
Abstract
Background:
Central compartment lymph node metastases in papillary thyroid carcinoma (PTC) are difficult to detect preoperatively, and the role of routine or prophylactic central compartment lymph node dissection (CLND) in managing PTC remains controversial. The aim of this project was to create a nomogram able to predict the occurrence of central compartment lymph node metastasis using readily available preoperative clinical characteristics.
Methods:
Records from patients undergoing total thyroidectomy and lymph node dissection for PTC in the period 1968–2012 were analyzed. Nodal status was based on results of serial hematoxylin and eosin (H&E) examination. Age, sex, tumor size, tumor site, and multifocality were included in a multivariable logistic regression model to predict lymph node metastasis. A coefficient-based nomogram was developed and validated using an external patient cohort.
Results:
The study population included 914 patients (80% females) with an average central compartment nodal yield of eight per patient. Central compartment lymph node metastases were present in 390 patients (42.7%). The variables with the strongest predictive value were age (p<0.001), male sex (p<0.001), increasing tumor size (p<0.001), and tumor multifocality (p<0.05). The nomogram had good discrimination with a concordance index of 76.4% [95% confidence interval 73.3–79.4], supported by an external validation point estimate of 61.5% [95% confidence interval 49.5–73.6]. An online calculator and smartphone application were developed for point of care use.
Conclusions:
A validated nomogram utilizing readily available preoperative variables has been developed to give a predicted probability of central lymph node metastases in patients presenting with PTC. This nomogram may help guide surgical decision making in PTC.
Introduction
P
Total thyroidectomy is generally considered the gold-standard surgical treatment of the primary tumor in clinically significant PTC (2 –4). When cervical lymph node metastases are detected (cN1), by either clinical or radiological means, the decision to perform concurrent lymphadenectomy is well founded. Ongoing controversy exists regarding the optimal management of clinically and sonographically uninvolved (cN0) central (level VI) lymph nodes. Minimization of the morbidity of local recurrence and reoperation (5) is weighed against the potential for increased harm and perceived lack of benefit.
In institutions where prophylactic central compartment lymph node dissection (CLND) is not performed routinely, the decision to perform lymphadenectomy is dependent on clinical and radiological assessment. Due to the poor reliability of these modalities in assessing the level VI lymph nodes, a tool that helps to quantify the risk of nodal disease may facilitate preoperative decision making and help inform the discussion between the surgeon and patient.
The purpose of this study was to create a validated nomogram tool able to quantify the likelihood of central compartment lymph node metastases in patients with PTC based on preoperatively determinable clinical and radiological findings. An online interface and smartphone application were then created to aid point of care decision making.
Materials and Methods
Data were obtained from a retrospective analysis of a prospectively maintained thyroid cancer database kept within a tertiary thyroid cancer service. All patients consented to the anonymous use of their data for research prior to surgery. Approval for data collection and storage was provided by the Northern Health Human Research Ethics Committee.
Study patients
Patients undergoing first-time surgery for PTC within the University of Sydney Endocrine Surgical Unit in the period 1968–2012 were studied. A total of 1589 patients with histologically proven PTC were identified.
Patients were excluded who had no lymph nodes removed (n=597), who had lateral but not central lymph nodes removed (n=70), and who had inadequate covariate information (n=8). The population used in the analyses consisted of 914 patients who all underwent thyroidectomy and CLND. Tumors found incidentally in patients undergoing thyroidectomy were included only if nodal dissection was also performed. Papillary microcarcinomas may metastasize in 20–60% of cases (6,7) and were included in the analysis.
CLND and pathological evaluation
CLND was performed as previously described (8). The typical approach was to perform ipsilateral CLND. However, bilateral CLND was also performed in 16% of cases. All operations were performed by surgeons within the University of Sydney Endocrine Surgery Unit.
In the study population of 914 patients, 744 (81%) had CLND performed routinely in the period after 2003. The remainder had CLND performed selectively at the discretion of the surgeon. To investigate further the applicability of the series to CLND, sensitivity testing was performed on patients undergoing surgery after 2003 (n=744), when the practice of prophylactic or routine CLND was introduced at this unit, and on patients who underwent CLND without any form of lateral lymphadenectomy (n=566).
