
Abstract
Background:
Public health concern about nuclear activities have existed since the 1980s. Most studies on this subject investigated childhood leukemia. Thyroid cancer may be another health outcome of interest, because some nuclear installations are a potential source of radioactive iodine isotopes in the environment and because thyroid cancer is known to occur after exposure to these isotopes.
Methods:
This study describes an ecological study investigating whether there is excessive thyroid cancer incidence among residents living in the vicinity of nuclear sites. Single-site analyses using indirect standardization (standardized incidence ratios [SIRs]) and Poisson regression modeling (rate ratios [RRs]) were conducted. The proximity area is typically defined as a circular zone with a radius of 20 km centered on the site. However, the choice of the size of this area is somewhat arbitrary. Therefore, a sensitivity analysis was carried out to investigate whether the results vary with radii of increasing proximity.
Results:
No increased thyroid cancer incidence was found within the 20 km proximity area around the nuclear power plants of Doel (SIR=0.74 [95% confidence interval (CI)=0.64; 0.84] and RR=0.72 [95% CI=0.63; 0.83]) and Tihange (SIR=0.86 [95% CI=0.70; 1.01] and RR=0.85 [95% CI=0.70; 1.02]). For the sites of Mol-Dessel and Fleurus, where a combination of nuclear research and industrial activities are located, the incidences of thyroid cancer within the 20 km proximity area were higher than expected (Mol-Dessel: SIR=1.19 [95% CI=1.01; 1.36] and RR=1.19 [95% CI=1.02; 1.38]; Fleurus: SIR=1.15 [95% CI=1.02; 1.28] and RR=1.17 [95% CI=1.04; 1.33]). For Chooz, a French nuclear power plant close to the Belgian border, the results were unstable as a result of the small population denominator. For all Belgian nuclear sites, the results were generally insensitive to the choice of the proximity area.
Conclusions:
No evidence for excessive thyroid cancer incidence around the Belgian nuclear power plants was found. On the other hand, an increased incidence of thyroid cancer was observed around the sites with other nuclear activities. Further research is recommended to verify whether the observed increases could be related to the site-specific nuclear activities.
Introduction
T
In 2008, the public health concern with regard to nuclear activities was intensified worldwide by the publication of the German KiKK study, a large-scale case-control study that showed a significantly increased risk for solid cancers and leukemia among children living within 5 km of nuclear power plants in Germany (2,8,9). In Belgium, the incidental gaseous release of 131I that occurred in 2008 at the Institute for Radio-Elements (IRE) in Fleurus, one of the major production sites of radioiodines in Europe, further elevated public concern. In the 2008 incident, rated as INES-3, an estimated 48 GBq of 131I was released into the environment over 4 consecutive days. The postincident investigation indicated points of serious concern with regard to both the operational safety and the management of the Fleurus site (10,11) and hence, the presence of earlier exposures cannot be ruled out.
In response to both the publication of the KiKK study and the incident at Fleurus, the Minister for Social Affairs and Public Health commissioned a nationwide epidemiologic study to explore health risks associated with living in the vicinity of nuclear sites in Belgium. As it was the first study of its kind in Belgium, a multidisciplinary research group decided that this study was to adopt an ecological approach using data that were readily available and should focus on acute childhood leukemia and on thyroid cancer. The study was carried out by the Belgian Scientific Institute of Public Health (WIV-ISP), in collaboration with the Belgian Cancer Registry (BCR) and the Federal Agency for Nuclear Control (FANC). The present study describes the analyses investigating whether thyroid cancer incidence (all ages) in the vicinity of the nuclear sites is higher than expected. A second approach, investigating the hypothesis of a gradient in thyroid cancer incidence with increasing levels of simulated exposure as well as the results for acute childhood leukemia are reported by Bollaerts et al. (12).
