
Abstract
Background:
The expression of somatostatin receptors (SSTR) in thyroid cells may offer the possibility to identify metastatic lesions and to select patients for peptide receptor radionuclide therapy (PRRT). We investigated 68Ga-DOTATOC positron emission tomography/computed tomography (PET/CT) to select patients with progressive differentiated thyroid cancer (DTC) for PRRT as well as treatment response and toxicity in treated patients.
Methods:
We enrolled 41 patients with progressive radioiodine-negative DTC (24 women and 17 men; mean age=54.3 years, median=59 years, range=19–78 years). In all patients, [18F]FDG-PET/CT was performed to determine recurrent disease with enhanced glucose metabolism, and 68Ga-DOTATOC PET/CT was used to identify SSTR expression. Dosimetric evaluation was performed with 111In-DOTATOC scintigraphy. Eleven patients were treated with PRRT receiving a fractionated injection of 1.5–3.7 GBq 90Y-DOTATOC/administration. Serial 68Ga-DOTATOC PET/CT scans were performed in all treated patients to evaluate treatment response. Parameters provided by 68Ga-DOTATOC PET/CT were analyzed as potential therapeutic predictors to differentiate responding from nonresponding. In all treated patients, adverse events and toxicity were recorded.
Results:
68Ga-DOTATOC PET/CT were positive in 24/41 of radioiodine-negative DTC patients. Based on the high expression of SSTR detected by 68Ga-DOTATOC PET/CT, 13 patients were suitable for PRRT. Two out of 13 patients were not treated due to the lack of fulfillment of other study inclusion criteria. PRRT induced disease control in 7/11 patients (two partial response and five stabilization) with a duration of response of 3.5–11.5 months. Objective response was associated with symptoms relief. Functional volume (FV) over time obtained by PET/CT was the only parameter demonstrating a significant difference between lesions responding and nonresponding to PRRT (p=0.001). Main PRRT adverse events were nausea, asthenia, and transient hematologic toxicity. One patient experienced permanent renal toxicity.
Conclusions:
In our series, SSTR imaging provided positive results in more than half of the cases with radioiodine-negative DTC, and about one third of patients were eligible for PRRT. 68Ga-DOTATOC PET/CT seems a reliable tool both for patient selection and evaluation of treatment response. In our experience, FV determination over time seems to represent a reliable parameter to determine tumor response to PRRT, although further investigations are needed to better define its role.
Introduction
T
In recent decades, the re-induction of 131I transport, organification, and retention by thyroid cancer cells have been attempted with controversial results (3 –8). More recently, several biological agents (e.g., inhibitors of RET and MEK) have been evaluated in clinical trials in iodine-refractory patients with progressive disease (9 –12).
Previous studies have described the visualization of metastases from follicular cell-derived thyroid cancer by somatostatin receptor (SSTR) scintigraphy (13), in agreement with the in vitro demonstration of specific SSTR in thyroid cells (14 –16). Based on these premises, peptide receptor radionuclide therapy (PRRT) with radiolabeled somatostatin analogues, originally introduced for neuroendocrine tumors (NETs) (17), has also been proposed as a therapeutic tool in patients with advanced thyroid cancer (18 –21). A preliminary experience with [90Y]-DOTA0-Tyr3-octreotide (90Y-DOTATOC) PPRT in patients with iodine-refractory thyroid cancer has provided encouraging results (22,23).
We present our experience with 90Y-DOTATOC PRRT in a series of patients with progressive radioiodine-negative differentiated thyroid cancer (DTC), selected on the basis of 68Ga-DOTATOC positron emission tomography/computed tomography (PET/CT) imaging.
Materials and Methods
Study design
This was a prospective nonrandomized single-arm clinical trial performed at the Nuclear Medicine Unit of Arcispedale Santa Maria Nuova—IRCCS, Reggio Emilia, Italy. The study was conducted in accordance with the International Conference on Harmonization Good Clinical Practice guidelines, the Declaration of Helsinki, and it was approved by Local and National Authorities (EudraCT numbers 2006-000897-65 and 2008-000983-17). All patients gave written informed consent.