The key outcome measure was the presence of PTC lymph node metastases as determined on histopathological examination. Lymph nodes were evaluated by step-sectioning with hematoxylin and eosin (H&E) staining. Pathology reporting was undertaken by three dedicated endocrine pathologists.
Predictive variables considered both likely to influence the rate of central compartment metastases and available in the preoperative period included clinical factors (age and sex) and tumor features (size, site within the thyroid, and multifocality).
Statistical methods
Descriptive statistics for the sample were calculated to show the number of patients for each predictive factor: (i) age, grouped as less than or greater than 45 years; (ii) sex; (iii) tumor size, grouped according to TNM criteria (9); (iv) tumor site, grouped as superior, mid, inferior, isthmic, or other; and (v) tumor multifocality, grouped as absent or present. The positive outcome variable was the number of patients (and percent) who had one or more positive nodes.
For the predictive model, we restricted one patient's tumor size of 100 mm to 70 mm to ensure that this value did not have undue influence as an outlier.
Logistic regression was used to model the association between each variable and the presence of PTC lymph node metastases. All candidate variables (age, sex, site of primary tumor, tumor multifocality) were included in the multivariable model regardless of significance to ensure the model's generalizability. Sex, tumor site (inferior, mid, superior, isthmus, and other/no data), and tumor multifocality (absent or present) were included in the models as categorical variables. Preliminary analysis showed that the best functional form for age was through a quadratic function. Tumor size was modeled using a fractional polynomial, and the best-fitting fractional polynomial was obtained from the full multivariable model. In multifocal cases, the largest diameter of the largest tumor focus was used to determine tumor size. Likelihood ratio p-values were used to assess the incremental value of each variable, and p<0.05 was considered statistically significant. For each patient, we calculated their probability of PTC lymph node metastases. The ability of the model to discriminate between patients with and without lymph node metastases was assessed using the area under the ROC curve (AUC), also known as the concordance index.
Ten thousand random bootstrap resamples were used for internal validation of the model and to assess the degree of sampling error in the estimates. This method, used to assess internal validation for risk prediction models, involves creating multiple (in this case 10,000) new samples from the existing data, and using the variability in the model estimates to ascertain sampling variability. Confidence intervals were estimated from the percentiles of the bootstrap distributions.
Sensitivity analyses were performed to assess the impact of the surgical unit's change in practice from 2003 onwards (routine prophylactic CLND for cN0 patients) and of lateral lymph node dissection on the model. This was done by refitting the model on the subset of patients from 2003 onwards and separately on the subset of patients with no lateral lymph node dissection (CLND alone).
External validation was performed using 87 patients who underwent thyroidectomy and CLND for PTC at the University of California Los Angeles Endocrine Surgery Unit between September 2000 and December 2010. As this data set did not document tumor site, two versions of the model were assessed. First, we used the original model and categorized all tumor sites as “unknown,” and second, a new model was fitted to the original sample with the tumor site variable excluded. The performances of these models were assessed on the external sample. The discrimination of the model in the external validation sample was assessed using the AUC. The calibration of the model was assessed by modeling the predicted probabilities from the model versus the true outcomes using logistic regression. Boxplots of the predicted probabilities in the original and external validation samples were plotted according to the presence or absence of PTC lymph node metastases (Fig. 1).
