
Abstract
Background:
Rodents with gestational thyroid-hormone (TH) deficiencies and children with congenital hypothyroidism show abnormal hippocampal development. Given that the human hippocampus starts to develop early in gestation, we asked if children born to women with hypothyroidism during pregnancy also show hippocampal abnormalities and if this is related to the severity of maternal TH insufficiency and current memory functioning. We additionally sought to determine whether effects were more prominent in anterior or posterior hippocampal subsections given these support different memory functions and have different developmental trajectories. We hypothesized that these children would have smaller than normal hippocampal volumes than controls and show memory deficits on both standardized tests and indices of “everyday” memory functioning.
Methods:
We studied 54 children aged 9 to 12 years: 30 controls and 24 HYPO cases—offspring from women diagnosed with hypothyroidism prior to or during pregnancy and treated with
Results:
HYPO cases showed significantly smaller right and left hippocampal volumes than controls, particularly in right posterior and left anterior segments. In HYPO children, hippocampal volumes were negatively correlated with maternal third-trimester TSH levels and positively correlated with third-trimester fT4. HYPO cases scored significantly below controls on one objective and several subjective memory indices, and these were correlated with hippocampal volumes.
Conclusion:
Early TH insufficiency from maternal hypothyroidism affects offspring hippocampal development and memory.
Introduction
D
Animal models of gestational hypothyroidism have shown the rodent hippocampus is particularly vulnerable to early TH loss (11 –15), and this contributes to learning and memory impairments (16 –18). Along the same lines, children with congenital hypothyroidism (CH), who experience a late gestational/early infancy loss of TH, show selective memory deficits (19,20) and structural and functional hippocampal abnormalities (20,21). However, it is not known if offspring of women with hypothyroidism during pregnancy (HYPO cases), who are exposed to an earlier developmental period of TH insufficiency than children with CH, are similarly affected. Given evidence showing that fetal hippocampal development starts very early in gestation (22,23), there is reason to suspect that the hippocampi of offspring of hypothyroid women will also be compromised.
To address these outstanding issues, we conducted an exploratory study comparing hippocampal volumes and memory performance in HYPO cases versus children serving as controls who were born to women with normal thyroid function in pregnancy. In light of recent findings that anterior and posterior hippocampal segments support distinct memory functions, particularly anterior for encoding new information and posterior for recollecting or reconstructing past memories (24,25), and that these segments have different developmental trajectories (26), we also compared anterior and posterior hippocampal volumes in HYPO versus control groups. In addition, we examined the relations between severity of maternal hypothyroidism and the child's hippocampal size and memory. We hypothesized that HYPO children would have smaller hippocampi and reduced functioning on hippocampally mediated memory tasks relative to controls and effects would be correlated with severity of maternal hypothyroidism.
Materials and Methods
Participants
We studied 54 children—24 HYPO and 30 controls—born between 1996 and 2001 and aged 9–12 years (mean±standard deviation, 10.2±0.69). All were part of a larger cohort followed longitudinally on a regular basis until early adolescence. Exclusion criteria were exposure to alcohol or other teratogens during pregnancy, head injury, neuroradiological abnormality, or major health problem.
The HYPO group, representing ∼30% of the original birth sample, included 24 children born full term to 23 women diagnosed with hypothyroidism prior to or during pregnancy (n=6); one woman contributing two children born two years apart was hypothyroid in both pregnancies. Most women were recruited via local endocrinologists and obstetricians during or right after pregnancy. The remainder was solicited soon after the child's birth from the Motherisk program at The Hospital for Sick Children (SickKids), an antenatal counseling service for prenatal medication exposures (including L-T4). As part of recruitment to our cohort originally, all women were contacted by telephone and admitted to the study only if they had not received an L-T4 dose increment, as was the case in 1996–2001 because knowledge to increase the dosage during pregnancy was not widely known (27). Current cohort participants had comparable birth weights, gestational ages, and sex distributions as nonparticipants. Similarly, mothers of current participants did not differ in TH levels, socioeconomic status, and educational levels from those not participating now. TH levels were available from 22 pregnancies, 19 of which involved an elevated thyrotropin (TSH) level during at least the first half of pregnancy. One woman had elevated TSH values in the second and third trimesters only, while three women had normal levels of TSH and fT4 throughout pregnancy. The mean dose of L-T4 during pregnancy was 105±39 μg (range: 50–200 μg).