In the more developed regions of the world, thyroid cancer represents 1.8% of all cancers (13). It is, however, the most common malignancy of the endocrine system, including a variety of histologic types of neoplasia, in particular papillary and follicular cancers. The incidence of thyroid cancer in women is approximately threefold higher than in men (14). Over the past 30 years, the incidence of differentiated thyroid cancers represented by the papillary type has increased in many countries. A study across five continents revealed an average increase of 67% in females and of 48% in males between 1973 and 2002 (15). The reasons for this increase in thyroid cancer incidence are not yet completely understood. One possible explanation is the increasing use of diagnostic techniques to detect thyroid cancer (16). However, recent studies suggest that other factors may be involved in the increasing incidence of thyroid cancer (17,18). Established risk factors for thyroid cancer include exposure to ionizing radiation and iodine deficiency, whereas putative risk factors include obesity, occupational exposures to certain chemical pollutants, genetic factors, and female sex hormones.
Exposure to ionizing radiation, particularly during childhood, is the best established risk factor associated with thyroid cancer (19). Studies on patients treated by radiotherapy, on survivors of the atomic bombings, or on people exposed in nuclear accidents, have demonstrated a significantly increased risk for developing thyroid carcinomas following radiation exposure during childhood. After the Chernobyl reactor accident in 1986, ∼1.8 EBq of 131I was released into the atmosphere. In Belarus and Ukraine in particular, childhood thyroid cancer, mainly of the papillary type, started to increase less than 5 years after the accident (20,21). Nuclear facilities, including those investigated in the current study, can release 131I into the environment, not only accidentally but also during routine operations.
The aims of the current study are twofold: (i) to investigate whether there is an excess of thyroid cancer in the vicinity of the nuclear sites in Belgium, and (ii) to evaluate these associations for different definitions of the proximity area of the nuclear sites.
Materials and Methods
Data