Patients
We enrolled 41 consecutive patients (24 women and 17 men; mean age=54.3 years, median age=59 years, range=19–78 years) with progressive radioiodine-negative DTC. Radioiodine-negative progressive DTC was determined according to the American Thyroid Association guidelines (24) as follows: (i) negative 131I whole-body scan; (ii) thyroglobulin (TG) level either >0.5 ng/mL (n=36) or <0.5 ng/mL in the presence of positive anti-TG antibodies (n=5) during thyrotropin (TSH) stimulation; and (iii) positive cervical ultrasonography (n=12), contrast-enhanced CT (n=28) and 2-deoxy-2-F(18)-fluoro-D-glucose ([18F]FDG) PET/CT (n=34). Sites of recurrent disease are specified in Tables 1 and 2. Thyroid cancer histology was as follows: papillary thyroid carcinoma (PTC; n=31; tall cells variant n=4); follicular thyroid carcinoma (FTC; n=4); insular thyroid carcinoma (n=4); and Hürthle cell carcinoma (HTC; n=2). All patients had previously received between one and five cycles of 131I (3.7–41 GBq).
PS, performance status; ECOG, Eastern Cooperative Oncology Group; N,M, Node and Metastases classifications according to AJCC/UICC TNM 7th edition (64); PD, progressive disease; TG, thyroglobulin; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; TT, total thyroidectomy; LND, lateral neck lymph node dissection; CND, central neck lymph-node dissection; LNs, lymph nodes; US, ultrasonography; CT, computed tomography; [18F]FDG-PET/CT=2-deoxy-2-F(18)-fluoro-D-glucose positron emission tomography combined with computed tomography.
Positive TGAb.
CNS, central nervous system; TGAb, anti-thyroglobulin antibodies.
Baseline patients' characteristics and previous treatments are detailed in Table 1 for each patient.
68Ga-DOTATOC PET/CT was performed in all patients to determine eligibility to PRRT. Patients having high expression of SSTR at 68Ga-DOTATOC PET/CT, an adequate hematological profile, and normal creatinine levels were admitted to PRRT. In all patients admitted to PRRT, a dosimetric evaluation with 111In-DOTATOC scintigraphy was also performed.
Radiopharmaceutical preparation
68Ga-DOTATOC (used for PET/CT), 111In-DOTATOC (used for dosimetry), and 90Y-DOTATOC (used for PRRT) were synthesized as previously reported (25,26). Radiochemical purity was assessed by chromatographic methods of the preparations resulted always in >95% and 99.8% for 68Ga-DOTATOC and 111In-/90Y-DOTATOC respectively.
PET/CT imaging
PET/CT scans were acquired on a GE Discovery STE™ (GE Healthcare Milwaukee, WI) 45–60 minutes after the injection of 68Ga-DOTATOC (2 MBq/kg) or [18F]FDG (4 MBq/kg). Bed positions (7 –9) with seven-slice overlap were acquired for 4–5 minutes emission time in 3D. The CT exposure factors for all examinations were 120 kVp and 80 mA in 0.8 seconds. PET images were reconstructed using a full 3D ML-OSEM algorithm. Studies were visually and semi-quantitatively assessed.
Standardized uptake value (SUV) calculations were performed on an Advantage Workstation™ (GE Healthcare). Mean and maximum SUV (corrected for patient weight and total injected activity) were recorded in all lesions.
Baseline PET/CT imaging interpretation
68Ga-DOTATOC PET/CT results were compared to [18F]FDG-PET/CT findings. The intensity of uptake in the tumor site was visually and semi-quantitatively assessed using the corresponding surrounding normal tissue as reference standard by a panel of two board-certified, nuclear-medicine physicians blinded to the patients' characteristics. Lesions were scored as 0 when no uptake was observed, 1+ when uptake was fainter than the surrounding normal tissue, 2+ in the presence of uptake similar to the surrounding normal tissue, and 3+ when showing uptake higher than the surrounding normal tissue.
Dosimetry
Dosimetric estimates were determined after the intravenous injection of 185 MBq of 111In-DOTATOC with a dual-head gamma camera (Genesys®, Philips, Amsterdam, The Netherlands, or Symbia-T®, Siemens, Munich, Germany) using parallel-hole, medium-energy, general-purpose collimators with window photon peaks centered over 247 and 172 keV (window width of 20%), as previously described by Filice et al. (25). Briefly, whole-body scans were performed at 1, 4–6, 20–24, 48, and 72 hours after radiopharmaceutical administration. Blood clearance was determined using blood samples drawn at 30 and 60 minutes, and at 4, 20, and 48 hours after radiopharmaceutical injection. Doses delivered to the tumor lesion and critical organs were obtained using OLINDA/EXM software (27). The dose to the red marrow was calculated from the residence time in blood, assuming no specific uptake, a uniform distribution of activity, and clearance from red marrow equal to that from blood. A correction factor of 1 was used, as described by Cremonesi et al. (28).