Controls were 30 typically developing youth born full term in the same period as the HYPO group. Most were recruited from birth lists of a Level 1 neonatal nursery at a local hospital, while the remainder was recruited through the Motherisk database for women who called the service regarding exposure to a nonteratogenic substance (e.g., acetaminophen) during pregnancy. A handful was also recruited by a local obstetrician who performed TH function tests and solicited women with normal results for this study. Based on interview and questionnaires provided throughout the study, none of the mothers of control participants reported having hypothyroidism during pregnancy or developing it later, and none of their children had a learning disability or attention disorder.
Procedures
As part of a larger study of the hippocampus and memory, all children were initially seen for a neuropsychological assessment and subsequently for a one-hour magnetic resonance imaging (MRI) scan during which structural and functional sequences (functional reported elsewhere) were performed. Parents first provided written consent, while children gave informed oral assent. Testing, which took place in the Psychology Department at SickKids and lasted about three-and-a-half hours, included measures of intelligence, reading, attention and executive functioning (not reported presently), and a comprehensive battery of memory tests. Parents completed several behavioral questionnaires assessing the child's everyday memory functioning. Scanning, which took place four to six months later, was done in a 1.5 Tesla Signa GE magnet in the Diagnostic Imaging Unit at SickKids. Participants viewed movies via MRI-compatible goggles, an effective device for reducing motion, during the structural sequences.
After both sessions, participants received a movie pass and certificate of participation and, after the scan, a CD of several of their own brain slices. Parents were compensated for all travel expenses. Within two months of the assessment, parents received a clinical report describing the child's neuropsychological test findings. A staff neuroradiologist masked to group status reviewed all MRI images for evidence of neuroradiological abnormalities and a report was sent to each child's pediatrician or family physician. The Research Ethics Board at SickKids and Office of Research Ethics at the University of Toronto approved all procedures.
Test instruments
Intelligence was assessed with the Vocabulary and Matrix Reasoning subtests of the Wechsler Abbreviated Scale of Intelligence (WASI) (28) and reading ability with the Wide Range Achievement Test (WRAT-3) (29). Memory was evaluated with standardized instruments having excellent psychometric properties, and these included selective subtests from the Children's Memory Scale (CMS) (30), the Rey–Osterrieth Complex Figure test (ROCF) (31), and the entire Test of Memory and Learning (TOMAL) (32). The three CMS subtests were: (i) Dot Locations, which require children to learn the locations of markers in a grid and remember them over time; (ii) Stories, which require listening to a story and reiterating it immediately and after a 20-minute delay as well as recognizing story facts; and (iii) Picture Locations, which shows an array of objects in different grid locations and requires participants to point where objects are in an empty grid. The ROCF requires copying a complex abstract design and reproducing it after a 20–30-minute delay. The TOMAL provides a comprehensive memory assessment, which is highly predictive of memory dysfunction in children with brain damage or developmental disabilities (32 –34). TOMAL subtests are: (i) immediate and delayed Word Selective Reminding (WSR), which requires learning a list of words and, after each trial, being reminded of ones forgotten; (ii) immediate and delayed Visual Selective Reminding, which is similar to WSR but requires remembering objects; (iii) Forward and Backward Digit Span; (iv) immediate and delayed Face Memory, which shows a face and requires recognizing it among distracters; (v) Object Recall, which shows pictures of objects and requires naming them later; (vi) Paired Recall, which requires learning and recalling word pairs; (vii) Abstract Visual Memory, which shows an abstract figure and requires finding it among distractors after a delay; and (viii) Visual Sequential Memory, which requires learning and remembering the order of presentation of a series of geometric designs. In all tasks, higher scores signified better performance.