Thyroid cancer incidence data (ICD-10 C73) were requested from the Belgian Cancer Registry (BCR), a population-based registry. The data were available at the level of the communes, the lowest administrative level at which age- and sex-specific cancer data are currently available in Belgium. In particular, Belgium has a total of 589 communes, divided over the Flemish (n=308), Walloon (n=262), and Brussels-Capital regions (n=19; Fig. 1). The incidence year and the place of residence are defined at the moment of cancer diagnosis. Cancer data of the Flemish Region were available for the diagnosis years 2000–2008. For the Walloon and Brussels-Capital regions, cancer data were available for the diagnosis years 2004–2008.
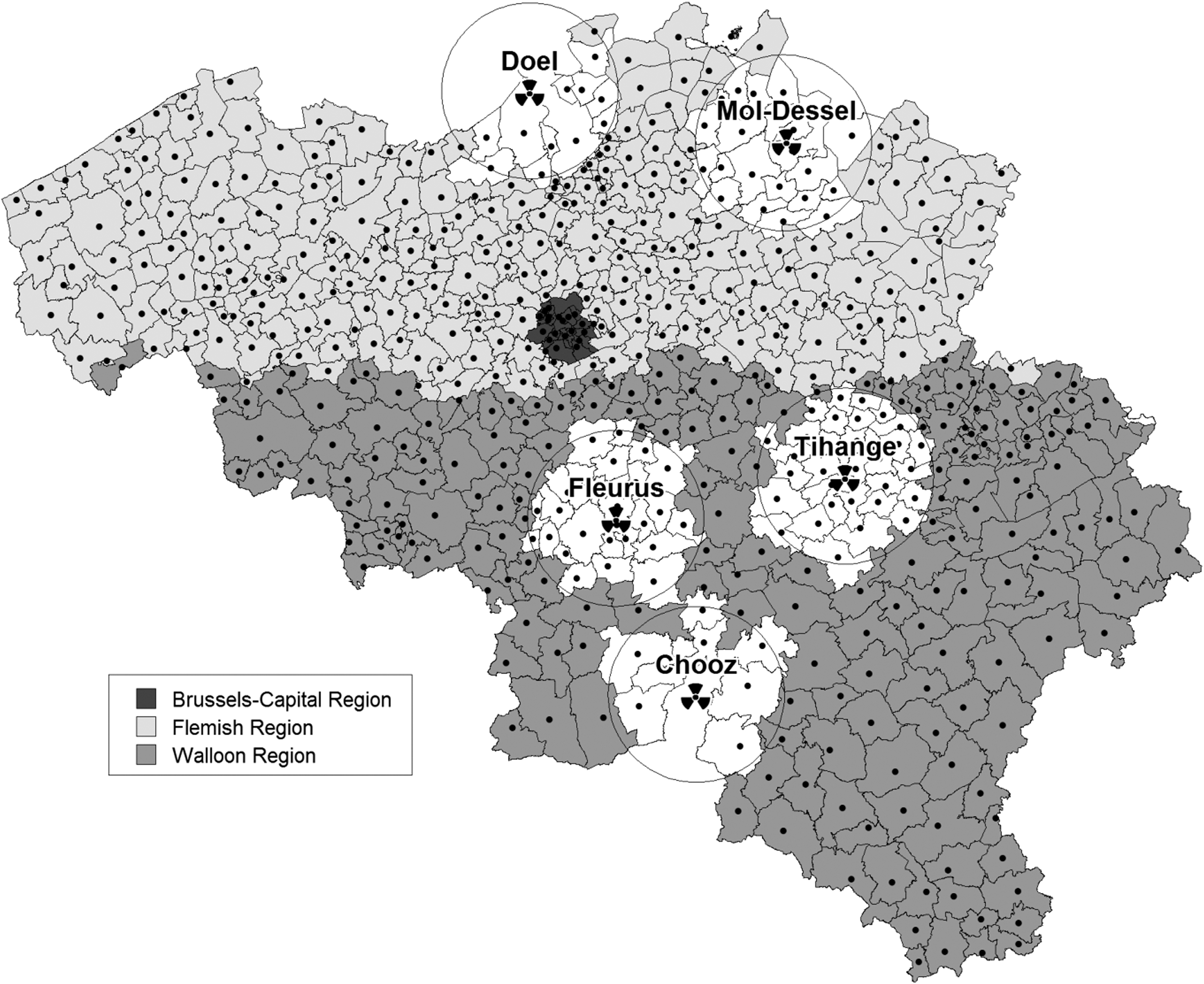
Map of Belgium depicting the nuclear sites, the communes' centroids, and the 20 km radius proximity areas (white) around the nuclear sites.
Population data by sex, 5-year age groups, and commune of residence were obtained from the Belgian Federal Public Service (FPS) Economy, Directorate-General Statistics and Economic Information, for every year from 2000 to 2008. In 2008, Belgium had a total population of 10,666,866 inhabitants, divided over the Flemish (n=6,161,600), Walloon (n=3,456,775), and Brussels-Capital regions (n=1,048,491).
Nuclear sites
The nuclear sites of interest are the four Belgian civil nuclear facilities of Class 1 [defined as facilities with the highest radiologic risk (22)] and the French nuclear facility of Chooz, which is located ∼3 km from the Belgian border. An overview of the nuclear sites with their main type of activity, the initial year of operation, the number of reactors, and the total capacity of the sites is given in Table 1. Doel (Flemish region), Tihange (Walloon region), and Chooz (France) are electricity-generating nuclear power plants. Several facilities in nuclear research and nuclear industry are situated on the sites of Mol-Dessel (Flemish region) and Fleurus (Walloon region). The nuclear site of Mol-Dessel primarily consists of the Belgian Nuclear Research Centre (SCK-CEN), the Class 1 operator with the highest potential source term at the site. Finally, the nuclear site of Fleurus primarily consists of the Institute for Radioelements (IRE), one of the major production sites of radioiodines for usage in diagnostic and therapeutic nuclear medicine in Europe. IRE is therefore a major potential source of 131I emissions.