Selection of patients eligible for PRRT
Patients fulfilling the following inclusion criteria were admitted to PRRT: (i) adequate laboratory tests (hemoglobin level ≥10 g/dL; leucocytes ≥2.5×103 per mL; platelets ≥100×103 per mL; bilirubin levels <2.5 mg/dL; creatinine levels <2 mg/dL); (ii) high expression of SSTR on 68Ga-DOTATOC-PET/CT defined as a score 3+ in tumor lesions; (iii) adequate dosimetric estimates to tumor, kidney, liver, red marrow, lung and whole-body; and (iv) exclusion of pregnancy or lactation.
Peptide receptor radionuclide therapy
Repeated administrations of 1.5–3.7 GBq 90Y-DOTATOC per cycle were intravenously injected with a time interval between cycles of 6–12 weeks (17). However, in case of toxicity, treatment was delayed until recovery of the normal organ function. For each administration, patients were hospitalized in a shielded environment for 3 days in accordance with local requirements.
As recommended (17), to counteract and reduce the high kidney retention of radiopeptides, an aminoacid infusion was co-administered with PRRT and continued over 2 days following radiopeptide administration. The renal protection was performed as follows: during the first day, mixed commercially available aminoacid infusion was used (1.5 L Proteinsteril Hepa 8% containing 10.72 g
None of the patients had been treated with long- or short-acting somatostatin analogs during the previous six and three weeks before receiving PRRT respectively. Repeated administrations were withheld in case of renal toxicity, loss of patient consensus, or denial of further treatment at least three months apart, as well as in case of progressive disease. Thyroxine was administered on a daily basis and continued during PRRT treatment in order to maintain absolute thyrotropin suppression.
Patients' follow-up
Vital signs were monitored before and for 72 hours after each therapeutic radiopharmaceutical infusion. Hematologic parameters and creatinine levels were measured before each cycle and at biweekly intervals until 12 weeks after the last PRRT administration. Then, patients were followed monthly for nine months. All toxicities were recorded. Acute and long-term adverse events were graded according to the Common Terminology Criteria for Adverse Events v3.0 (30).
TG measurements were performed every six months during treatment and were repeated three months after the end of PRRT.
Serial follow-up 68Ga-DOTATOC PET/CT studies were repeated after each PRRT administration (one to two weeks before the next administration, and three months after the end of treatment). Areas of radiopharmaceutical uptake in baseline and follow-up studies were compared. The low-dose CT images co-registered with the 68Ga-DOTATOC PET imaging were used to evaluate treatment response according to the Response Evaluation Criteria in Solid Tumors (RECIST) (31). In the presence of stable disease (SD) or partial response (PR), a confirmatory scan was performed four weeks after the initial response assessment. Additional standard radiological examinations were performed when needed. Further, the PET-VCAR™ application (GE Healthcare) was used to analyze tumor response considering the functional volume (FV) and functional volume change (ΔFV%) (32). Since RECIST criteria are not appropriate to assess bone lesion responses, we used FV changes over time for such determination.
We also calculated the SUV of each lesion and derived lesion response according to European Organization for Research and Treatment of Cancer (EORTC) criteria; SUV relative to the maximal splenic uptake by dividing the SUVmax of the tumors by the SUVmax of the spleen (SUVT/S), since this parameter has been proven to be superior to ΔSUVmax in predicting time to progression; and clinical outcome (33). Additionally, we calculated SUV of each lesion relative to the maximal liver uptake (SUVT/L) and to the muscle (SUVT/M). Results with both RECIST and PET-derived parameters were compared to clinical benefit and outcome.
Treatment endpoints
Primary endpoints were treatment response and toxicity of PRRT. The overall response rate was defined as the number of participants who showed a response to treatment divided by the total number of participants.
Statistical analysis
Statistical analyses were performed using the SPSS v15 (SPSS Inc., Chicago, IL) software package.