Parents completed three questionnaires: (i) a demographic history form seeking information on the child's birth and developmental history, current health and school status, family history, and parental education level and occupation (for computing socioeconomic status); (ii) the Behavioral Rating Inventory of Executive Function (BRIEF) (35); and (iii) the Everyday Memory Questionnaire (EMQ) (36). The BRIEF is an 86-item questionnaire evaluating multiple aspects of executive function such as shifting, inhibition, working memory, and planning. In the current study, only the Working Memory subscale enquiring about daily memory functioning was examined. The EMQ is a 28-item questionnaire requiring parents to rate the child's daily memory difficulties on a nine-point scale from 1 (not at all in the last 3 months) to 9 (more than once a day). EMQ scoring provides a total score and scores for five factors: retrieval (e.g., forgets when something happened); task monitoring (unable to follow thread of a story); conversational monitoring (repeats what was said before); spatial memory (gets lost where they often have been before); memory for activities (forgets change in daily routines) (37). Both the BRIEF and EMQ have been extensively validated on children spanning a broad age range, while the EMQ has also been shown to correlate with hippocampal size in children born preterm (38). For both questionnaires, higher scores signify more memory problems.
Image acquisition and processing
Structural images were collected using a 3D FSPGR (IR prep Zip X2) T1-weighted series in the axial plane (TR=10.37 ms, TE=4.26 ms, TI=400 ms, flip angle=20°, field of view=240 mm, slice thickness=1.50 mm, no gap). First processing steps involved extracting the brain from the skull and cerebral spinal fluid, and normalizing the extracted brain in standard space using anterior and posterior commissure alignment.
The traced hippocampal region included the cornu ammonis regions (CA1–CA4 fields), dentate gyrus, and subiculum (Fig. 1). All tracings were carried out manually on a slice-by-slice basis in ANALYZE 9.0 (AnalyzeDirect, Inc., Overland Park, KS). A trackball cursor was used to outline hippocampal boundaries in coronal images from anterior to posterior, beginning at the rostral end when the hippocampal head first appears below the amygdala and ending where the crura of the fornices depart from the hippocampal tail. Sagittal images served to verify hippocampal boundaries and delineate the inferior boundary of the hippocampus from the parahippocampal gyrus. Each hippocampus was further subdivided into anterior (hippocampal head) and posterior (hippocampal body and tail) segments along the coronal axis using the uncus as an unambiguous dividing marker according to established procedures (39). In addition to absolute right and left hippocampal volumes, we also computed total intracranial volumes (ICV) in SPM-5 and determined ICV-adjusted hippocampal proportions.
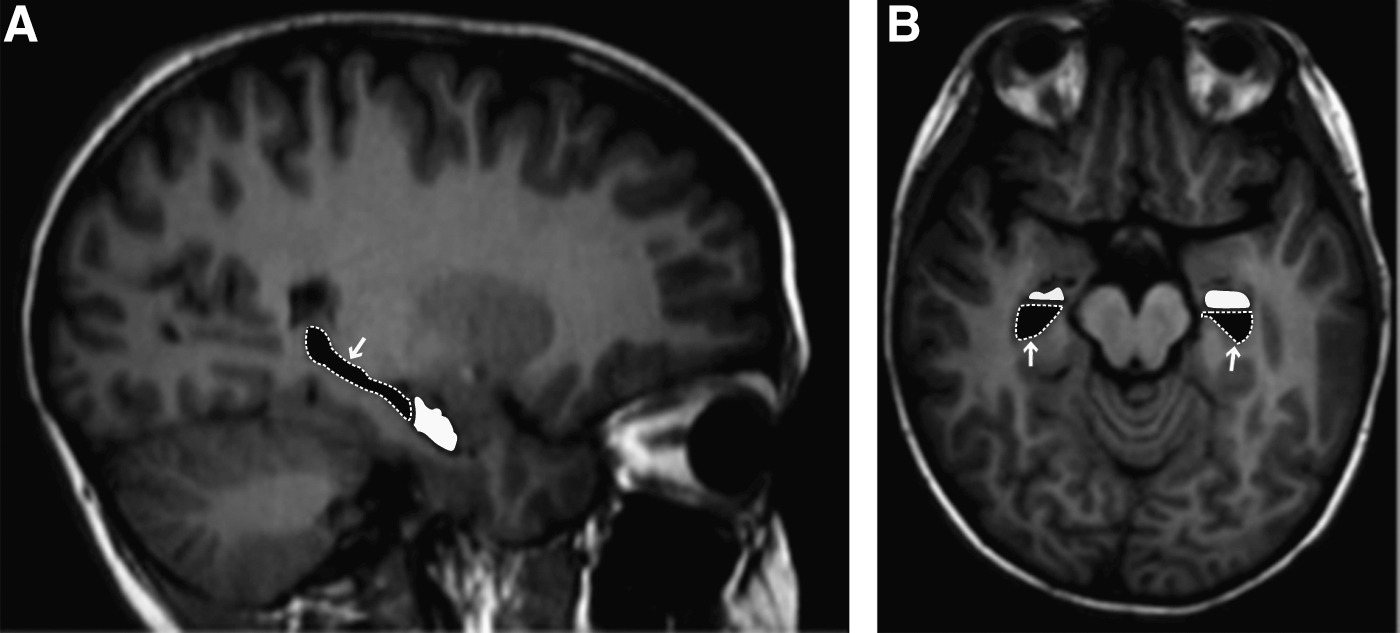
Manual tracings of anterior (white) and posterior (black, indicated by white arrows and dashed outline) hippocampal subregions for a control subject:
One image analyst masked to group status traced all left and right hippocampi, and a second analyst traced a subset of scans for reliability purposes. Inter-rater reliabilities were 93% for the left hippocampus and 86% for the right.