NPP, nuclear power plant; PWR, pressurized-water reactor; BR, Belgian reactor; VENUS, Vulcan Experimental Nuclear Study; HADES, high activity disposal experimental site; MOX, mixed oxides; MWe, megawatts electric; MWth, megawatts thermal; IRE, Institute for Radio-Elements; SCK-CEN, Belgian Nuclear Research Center; IRRM, Institute for Reference Materials and Measurements; FBFC, Franco-Belge de Fabrication Combustible.
Proximity areas
For each of the 589 Belgian communes, distances were calculated between the commune's centroid and the geographical location of the nuclear sites. The locations of the sites were determined by locating the nuclear facilities. For Doel, Tihange, and Chooz, a point amidst the respective four, three, and three reactor buildings was determined. For Mol-Dessel, the geographical coordinates correspond to chimney BR1 of SCK-CEN, whereas for Fleurus the coordinates correspond to chimney B6 of IRE. Then, the proximity area of a site was constructed as the aggregation of communes having their centroid lying within a circle of radius r centered on the site. Typically, the radius r is taken to be 20 km (Fig. 1), as it corresponds to the perimeter used for nuclear power plant emergency plans, and as it is often used within the literature for this type of studies (2,9,23 –25).
Statistical methods
Exploratory analyses
Thyroid cancer incidence was first explored as a function of some epidemiologic covariates, namely age, sex, time, and geographical location. These covariates were selected because they have been identified in the literature to play an important role in the epidemiologic patterns of thyroid cancer and because they are available at the commune level within the BCR.
The occurrence of thyroid cancer as a function of age and sex was evaluated by means of age (5-year age groups) and sex-specific incidence rates, whereas time and regional trends were investigated by calculating the age- and sex-standardized rates (European Standard Population). The Poisson approximation was used to obtain the 95% confidence intervals (CIs).
Relative risk
Single-site analyses were performed using two approaches, i.e., indirect standardization (age- and sex-adjusted standardized incidence ratios [SIRs]) and Poisson regression modeling, to investigate whether there is an excessive thyroid cancer incidence among residents living in the vicinity of nuclear sites. The SIRs were calculated using regional reference populations, as regional differences in thyroid cancer incidences are large. This means that the areas in proximity to the nuclear sites of Doel and Mol-Dessel were compared with the whole Flemish region whereas the areas in proximity to nuclear sites of Fleurus, Tihange, and Chooz were compared with the whole Walloon and Brussels-Capital regions. Confidence intervals were obtained using the Wald method.
The SIRs were complemented with single-site Poisson regression models. For rare diseases and aggregated data, Poisson regression models are a natural choice to compare cancer incidences between populations while accounting for several covariates (26). The regression parameters of the Poisson model have a good epidemiologic interpretation. Indeed, the exponent of the regression parameter for a binary variable is the incidence rate ratio (RR). For example, let the binary variable Xk refer to living (Xk =1) or not living (Xk =0) in the proximity of a nuclear site. Then exp(βk ) is to be interpreted as the disease risk for a person living in the proximity of a nuclear site compared to the disease risk for a person not living in the proximity of a nuclear site, given all other covariates remain the same. As such, an RR>1 (<1) means that the disease risk is larger (smaller) when Xk =1 compared to when Xk =0 and an RR close to 1 means that risks are similar in both cases.
The model was built by including the main effects of (i) proximity to the nuclear site (defined using a circle centered at the nuclear site having a 20 km radius r), (ii) 5-year age groups, (iii) sex, (iv) time, and (v) region (Walloon and Brussels-Capital regions vs. Flemish region; Table 2). To reflect the results of the exploratory analyses, a quadratic term for age group and interactions between sex and age group and between incidence year and region were included as well.