Multiple regression analysis of all the potential predictors of 68Ga-DOTATOC PET/CT positivity and clinical response to PRRT was performed using Backward Stepwise method. The following variables were analyzed: age, sex, histopathology, disease stage at diagnosis, disease duration, time to recurrence after primary treatment, serum TG levels, 131I cycles and cumulative 131I activity previously received, number and sites of metastasis, and performance status (PS). Additionally, median SUVmax in the most 68Ga-DOTATOC avid lesions and provisional absorbed dose in the target lesions were analyzed as potential predictors of 68Ga-DOTATOC PET/CT positivity. Pearson coefficients were calculated for the correlations between the SUV values and FV determinations. Kruskal–Wallis and Spearman correlation were used to measure differences in these scores and their correlation with clinical improvement and lesion response to therapy. An uncorrected p-value of <0.05 was assumed to be statistically significant. Sensitivity analyses were performed in the subsets of responders and nonresponders to PRRT for response and toxicity.
Results
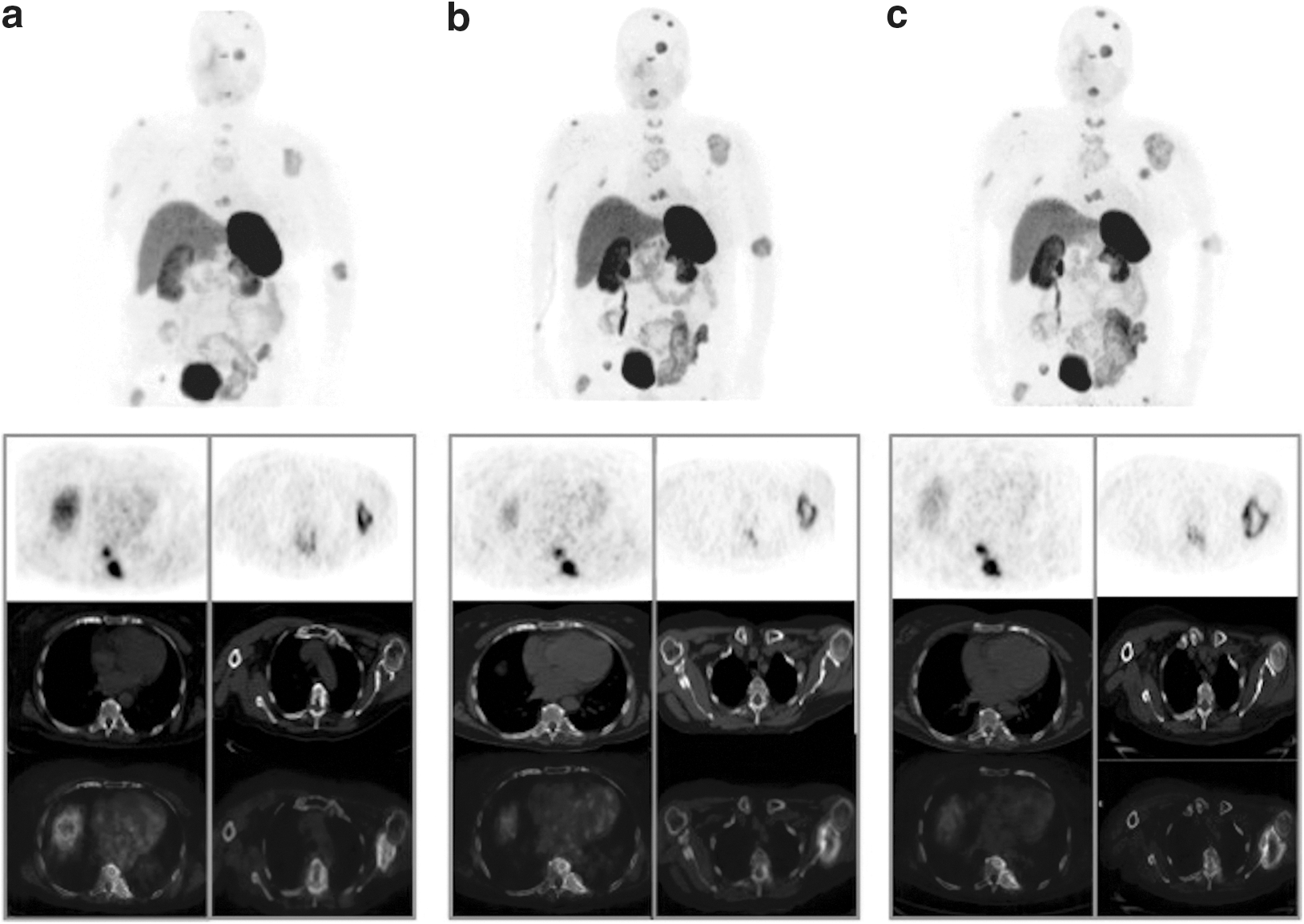
Baseline 68Ga-DOTATOC PET/CT demonstrated at least one site of radiopharmaceutical uptake in 24/41 (58.5%) patients. In 17/41 patients, 68Ga-DOTATOC PET/CT was completely negative, while [18F]FDG-PET/CT was completely negative in 7/41 cases. Only one patient presented a 68Ga-DOTATOC PET/CT positive lesion with a negative [18F]FDG-PET/CT. [18F]FDG and 68Ga-DOTATOC uptake were similar in 6/23 cases, while a predominant [18F]FDG or 68Ga-DOTATOC uptake was present in 11/23 and 7/23 patients respectively. Figure 1 shows different patterns of uptake on 68Ga-DOTATOC PET/CT and [18F]FDG-PET/CT.

Examples of different pattern of uptake of [18F]FDG (left columns) and 68Ga-DOTATOC (right columns) on positron emission tomography combined with computed tomography (PET/CT; PET emission on left panels, and fused PET/CT images on right panels). Subpleural and lymph-node lesions