Data management and statistical plan
No child was missing any memory data. Two HYPO cases lacked scan data, one due to excessive motion and the other because of a newly implanted metal retainer not reported to us until the day of scanning. In both cases, mothers lacked TH data, signifying only one mother of children with acceptable scan data was lacking TH information. Because the three women treated for hypothyroidism had normal TH values throughout pregnancy and thus were not technically hypothyroid during pregnancy, their children were not included in the comparisons with controls but were included in the correlation analyses to allow a broader range of maternal TH values.
All analyses were conducted using SPSS version 20 software (IBM, Armonk, NY). Demographic data were analyzed using chi square and t-tests. Group differences in hippocampal volumes were examined by (i) multivariate analyses of covariance (MANCOVA) on absolute volumes with ICV as the covariate and (ii) multivariate analyses of variance (MANOVA) on the proportional volumes. Separate MANCOVAs and MANOVAs were used in comparing total right and left hippocampi versus the four subsegments. To reduce number of comparisons for the memory-test data and obtain overall results per instrument, we performed MANOVAs within CMS, ROCF, and TOMAL instruments and for BRIEF and EMQ questionnaires combined. Significance was set at p<0.05.
We also carried out a number of exploratory correlation analyses to investigate relationships among key variables of hippocampal size, memory performance, and maternal thyroid function. To assess relationships between hippocampal size and trimester-specific maternal TH levels, we performed both first-level correlations and partial correlations controlling for ICV on the raw hippocampal volumes. To assess the relationships between hippocampal size and memory, we performed first-level correlations by group between raw hippocampal volumes and memory indices. Although mindful of further Type 1 error inflation, we did not exercise strict control for multiple test comparisons, as we were primarily interested in these for generating future hypotheses. However, we set the p-value at 0.01.
To identify which of the hippocampal segments were contributing most strongly to memory results, we used stepwise linear regression analysis. Our approach involved entering group first followed by the four hippocampal segment sizes together. The p-value was set at 0.05 in these analyses.
Results
Demographics
Table 1, which presents the demographic data for HYPO and control groups, shows no group differences in sex, age, birth weight, school grade, hand preference, maternal age or education, socioeconomic status, or number of siblings. Although HYPO scored below controls on IQ and reading, differences were not significant. In the HYPO group, 8.3% had a learning disability, and 12.5% had attention deficit hyperactivity disorder (ADHD) compared with none for controls, which was not significantly different.
Results expressed as mean±standard deviation (SD) or as percentage.
Rated on a five-point scale whereby 5=graduate or professional school, 4=completed university, 3=some university or college, 2=completed high school, and 1=not completed high school.