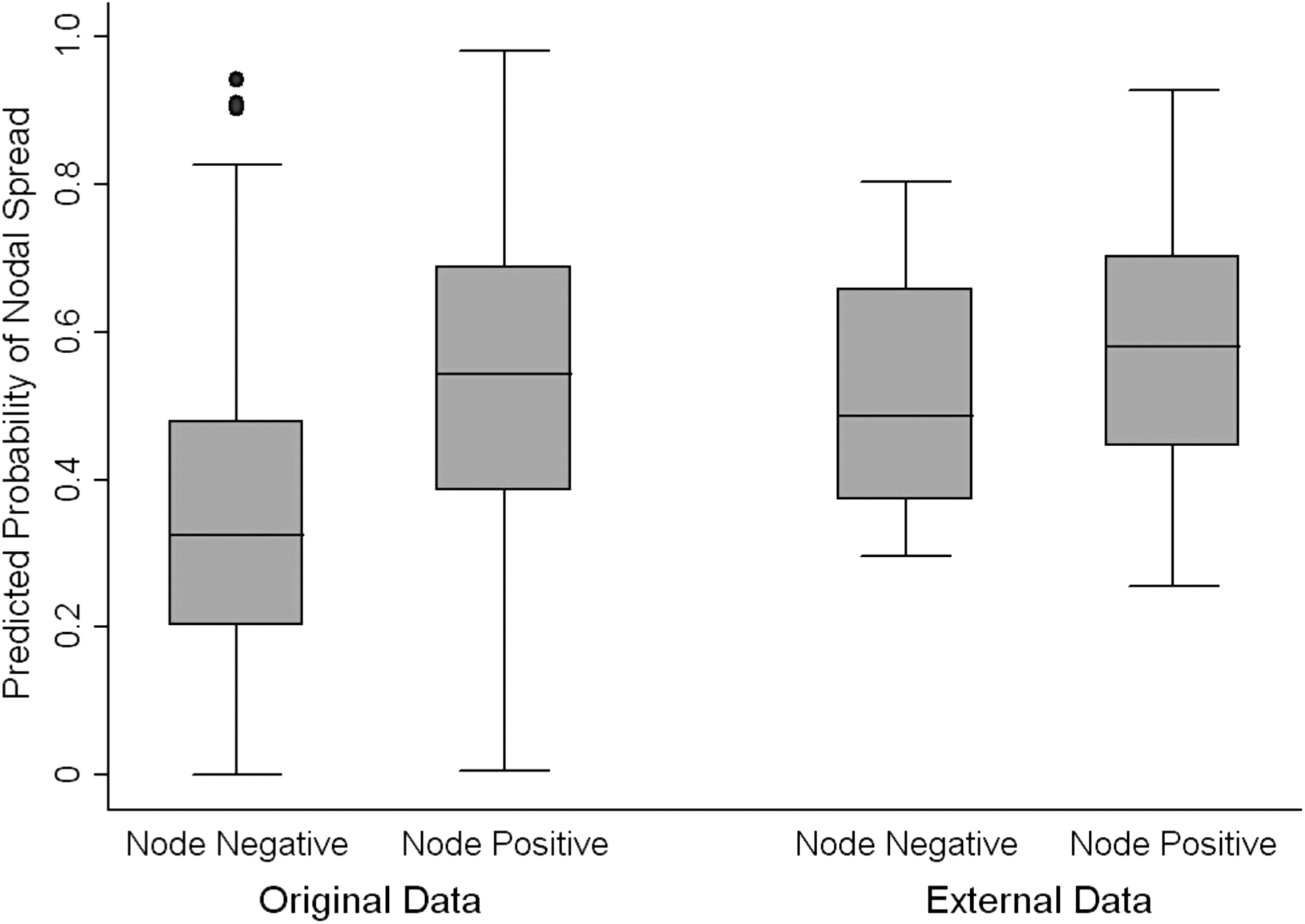
Distribution of predicted probabilities by pathologically determined nodal involvement for the original and external data sets.
All statistical analyses were performed in SAS v9.2 and Stata v11.2.
Software development
An online interface (Supplementary Fig. S1; Supplementary Data are available online at
Results
Demographics
The study population consisted of 733 females and 181 males with a mean age of 46.3 years. The overall rate of nodal metastases detected by H&E sectioning was 42.7% (Table 1). The mean nodal yield from the central compartment was 7.7 lymph nodes. Lateral compartment lymph nodes were removed in 348 (38.1%) patients and were positive in 173 patients (Table 1). Skip metastases occurred in 5.6% of patients who had cancer in the lymph nodes (23 of 413) and were considered “node negative” for the purposes of the central compartment predictive model.
23 patients with skip metastases are not included.
The mean maximum diameter of the primary tumor was 17.4 mm (median=15.0 mm), with sizes ranging from 0.2 mm to 100 mm. A total of 36.2% of the study population had papillary microcarcinomas (T1a).
The rates of lymph node metastases according to each of the predictive variables are shown in Table 2. The database did not contain sufficient detail to define the size of the metastatic deposits within the lymph nodes and therefore included both micro- and macrometastases.