At multivariate analysis, none of the variables considered was associated with 68Ga-DOTATOC PET/CT positivity. All patients with negative 68Ga-DOTATOC PET/CT imaging had a papillary histology (n=17/31). Metastatic sites of disease (i.e., lymph nodes, lungs, bones) were apparently not related to either a [18F]FDG or 68Ga-DOTATOC preferential uptake. Thirteen patients presented a score of 3+ in tumor lesions on 68Ga-DOTATOC PET/CT and hence were suitable for PRRT. However, due to the lack of fulfillment of the other inclusion criteria, only 11 patients were treated with PRRT. Sites of disease for each treated patient are specified in Table 3.
DOTATOC, DOTA0-Tyr3-octreotide; PRRT, peptide receptor radionuclide therapy; RECIST, Response Evaluation Criteria in Solid Tumors.
Patient specific dosimetry allowed the provision of organ-specific radiation absorbed doses and the estimation of the risk of delayed organ toxicity (Table 4).
A total of 44 administrations of 90Y-DOTATOC (2–6 administrations/patient) at 70±24.6 days apart (range=45–140 days) were injected with a median cumulative activity of 3.5 GBq (range=1.5–3.7 GBq).
A total of 28 68Ga-DOTATOC PET/CT scans were performed in patients undergoing PRRT. Baseline and end-of-study scans were used to evaluate treatment response (Figs. 2 and 3). The overall response assessed by 68Ga-DOTATOC PET/CT resulted in PR in 2/11 patients (lasting up to eight months), SD in 5/11 (with a duration up to 11.5 months), while progressive disease (PD) was observed in four cases (Table 3). In all four patients defined as PD, the PD was assessed by 68Ga-DOTATOC PET/CT performed three months after the end of treatment. Based on the tumor site, a total of 79 lesions were evaluable for the assessment of PRRT responses. Lesions were localized in the thyroid bed (n=4), lymph nodes (n=19), lungs (n=18), and bones (n=38). Table 5 summarizes overall responses and tumor-site responses in all treated patients. TG values did not show significant differences between baseline and follow-up measurements over time. TG was not significantly correlated with objective responses to PRRT or the calculated 68Ga-DOTATOC PET/CT parameters (SUVmax, SUVT/S, and FV). SUVmax and FV did not demonstrate any significant difference based on tumor site. Among all the 68Ga-DOTATOC PET/CT parameters considered, FV was the only one that demonstrated a significant difference between responding (either PR or SD) and nonresponding lesions to PRRT (p=0.001; Fig. 4).

