. We found that if completely resectable by surgery, the presence of disease, either local recurrence or distant metastasis, does not seem to inversely affect patient prognosis.
We observed that after the detection of 131I-refractory tumor recurrence, having disease amenable to surgery is an independent prognostic indicator on clinical outcome. Clinical remission could only be achieved by curative surgery. In addition, among patients who could not have curative surgery, 75% had progressive disease, whereas 25% of these patients survived with stable disease. The risk of developing progressive disease was 43 times higher in patients without curative surgery than in patients with disease amenable to surgery. Moreover, disease-specific survival was comparable between patients with noncurative surgery and inoperable patients with widespread disease (Fig. 1).
Surgery is considered first-line therapy in locoregional recurrence or gross nodal involvement. Selective neck dissection for lymph node recurrence is usually the preferred procedure in terms of treating locoregional recurrence. When certain compartments have been previously dissected, a focused neck dissection or completion compartmental neck dissection might be considered (16,17). However, the benefit of surgically removing small-volume metastatic lymph nodes still remains controversial (18). Despite the best surgical efforts, recent studies report that biochemical remission can be reached only in one-third of patients (16). Furthermore, to prevent future locoregional complications, the American Thyroid Association guidelines recommend surgical removal of only clinically significant metastatic lymph nodes (18 –20).
Studies have shown that cytoreductive surgery is associated with decreased recurrence and improved survival (21). However, it must be kept in mind that more scarring is generated in the operating field after each neck exploration, which makes each subsequent re-operation more difficult and increases the risk of morbidity. Even though we did not evaluate surgical complications specifically, we believe that the decision for re-operative neck dissections should be balanced between surgical complications and patient-based expectancy to achieve clinical and biochemical remission. In addition, we considered that if the identified disease is not suitable for curative surgery, noncurative surgery does not prolong disease-specific survival in patients with advanced thyroid cancer; however, it may have significance to palliate disease-specific symptoms.
We observed that serum Tg levels under TSH suppression at the time of recurrent/metastatic disease was another independent prognostic indicator for favorable clinical outcomes. However, Tg levels in off L-thyroxine at the time of recurrent/metastatic disease did not correlate with outcome results. In a recently published study, our group showed the prognostic importance of the “suppressibility of Tg levels” by L-thyroxine despite significant elevation in off-therapy state (6).
In general, high pre- and postablation initial Tg levels are known to correlate with nonfavorable prognosis. In this study, we found that initial off-therapy Tg levels did not correlate with clinical follow-up results. However, it is remarkable that all patients had significantly high initial off-therapy Tg levels with an average of 321.6±1245.7 ng/mL in our patient population. Therefore, we could not compare the prognostic value of high versus low Tg levels. We considered that, regarding these initial high Tg levels, despite aggressive 131I therapies and close monitoring, recurrence on follow-up was not unexpected in our patient population. We considered that, if the detected disease was amenable to surgery and Tg levels could be suppressed by L-thyroxine replacement, the degree of initial high Tg levels did not affect disease-specific survival.
Metastatic thyroid cancer represents a heterogeneous disease with different outcomes. The current literature contains several studies that indicate different results for survival data and prognostic indicators in patients with thyroid cancer. Nevertheless, there are no precise risk stratification schemes for the management of patients with DTC that adequately incorporate the prognostic implications of detailed pathological features and the molecular biological profiles of the primary tumor.
Today, in patients with 131I refractory thyroid cancer, the current literature points out several molecular abnormalities that may represent potential targets for individualized targeted therapies (9,22). We believe that by improving the knowledge of targets present in each individual tumor and by increasing the experience with the use of these drugs directed against each of these targets, thyroid cancer patients may benefit from personalized selection of therapies.
We believe that the strength of our study derives from the multifactorial analysis of the studied parameters in association with clinical outcome results. Even though recurrent lesions and metastatic deposits may not be identical to the primary tumor in clinical behavior and biological characteristics, the results of this study demonstrate that patient management strategies must include all data from patient history along with all information obtained from imaging techniques and clinical findings.
In conclusion, we found that curative surgical treatment and suppressible on-therapy Tg levels are independent prognostic indicators after the onset of metastatic and recurrent disease. Clinical remission can be reached only by curative surgery especially in patients with 131I-refractory aggressive tumors. Through the identification of disease amenable to surgery, FDG PET/CT provides a unique and important information to select patients who will benefit from curative surgery.
Footnotes
Author Disclosure Statement
The authors declare that they have nothing to disclose. They do not have any research grants, fund, or any other financial support. They have no conflicts of interest.