Based on the Hollingshead scale, whereby 1=highest social class.
HYPO group, offspring of women with hypothyroidism during pregnancy; SES, socioeconomic status; WASI, Wechsler Abbreviated Scale of Intelligence; IQ, intelligence quotient; WRAT, Wide Range Achievement Test; ADHD, attention deficit/hyperactivity disorder.
Table 2, which presents mothers' trimester-specific TH values, shows that the majority of women had TSH values significantly above the pregnancy-level cutoff range (40), especially in their first and second trimesters of pregnancy.
Data are based on 21 cases (excludes 3 cases whose mothers' TH levels were normal in pregnancy). Cutoffs for TSH set at 2.5 mU/L for trimester 1, 3.0 mU/L for trimester 2, and 3.5 mU/L for trimester 3.
TSH, thyrotropin; fT4, free thyroxine.
Hippocampal volumes
Groups did not differ in ICV: HYPO=1781.4±178.6 mm3; control=1738.8±144.5 mm3 (p=0.56). However, because ICV was strongly correlated with both right (p=0.001) and left (p=0.005) hippocampal volumes, we used ICV as a covariate in between-group comparisons of hippocampal volumes. Since results were almost identical for raw hippocampal volumes versus ICV-adjusted proportion data, we report here raw-volume results only. Mean volume data are shown in Table 3. MANCOVA revealed a significant overall group difference (p=0.04) while post hoc univariate analyses indicated right and left hippocampi were both significantly smaller in the HYPO group (p=0.012 and p=0.019), reflecting 8.2% and 7.1% reductions, respectively. A similar group comparison on the four hippocampal segments showed right-posterior (p=0.03) and left-anterior (p=0.04) subregions were significantly smaller in the HYPO group.
Data are based on 19 cases (excludes 2 cases which lacked scan data and 3 cases whose mothers' TH levels were normal in pregnancy).
ns, not significant.
To explore the relations between maternal hypothyroidism severity and child's hippocampal size, we performed simple correlations between maternal TH values from each trimester using the entire HYPO sample (see justification above). For the right hippocampus, results revealed significant negative correlations with maternal TSH values from second (r=−0.472, p=0.04) and third trimesters (r=−0.599, p=0.01). For the left hippocampus, only a negative trend-level association with maternal third-trimester TSH was observed (p=0.075). There were no correlations with maternal fT4 levels.
When we repeated these analyses on the individual segments, we observed several significant correlations with the size of the right-anterior segment (Fig. 2). Specifically, this segment was smaller if mothers had higher third-trimester TSH (r=−0.678, p=0.004) and lower third-trimester fT4 levels values (r=0.721, p=0.029) while a trend-level effect was observed with maternal second-trimester TSH (r=−0.388, p=0.101). Although close examination of the data suggests these effects may have been driven by the child born to the women whose TSH was very elevated in late gestation, the effect persisted at a modest trend level (p=0.12) when this analysis was repeated without this participant, accounting for 18% of the variance in hippocampal segment size. Furthermore, as this child's mother lacked a third-trimester fT4 value, he and his mother did not contribute to the positive association between fT4 and size of the right-anterior segment.