68Ga-DOTATOC PET/CT in a metastatic Hürthle cell carcinoma at baseline
68Ga-DOTATOC PET/CT in a metastatic insular TC at baseline
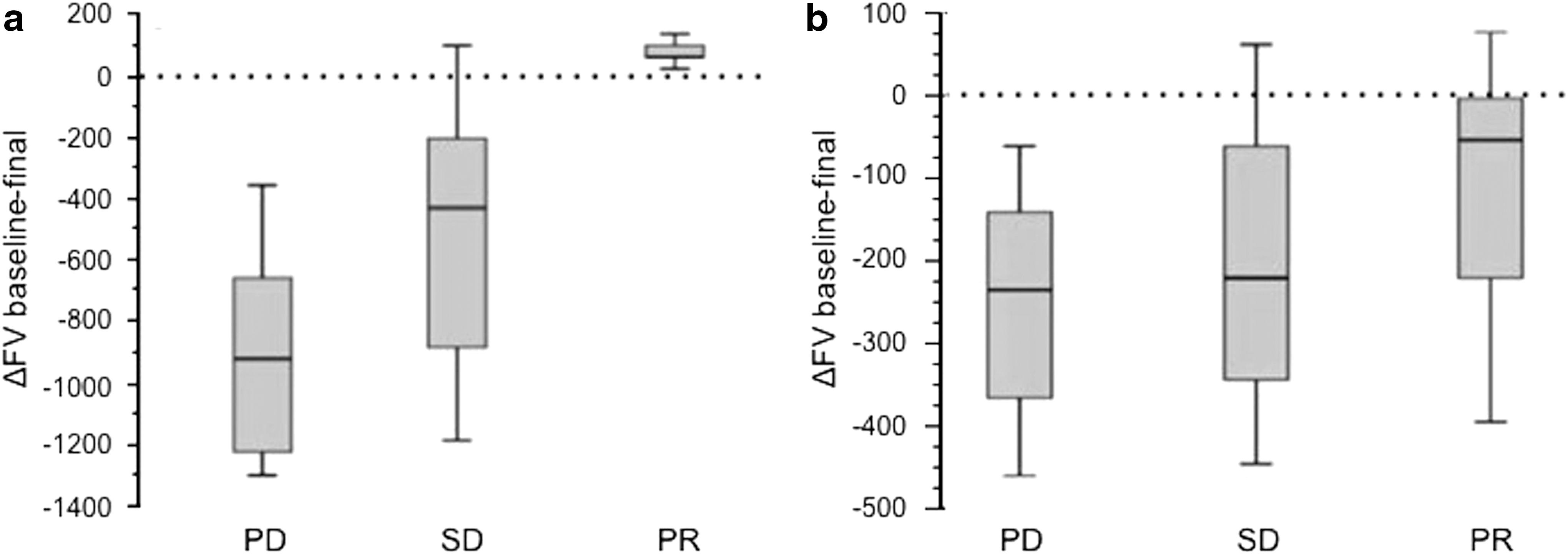
Reduction of FV between baseline and final 68Ga-DOTATOC PET/CT scans in lesions response according to the Response Evaluation Criteria in Solid Tumors (RECIST)
One patient out of the 11 treated with PRRT was not evaluated by RECIST criteria, since this patient presented only bone metastases.
EORTC, European Organization for Research and Treatment of Cancer.
Main PRRT toxicities were nausea (n=4/11) and asthenia (n=2/11), both grade 1. In 4/11 patients, we observed transient hematologic toxicity (grade 1): 2/11 leukopenia and 2/11 anemia. One patient experienced permanent renal toxicity (grade 2 that arose 16 months after therapy). A transient increase of transaminase levels (grade 1) was recorded in one case. We did not find a significant risk factor in terms of patient characteristics or administered PRRT activities for renal toxicity on multiple regression analysis.
Discussion
The outcome of DTC is excellent in the majority of cases. However, some patients exhibit more aggressive forms, unresponsive to conventional therapies. Partial or complete loss of 131I concentrating ability is usually associated with tumor dedifferentiation, and only 50% of patients with radioiodine-negative DTC will attain a disease-free status with conventional treatments (34). The loss of 131I concentration abrogates the utility of diagnostic 131I-WBS to detect residual/recurrent tumor. Therefore, in patients with negative diagnostic 131I-WBS and persistently elevated TG, [18F]FDG-PET and [18F]FDG-PET/CT has become the standard of care to localize residual/recurrent disease successfully (35). The incapability of dedifferentiated DTC cells to concentrate iodine has stimulated the search for therapeutic approaches alternative to 131I.