To decide upon model simplification, backwards selection was adopted using Wald tests at a significance level α=0.05. Proximity to the nuclear site, the independent variable of main interest, was not considered for exclusion. Confidence intervals of the RRs were calculated using the delta-method. To account for overdispersion, the model was fitted using the quasi-likelihood approach with Pearson-based overdispersion parameter φ (27).
Sensitivity analysis
Although crucial, the choice of the size of the proximity area is to a certain extent arbitrary. Therefore, a sensitivity analysis was conducted by varying the radius r of the circles used to determine the proximity areas. More precisely, for every r, with r=1,2,…25 km, the SIRs and RRs were calculated as above, allowing to investigate whether the results vary with expanding proximity areas.
Results
Exploratory analyses
The age- and sex-specific incidence rates of thyroid cancer (Fig. 2) were significantly higher among women compared to men for the ages ranging from 20 to 79 years. Taking all years together, a male:female ratio of 1:3 was obtained. Thyroid cancer is mainly affecting middle-aged people, with a peak at the age of 55–59 years, both for women and men. In contrast, thyroid cancer rarely occurs in children.
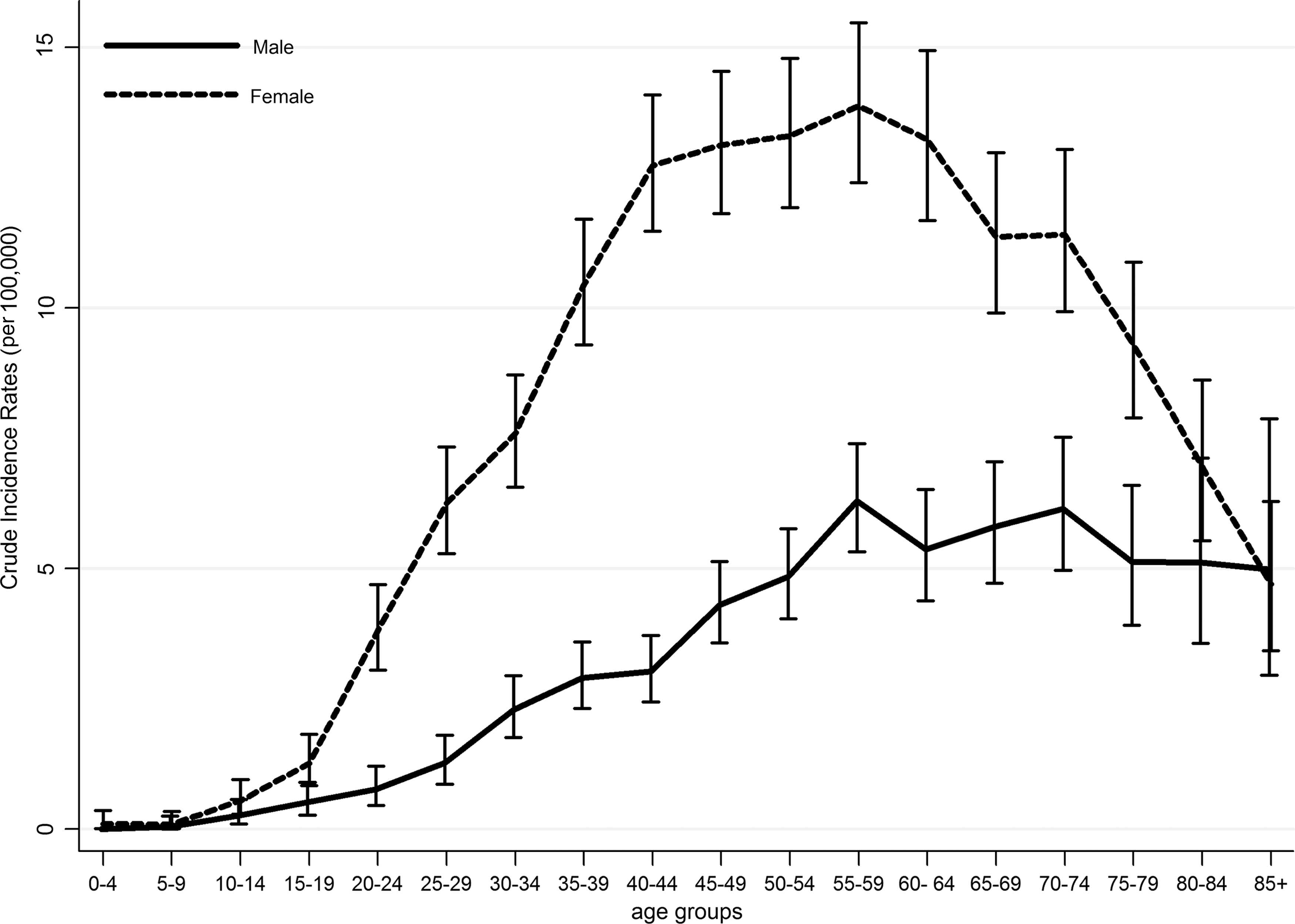
Age- and sex-specific incidence rates of thyroid cancer in Belgium, 2000/2004–2008.