T1a (≤10 mm), T1b (>10 mm and ≤20 mm), T2 (>20 mm and ≤40 mm), ≥T3 (>40 mm) (9).
Categorization of extrathyroidal spread: 1, Tumor is completely confined to the thyroid parenchyma; 2, tumor directly underlies the junction of the thyroid and adjacent soft tissue; 3, tumor extends focally out of the thyroid and adjacent perithyroidal fibroadipose tissue; 4, widespread extrathyroidal spread into soft tissue and skeletal muscle; 5, unknown.
Our database recorded tumor focality according to the number of tumor foci seen (1, 2, 3, ≥4). When modeled in this way, multifocality was also a significant risk factor (p<0.001) and improved the concordance index to 77.2%. As preoperative ultrasound is not sensitive to this level of measurement, multifocality was remodeled to be either “present” (number of foci=2, 3, or ≥4) or “absent” (number of foci=1). Significance was preserved under the less detailed classification system in both the univariable (p=0.017) and multivariable (p<0.05) models.
Of the study population, 63.2% had insufficient detailing of tumor site, in most cases having it defined as “left lobe” or “right lobe” only.
Prediction model for lymph node metastases
In the multivariable model, patient age, sex, tumor size, and multifocality were all associated with the presence of lymph node metastases (p<0.001; Table 3). Males had 2.27 times increased odds of lymph node metastases compared to females [95% confidence interval (CI) 1.56–3.23] adjusted for all other variables in the model (Table 3). The risk related to age was U-shaped with increased odds of metastases in younger and older patients (Fig. 2B). Increasing tumor size was also highly predictive of lymph node metastases, with tumors >50 mm having an estimated 60% predicted probability of involved lymph nodes (Fig. 2A).

Predicted probability of central lymph node disease compared to
Reference group for Wald p-values.
Intercept=−0.057
AUC, area under the receiver operator curve, also known as the Concordance Index; CI, 95% confidence interval.
This model showed good discrimination of lymph node metastases with an AUC of 76.4% [CI 73.3–79.4]. Internal validation, performed on 10,000 bootstrap resamples, produced an AUC of 76.4% [CI 73.6–79.7]. The bootstrap confidence intervals for the odds ratios were similar but slightly wider, as expected, than the original model.
Sensitivity analysis
Although the database was unable to discern if CND was performed with prophylactic or therapeutic intention, it was known that the prophylactic approach became routine at the start of 2003. A sensitivity analysis of the 744 patients operated on since 2003 had similar precision (AUC=76.5%) compared to the full data set, with model coefficients similar to that obtained in the full model (Supplementary Table S1).
External validation
The external validation population comprised 87 patients (72 females) with a 64% overall rate of nodal metastases. The mean age was 40.1 years with a range of 13–75 years. Tumor and lymph node characteristics were again determined by histopathology and were comparable overall to the original data set (Table 1). The site of primary tumor was not recorded in this data set.
When applied to the original model, the external validation data set (assuming tumor site unknown for the 87 cases) produced an AUC of 61.5% [CI 49.5–73.6]. Tumor site was then excluded from both data sets (Fig. 3; “original reduced model” and “external reduced model”) and the model refitted on the original sample. A comparison of ROC was produced (Fig. 3).

Receiver operator curves for original and external validation data sets, and reduced models (excluding site of primary tumor).
Figure 1 shows the distribution of predicted probabilities of nodal metastases for the original sample and external validation sample by whether lymph node metastases were present at histopathological examination.
To check the calibration of the model, the predicted probabilities from the model were used as predictor variables against the true outcomes. A calibration slope of 1 would indicate perfect calibration, and a slope less than 1 indicates the degree of shrinkage required for the model coefficients to be optimized to the new sample. We found that the calibration slope did not deviate significantly from 1 (full model: deviations from perfect calibration=0.38, p=0.254; reduced model: deviations from perfect calibration=0.38, p=0.23), indicating that there was little shrinkage of the model coefficients. The mean of the predicted values was similar to the mean of the true values (full model: difference=−0.02, p=0.94; reduced model: difference=−0.01, p=0.96).