Several data about the role of somatostatin and somatostatin analogues as regulator of growth in normal and neoplastic thyroid tissue have been reported (36 –38). Recently, results have shown a high expression of all types of SSTRs in human nonmedullary thyroid carcinoma tissue (39). Based on these findings, SSTR imaging has been used to evaluate thyroid cancer patients with variable results (sensitivity 25–100%) (23,40) possibly due to major differences in study populations and in the imaging modalities used (32,41 –43).
In our series of patients, 68Ga-DOTATOC PET/CT detected SSTR expression in up to 58.5% of iodine-negative DTC. This finding was consistent with data previously reported in radioiodine-negative tumor lesions (36–82%) (44). Interestingly, [18F]FDG-PET has been reported to be more sensitive compared to 68Ga-DOTATOC in the detection of radioiodine-negative lesions (64% vs. 31%), but not in radioiodine-positive lesions (48% vs. 46%), introducing the concept of a concurrent loss of SSTR expression and radioiodine uptake in thyroid cancer cells (44).
Our results confirm the higher diagnostic performance of [18F]FDG compared to 68Ga-DOTATOC to stage radioiodine-negative DTC patients (82.9% vs. 58.5%). The combination of [18F]FDG-PET/CT and 68Ga-DOTATOC PET/CT improved metastasis detection (85.3%) in our series of patients. 68Ga-DOTATOC PET/CT cannot be considered as the first-line functional imaging modality in this clinical setting, except for the determination of SSTR status (45). Furthermore, it may disclose the opportunity for PRRT and may be superior to 111In-pentetreotide scintigraphy because of the higher affinity of the PET radiotracer for the SSTR type 2, the pharmacokinetic profile, the superior spatial resolution, as well as for the fact that it uses the same radiolabeled moiety employed for PRRT (45 –47).
Among the multiple factors analyzed, we did not find any predictor of [18F]FDG or 68Ga-DOTATOC positivity. In fact, similar uptake patterns in lymph nodes, parenchymal tissues (lungs and liver), and skeletal lesions were found. Additionally, none of the clinical variables included in the multiple regression analysis was associated with 68Ga-DOTATOC PET/CT positivity. Interestingly, all cases featuring negative [18F]FDG-PET/CT and 68Ga-DOTATOC PET/CT were PTC. This observation, which may suggest a differential SSTR expression based on the histological type, needs to be addressed in further studies.
SSTR expression at a level considered sufficient to give access to PRRT was found in 13/41 (32%) of our patients. Iten et al. (22) reported a higher rate of recruitment for PRRT in refractory DTC evaluated by Octreoscan scintigraphy. This difference may be explained by the different selection criteria used to admit patients to PRRT. In fact, we selected only patients with high SSTR expression on 68Ga-DOTATOC PET/CT, a modality of higher sensitivity as compared with Octeroscan scintigraphy (45), while previous experience excluded PRRT only in patients with completely negative SSTR imaging.
Dosimetric estimates obtained in this series of DTC patients were comparable to dosimetric results to critical organs reported in patients with advanced NETs (25). However, since we used only 111In-DOTATOC planar images for dosimetry, dosimetric estimates (especially for tumor lesions) may be affected by some limitations represented by a 2D approach and the relative low-resolution planar scintigraphy as compared to PET/CT (48). However, although we did not perform a comparative analysis between PET/CT and planar images, it is well known that 68Ga-DOTATOC PET/CT scanning is superior to 111In-DOTATOC planar images in terms of spatial resolution and that it shows more and/or smaller lesions (45). The use of planar scintigraphic images only may also explain why we did not find any relation between tumor dosimetry and outcomes.
90Y-DOTATOC PRRT induced disease control in 7/11 patients (2 PR and 5 SD) with a duration of response ranging from 3.5 to 11.5 months. An objective response in this series of patients was associated with a symptomatic response, as previously observed in patients with NET treated with PRRT (25,49). In particular, patients #4 and #7 registered a significant improvement of dyspnea and bone pain respectively.
As expected, PRRT toxicities were mainly hematologic and renal without significant differences from NET treated with this approach (25,49), although our patients had previously received high doses of 131I.