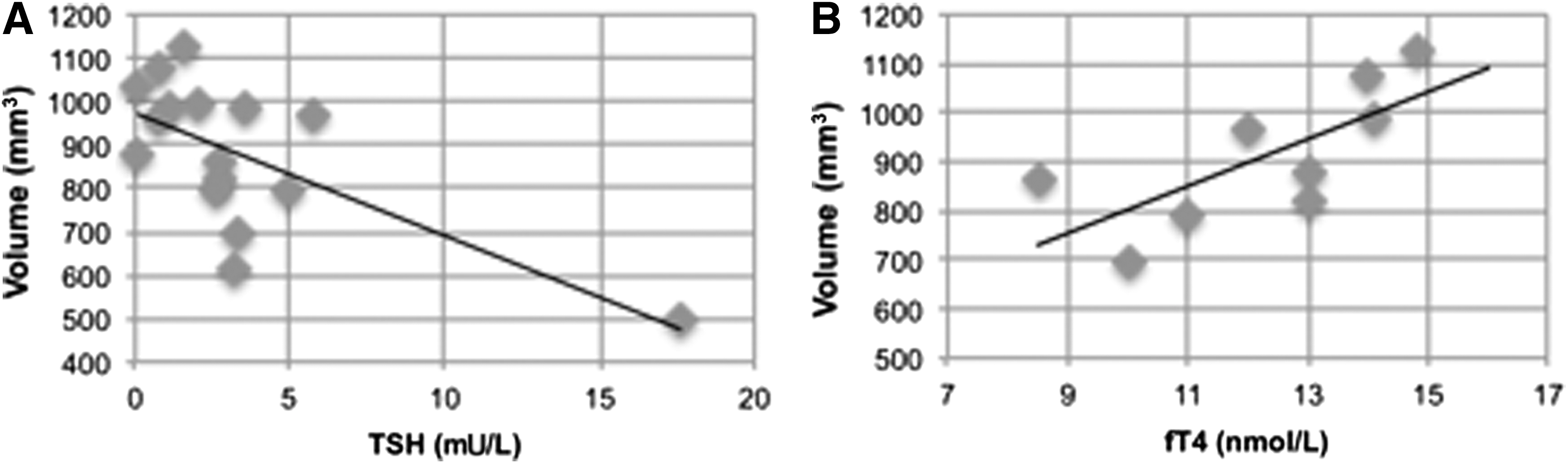
Regression of right anterior hippocampal size by maternal third-trimester levels of
Memory performance
To assess whether groups differed in memory, we performed separate MANOVAs for each of the three clinical instruments and for questionnaire data. Results revealed an overall group effect for questionnaire data (p=0.006) but none of the three memory test instruments (Table 4). The only memory subtest on which the HYPO group performed significantly (p=0.05) below controls was TOMAL WSRT. Regarding questionnaires, the HYPO group received higher problem rating scores on the BRIEF Working Memory Scale (p=0.036) and the EMQ (p=0.036), particularly on EMQ subscales pertaining to memory for past events (p=0.024) and monitoring current conversations (p<0.001).
Scores from three HYPO cases whose mothers' TH levels in pregnancy were normal are removed.
Scores presented as scale scores (mean±SD, 10±3).
Scores presented as raw scores (mean±SD).
BRIEF, Behavioral Rating Inventory of Executive Function; EMQ, Everyday Memory Questionnaire.
Correlations were performed between memory test data and maternal TH levels. Given the large number of indices of memory, we set the p-value at 0.01 for significance. The only tests showing significant effects were the ROCF and TOMAL. The findings reflect: (i) a negative correlation between ROCF delayed recall scores and second-trimester maternal fT4 (r=−0.668, p=0.013); (ii) a positive association between TOMAL delayed Visual Selective Reminding and third-trimester maternal fT4 levels (r=0.736, p=0.01); (iii) negative correlations between TOMAL Face Memory performance and second- and third-trimester maternal TSH levels (r=−0.543, p=0.01, and r=−0.648, p=0.007); (iv) a negative correlation between TOMAL Abstract Visual Memory and third-trimester maternal TSH (r=−0.682, p=0.004) and at a trend-level for second-trimester maternal TSH (r=−0.453, p=0.05). There were no significant correlations for the CMS test or questionnaire data.
Structure/function correlations
To examine the relations between hippocampal size and memory, we performed separate series of correlations by group, again setting the p-level at 0.01 to account for the large number of potential correlations. For HYPO, the only significant effects were between TOMAL Abstract Visual Memory and total right (r=0.521) and right-anterior (r=0.520) hippocampal volumes. There were no significant correlations for controls. Questionnaire results were unrelated to hippocampal size in either group.
To determine the relative predictive value of the each of the hippocampal segments on memory, we conducted stepwise multiple regression analyses entering group first followed by the four segment volumes of the hippocampus together. Only one variable—WSR (the task on which groups differed)—showed an overall effect (p=0.04, R 2=0.186), reflecting a significant contribution of the left posterior segment (p=0.03, β=0.532), beyond the effect of group (p=0.04, β=0.311).