The European standardized incidence rates (ESR) of thyroid cancer (Fig. 3) were significantly lower in the Flemish region compared to the Walloon and Brussels-Capital regions. Within the Flemish region, the thyroid cancer incidence has been steadily increasing over time with the incidence in 2008 being significantly higher than that of 2000. This increasing time trend was not observed in the Walloon and Brussels-Capital regions, possibly because of the shorter time period of registration.
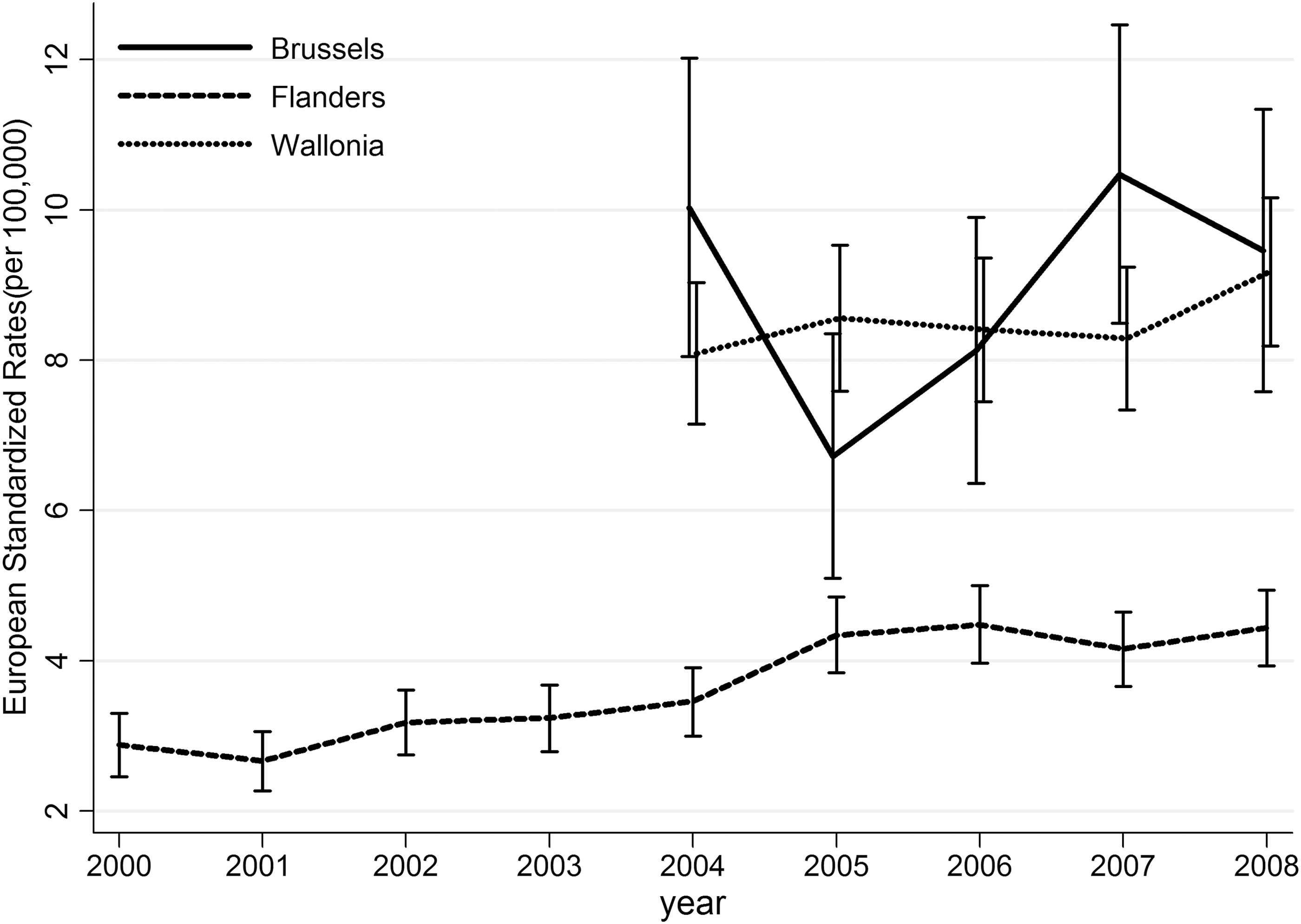
Age- and sex-standardized rates (European Standard Rate, ESR) of thyroid cancer by year of diagnosis and region in Belgium, 2000/2004–2008.
Relative risk
The results of the single site analyses investigating the evidence of an excess of thyroid cancer incidence within the 20 km proximity area are summarized in Table 3. Both the indirect standardization (SIRs) and Poisson regression (RRs) full model, which could not be simplified, yielded similar results. For the nuclear power plants of Doel and Tihange, a lowered thyroid cancer incidence was found within the 20 km proximity area. For Doel, this difference was significant (SIR=0.74 [95% CI=0.64; 0.84] and RR=0.72 [95% CI=0.63; 0.83]), whereas it was not for Tihange (SIR=0.86 [95% CI=0.70; 1.01] and RR=0.85 [95% CI=0.70; 1.02]). A significantly increased thyroid cancer incidence was found around