Treatment response evaluation is a critical aspect in patients with advanced, metastatic radioiodine-negative DTC. Ideally, patient survival may represent a strong indicator of treatment efficacy. Yet, prolonged survival is commonly seen even in patients with diffusely spread, progressive disease. An extended follow-up period on a large series of patients would therefore be required to accomplish this aim. Therefore, both serum markers and imaging findings are commonly adopted to evaluate treatment responses. Although RECIST criteria are the recommended criteria to evaluate treatment response, they are affected by some limitations, particularly in evaluating bone lesion responses. [18F]FDG uptake may also be extremely heterogeneous in case of metastatic radioiodine-negative DTC. Furthermore, the trend of serum TG levels in case of dedifferentiated tumors may not mirror the course of the disease (50,51).
In our series, the only 68Ga-DOTATOC PET/CT derived semi-quantitative parameter significantly associated with either single lesion or individual patient response according to RECIST criteria was the FV variation. This result is consistent with data previously reported for [18F]FDG-PET/CT in other types of cancer, in which FV changes have been successfully used to predict response to therapy (52). Therefore, as for results with 68Ga-DOTATOC in NETs (53), FV assessed by 68Ga-DOTATOC PET/CT seems to represent a valuable parameter to predict clinical improvement during patient follow-up. Despite data previously reported in the literature about the predictive role of SUVT/S (33), our results demonstrate no significant prognostic role of this parameter originally introduced to overcome limitations of SUV determination (54). Moreover, SUV parameters seem not to be adequate in this setting, since a decreased 68Ga-DOTATOC uptake in tumors could theoretically reflect loss of SSTR expression, a phenomenon known to occur in NETs undergoing dedifferentiation (55).
The identification of functional imaging parameters to define treatment response is critical for the evaluation of PRRT. In fact, when morphologic criteria are used to identify tumor response to PRRT in NETs, patients with SD or minimal treatment response showed similar survival rates compared to patients presenting PR (56,57). Furthermore, improved quality of life after PRRT does not seem to be clearly associated with a discernible morphologic response to therapy (58). In progressive medullary thyroid cancer, a significant clinical improvement induced by PRRT has been reported, in spite of minor effects in terms of decline in tumor lesions and serum calcitonin levels (43). This could be related to the pattern of cell damage induced by 90Y used for PRRT, which is supposed to last over time. Although the necrotic effects will continue to accumulate, the amount of necrotic and fibrotic tissue may result in unchanged lesion size on subsequent examination. This highlights the need for more sensitive imaging methods to monitor the response to PRRT. Thus, the use of functional images may be translated into PRRT response evaluation, as already applied in various tumors, with [18F]FDG-PET/CT (59 –63).
Our study has some major limitations: first, the small number of patients, and second, their clinical heterogeneity. Additionally, despite the fact that baseline [18F]FDG-PET/CT and 68Ga DOTATOC PET/CT presented discordant results in some patients, suggesting tumor heterogeneity, [18F]FDG-PET/CT was not repeated at the end of treatment to assess treatment response, making it impossible to compare treatment response with [18F]FDG-PET/CT and 68Ga DOTATOC PET/CT. Despite these unavoidable drawbacks, our preliminary results suggest a possible role for 68Ga-DOTATOC PET/CT in the diagnostic work-up of patients with radioiodine-negative metastatic progressive DTC. Moreover, in this clinical setting, PRRT may be a promising treatment option in selected patients, although further studies on larger series of patients are needed.
In conclusion, SSTR expression by 68Ga-DOTATOC PET/CT imaging was present in more than half of the patients with progressive radioiodine-negative DTC studied in our series. The combination of [18F]FDG-PET/CT and 68Ga-DOTATOC PET/CT provided an accurate disease restaging. Furthermore 68Ga-DOTATOC PET/CT allowed selecting patients suitable for PRRT. 90Y-DOTATOC PRRT induced disease control (PR and SD) in 7/11 of treated patients (duration response of 3.5–11.5 months). Main PRRT adverse events included nausea, asthenia, and hematologic and renal toxicities. 68Ga-DOTATOC PET/CT seems a reliable tool for both patient selection and evaluation of treatment response. In our experience, FV determination over time seems to represent a reliable parameter to determine tumor response to PRRT, although further investigations are needed to define its role better.
Footnotes
Author Disclosure Statement
All authors declare no competing financial interests exist.