Discussion
The aims of this study were: (i) to compare hippocampal volumes and memory functions in children exposed to insufficient TH in gestation compared with typically developing controls, whose mothers presumably had normal thyroid function in pregnancy, and (ii) to determine if differences reflected severity of the mothers' gestational hypothyroidism. As hypothesized, the HYPO group had smaller left and right hippocampi, particularly in right-posterior and left-anterior segments, than controls. Maternal third-trimester hypothyroidism severity was associated with smaller right hippocampi, especially in the anterior region, as well as smaller left hippocampi but to a lesser degree. On memory tests, the HYPO group performed below controls only on the WSR subtest of the TOMAL, and on questionnaires, HYPO was rated as having significantly more daily memory problems than controls, but these indices were unrelated to maternal TH levels.
We observed that two of the four hippocampal segments—the left anterior and right posterior hippocampi, which are responsible for learning novel verbal information and for recognizing or recalling past visual information, respectively—were differentially affected by maternal hypothyroidism. It is not readily apparent, however, why these two particular subregions were more compromised in HYPO than the other subregions. One possibility is an interaction between timing of lack of hormone and timing of development of different underlying hippocampal substructures within each subregion, with the CA1 being more distributed anteriorly and the dentate gyrus more posteriorly (41). According to Gogtay et al. (26), structural development of the hippocampus is nonhomogeneous and may also reflect different patterns of maturation in the cortical regions connected to different regions of the right and left hippocampi.
We observed a significant association between smaller right hippocampal volumes (especially right-anterior hippocampus) and elevated third-trimester TSH levels or reduced fT4 levels, consistent with knowledge that hippocampal asymmetry is evident in preterm neonates (42). Our findings suggest that the right hippocampus may be critically dependent on a normal supply of TH in late gestation (which is obviously unavailable after preterm birth). Although our results are largely influenced by the child whose mother had the highest TSH levels in the second and third trimesters, our findings remain at an attenuated level when his data are removed from the analyses. Also, as this child's mother lacked third-trimester fT4 data, their data cannot explain the positive relation between third-trimester fT4 and hippocampal size. Importantly, as Figure 2 shows that mothers in better TH control during the third trimester had children with larger hippocampi, our findings support the need to monitor and manage women with hypothyroidism closely throughout their entire pregnancy until the fetal thyroid system achieves maturity at birth.
Memory test results show that the HYPO group and controls performed similarly on most indices. The one exception was on the TOMAL WSR subtest, which required learning a list of words to perfection by repeating only missing items on each trial. Nonetheless, the HYPO group scored above the test's normative mean, suggesting a relative weakness not impairment. While some evidence suggests that performance on this task is sensitive to hippocampal function (43), results are inconsistent (44) and also reflect reliance on other brain regions, such as the entorhinal cortex (45). Our observation of a relationship between elevated second- and third-trimester maternal TSH levels and performance on other indices such as memory for faces may reflect a need for maternal TH in other brain regions than the hippocampus. Our recent findings using cortical morphometry techniques to show a variety of abnormally thick or thin cortical regions in the HYPO group (46) also support this claim.
The lack of difference on the remaining clinical memory tests may reflect participants' reliance on other intact parts of the brain's memory networks as compensation or on later developing hippocampal substructures (e.g., dentate gyrus for associative memory). To address this issue, future studies need to use laboratory-based memory tasks that more finely measure specific hippocampally related memory functions and more sensitively assess the parts of the hippocampus known to be developing when the TH deficiency was occurring. Our recent study of autobiographical memory, a well-established hippocampal function task, showed it was compromised in the HYPO group (47). It is also possible that volumes are not the best indicator of memory function, and indices of functional activation, connectivity, and synaptic function may better reflect the impact of insufficient TH during pregnancy on hippocampal development. Studies examining the interconnectivity between hippocampal and nearby, as well as remote extrahippocampal regions, are thus warranted.