Discussion
In the absence of randomized controlled data, the role of central lymph node dissection in PTC continues to be debated. Prophylactic level VI lymphadenectomy, which in the cN0 patient has become increasingly popular, is supported by evidence that suggests reduced local recurrence rates (2,10 –12) and less potentially hazardous reoperative surgery. Advocates also point to an improved postoperative course as defined by a lower serum thyroglobulin (13) and potentially lower doses of radioactive iodine-131 (14,15). Survival benefit, although identified in several studies (16 –18), has been difficult to prove, possibly because of the excellent overall prognosis seen in patients with PTC (19).
An alternate approach that many clinicians continue to adopt is a policy of therapeutic lymphadenectomy only. They cite a lack of evidence for the benefit of prophylactic CLND in terms of recurrence and survival (20), as well as the potential increased risks to the patient (21,22). Although many series have shown little or no adverse effect from CLND (23), there is concern that in low-volume centers, rates of permanent hypoparathyroidism and recurrent laryngeal nerve injury might increase if the procedure became the acceptable standard of care.
While upstaging of patients due to the detection of subclinical disease may change treatment (24), the impact of cN1a disease on the decision to use radioactive iodine is most often institutionally dependent (25) and variable.
Therapeutic rather than prophylactic management of the central compartment depends on detection of nodal metastases by clinical and radiological means. In contrast to the lateral neck, ultrasound, computed tomography (CT), and physical examination perform poorly in diagnosing nodal disease in level VI (26,27) due to the anatomical confines.
Given the limited ability to detect level VI nodal metastases clinically, attention might instead be turned to risk stratification, in order to select patients most likely to have locoregional nodal disease. The aim of this study was to develop a nomogram tool able to predict the risk of central compartment lymph node metastases, and thereby guide clinicians in regard to the need for prophylactic lymphadenectomy.
Our study identified central compartment nodal metastases in 42.9% of cases. Of the patients who had concurrent lateral nodes dissected, a 49.7% rate of lateral nodal metastases reflects our practice of therapeutic (rather than prophylactic) lateral neck dissection. The median number of lateral nodes (four per patient) is in keeping with selective node sampling of the medial aspects of levels III and IV in certain patients. Among patients with lymph node metastases, the rate of skip metastases (5.6%) was comparable to work by Roh et al. (28), but lower than that of Machens et al. (29).
Excluding patients who underwent lateral lymphadenectomy from our model had little or no impact on the significance of patient age (p<0.001), sex (p=0.007), and tumor size (p<0.001), and only a modest effect on the overall model fit (AUC=74.6%; Supplementary Table S1). Multifocality (p=0.84) and tumor site (p=0.75) were not significant factors in this sample.
This large retrospective cohort of patients who underwent thyroidectomy and nodal dissection for PTC has enabled clinical and tumor characteristics to be tested as predictive factors for nodal metastases. Macroscopic (>2 mm) and microscopic metastases were not differentiated in our histopathological appraisal. In the younger population, micrometastases may be clinically significant in >50% of cases (30). The impact of micrometastases is, however, controversial, and a number of authors question their role in locoregional recurrence (31,32). Ongoing work in our unit aims to explore the prognostic value of macro- and micrometastases.
Male sex was highly predictive of nodal spread in both the univariable and multivariable models. This has been previously demonstrated in series by Mirallie et al. (33) and Hay et al. (34).
In order to function as a preoperative tool, the nomogram relies on a close correlation between histopathologically determined tumor characteristics and radiological findings. Shimamoto et al. (35) looked at the ultrasound findings of 77 thyroid malignancies and found ultrasound to estimate tumor size accurately (T stage) in 63 (81.8%) cases. Thirteen of 35 T4 tumors were understaged, and one T2 tumor was overstaged, suggesting that while ultrasound is very accurate in assessing the size of the malignant nodule, it is less reliable in detecting extrathyroidal spread.
Park et al. (36) performed preoperative ultrasound on 94 consecutive patients with PTC and found sonographic estimation of greatest tumor diameter compares favorably with that determined on histopathology, with accurate estimation (findings within 20%) present in 78 (83%) of 94 patients. Overestimation (14 of 94 cases, 14.9%) was much more likely than underestimation (2 of 94 cases, 2.1%).