Findings from parent-report questionnaires showed that the HYPO group experienced more daily difficulty in everyday activities requiring memory than did controls. Particularly affected were monitoring conversations and remembering to do something. Importantly, a supplementary item analysis revealed that the HYPO group was much more likely than controls to ramble in discussions, suffer from “tip of the tongue” problems, forget what he or she just said or was doing, seem confused, and forget to do things or convey messages. Contrary to expectation, however, these difficulties were neither associated with hippocampal size nor severity of maternal hypothyroidism. While it is possible that our sample size was too small to observe the expected effects, it is also possible that these results reflected reporting bias from mothers' concerns about the impact of their early hypothyroidism, which may have been heightened by their continuous participation in our research since the child was an infant.
Finally, we found that the HYPO group showed a reduced IQ. Although this was not significantly different from controls, the difference is of similar magnitude as in other studies (4) and consistent with our earlier report on the larger cohort at a younger age (48).
Major strengths of our study are its prospective approach following both HYPO and control groups from birth, a broad battery of memory tests, and manually tracing the hippocampus rather than an automated approach, as is common. However, our study has some limitations. First, our sample size was small (common in clinical neuroimaging studies), and as we lost more than 60% of our sample over the 10–12-year period, we may have been unable to detect the subtle impact of maternal hypothyroidism on structure and memory function. Second, our mothers with hypothyroidism represented a relatively heterogeneous sample that varied considerably in their TH levels, while a few woman were missing TH values. Also, since the trimester-specific value was the mean per trimester, effects of very deviant values may have been lost if the mother had a number of varying blood draws during a particular trimester. Third, our decision not to include children born to women with normal thyroid tests in the between-group comparisons was arbitrary and based on the fact that even though their mothers were being treated for hypothyroidism during pregnancy, they were not technically “hypothyroid.” However, we chose to include them in the correlational analyses to have a larger sample and a broader range of effects. Nevertheless, it should be noted that when we repeated the correlational analyses without the children of these women, effects persisted with only slight attenuation of the p-value. Fourth, we were unable to obtain TH data from the mothers of control participants, and thus there remains the possibility these women were not completely euthyroid during pregnancy. While this is an unlikely possibility given that many of these women were repeatedly interviewed throughout the course of our study about whether they acquired hypothyroidism, the possibility of subclinical hypothyroidism in pregnancy remains and may have played a role in why we did not detect more significant differences between the HYPO and control groups. Fifth, although we used reputable clinical tests to assess memory, the ones we chose may have been influenced by brain function beyond the hippocampus. Because of the breadth of our memory battery in this exploratory study, the number of tests given to a relatively small number of subjects was large, and some of the findings (particularly in correlation analyses) may have occurred by chance. Finally, we recently learned that one control male was diagnosed with a reading problem after current participation. Although findings remained essentially the same when we reanalyzed without his data, it is possible that other control children could also have acquired latent cognitive problems that would affect the findings.
In conclusion, this study has shown that maternal hypothyroidism during pregnancy can adversely affect hippocampal development and selective memory functions, particularly list learning and everyday memory. Since the effects on memory and the hippocampus were stronger when maternal hypothyroidism was more severe throughout the entire pregnancy, our findings speak to the need for close adherence to current guidelines for managing maternal hypothyroidism during pregnancy (49,50).
Footnotes
Acknowledgments
We wish to thank Anishka Leis, Victoria Martin, and Rosie Bell for recruiting participants and assistance with conducting the study; Jovanka Skocic for assistance in performing the tracings and reliability studies; Susan Blaser for neuroradiological evaluations; and Tammy Rayner, Garry Detzler, and Ruth Weiss for scanning. We also acknowledge Wendy Wolfman for testing and recruiting “normal controls” through her obstetrics practice; Catherine Kelly and Denice Feig for recruiting hypothyroid women; Elizabeth Astzalos for recruiting controls-through her level 1 neonatal nursery; and Gideon Koren for giving us access to the Motherisk database. We appreciate John Lazarus's insightful commentary on an earlier version of this paper. (All of the mentioned individuals are located in Toronto, Canada.) Finally, we want to thank the children and their parents for their continued participation and involvement in this research.
This research was supported by a grant from the Canadian Institutes of Health Research (MOP 49488) to J.F.R. and M.P.M.; K.A.W. was supported through an Ontario Graduate Scholarship and a Hospital for Sick Children RESTRACOMP scholarship.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.