Larger tumors have frequently been shown to be associated with higher rates of nodal spread and worse disease-free survival (37,38). The relationship between tumor size and predicted probability of nodal disease (Fig. 2A) shows that 20% variability in tumor size would produce only very modest (<5%) changes in risk calculation, even for large tumors.
Previous investigations have suggested that the lymphatic drainage of the inferior parts of the thyroid is directed toward the central compartment and that the superior poles drain primarily toward the upper, central compartment and lateral nodes (39).
In the 336 patients on whom the site of primary tumor had been determined, no significant association was detected. Similar findings were reported by Lee et al. (40). This may be because normal lymphatic channels are obstructed where malignancy is present. Despite its lack of significant association, the site variable was kept in the model to avoid overfitting.
Multifocal tumors are associated with higher rates of lymph node involvement (1). Total thyroidectomy is generally the accepted standard to manage primary PTC, and many clinicians would not go to lengths to determine if a bilateral or multifocal cancer is present, since the whole thyroid is to be removed. Preoperative assessment for aggressive tumor features may therefore be underutilized in many centers.
Ultrasonographic detection of tumor multifocality in the preoperative period is highly operator dependent. Park et al. (36) successfully identified multifocality in 22 of 29 (75.9%) cases, and bilateral cancers in 15 of 18 (83.3%) cases. Other studies have shown ultrasound to have a sensitivity around 60% and a positive predictive value of 44–68%. While ultrasound is therefore not reliable, positive findings such as multiple suspicious nodules or diffuse punctate calcifications may aid in diagnosing a multifocal tumor. Recategorization of tumor focality from the histopathological detail (1, 2, 3, ≥4 foci of tumor) of our database to a level of accuracy more in keeping with ultrasound did not reduce the significance (p=0.045) in our multivariable model.
Limitations of this series in relation to histopathological and ultrasonographic discrepancies are best dealt with by further prospective external validation studies. Although this study's inability to isolate prophylactic and therapeutic procedures may have resulted in higher rates of metastases, it also resulted in a good sample size and proportion of positive endpoints. The predictive accuracy of the model was only slightly higher when based on the patients operated on from 2003 onwards (AUC=76.5).
Other variables (extrathyroidal spread, and lymphovascular invasion) previously demonstrated to increase risk of nodal disease were not assessable preoperatively. In this data series, extrathyroidal spread was highly predictive of nodal disease in preliminary univariable and multivariable models, and increased the concordance index to 82%. Future predictive modeling may incorporate microRNA (41) and PTC subtypes (42), as well as immunohistochemical staining patterns of fine-needle aspiration samples.
The development of an online interface and smartphone software has been previously used for predictive models. Bevilacqua et al. (43) produced a validated nomogram predicting sentinel node metastases in patients with breast cancer and highlighted the patient's focus on pursuing information about their disease and tailoring surgery to the individual. As in other fields, personalization of surgery is of growing importance in the management of PTC (44).
This nomogram does not aim to provide a “tipping point” where risk and benefit meet. This would require reliable studies on the quality of life with and without CLND, which at present do not exist. The overall rate of nodal metastases in this study approached 50% and certainly supports the practice of prophylactic level VI lymphadenectomy by those clinicians who feel that PTC nodal metastases are clinically significant. Where the routine prophylactic approach is not adopted, our nomogram aims to stratify risk to allow for more informed preoperative discussion with patients. A second utility may be to select high risk patients for bilateral central neck dissection (45).
Conclusion
This study puts forward a predictive model that appears to determine reliably the likelihood of central compartment lymph node metastases in PTC. The model allows the use of readily available preoperative clinical characteristics in a point of care setting that may help guide surgical decision making in the management of PTC.
Footnotes
Acknowledgments
A.M.T. completed the Mary-Jo Reeve Fellowship with the Department of Endocrine Surgery, University of Sydney. R.M.T. was supported by National Health and Medical Research Council (NHMRC) program grant 633003 to the Screening and Test Evaluation Program.
Author Disclosure Statement
The authors declare that no competing financial interests exist or have contributed to the production of this manuscript.