the nuclear sites of Mol-Dessel (SIR=1.19 [95% CI=1.01; 1.28] and RR=1.19 [95% CI=1.02; 1.38]) and Fleurus (SIR=1.15 [95% CI=1.03; 1.30] and RR=1.17 [95% CI=1.04; 1.33]), the two sites with combined industrial and research activities. For the French nuclear power plant of Chooz, the SIR was not significant (SIR=1.47 [95% CI=0.93; 2.00]), whereas the RR was borderline significant [95% CI=1:02; 2:10]. However, the small population denominator for the Belgian territory around the nuclear power plant of Chooz resulted in large confidence intervals and unstable results.
RRs are calculated as exp(β 1) based on the Poisson regression model.
Walloon/Brussels-Capital region as reference region.
Flemish region as reference region.
PY, person years at risk; O, observed number of cases; E, expected number of cases; SIR, standardized incidence ratio; RR, rate ratio; est., estimated; CI, confidence interval; +, significantly increased incidence; −, significantly decreased incidence.
Sensitivity analyses
The results of the sensitivity analysis, investigating whether the RRs vary with expanding proximity areas, are graphically displayed in Figure 4 for increasing radius r with r=1,2,3,…,25 km. The SIRs resulted in similar estimates and are not shown. For the nuclear power plants of Doel and Tihange, no excess in thyroid cancer incidence was observed, irrespective of the size of proximity area.
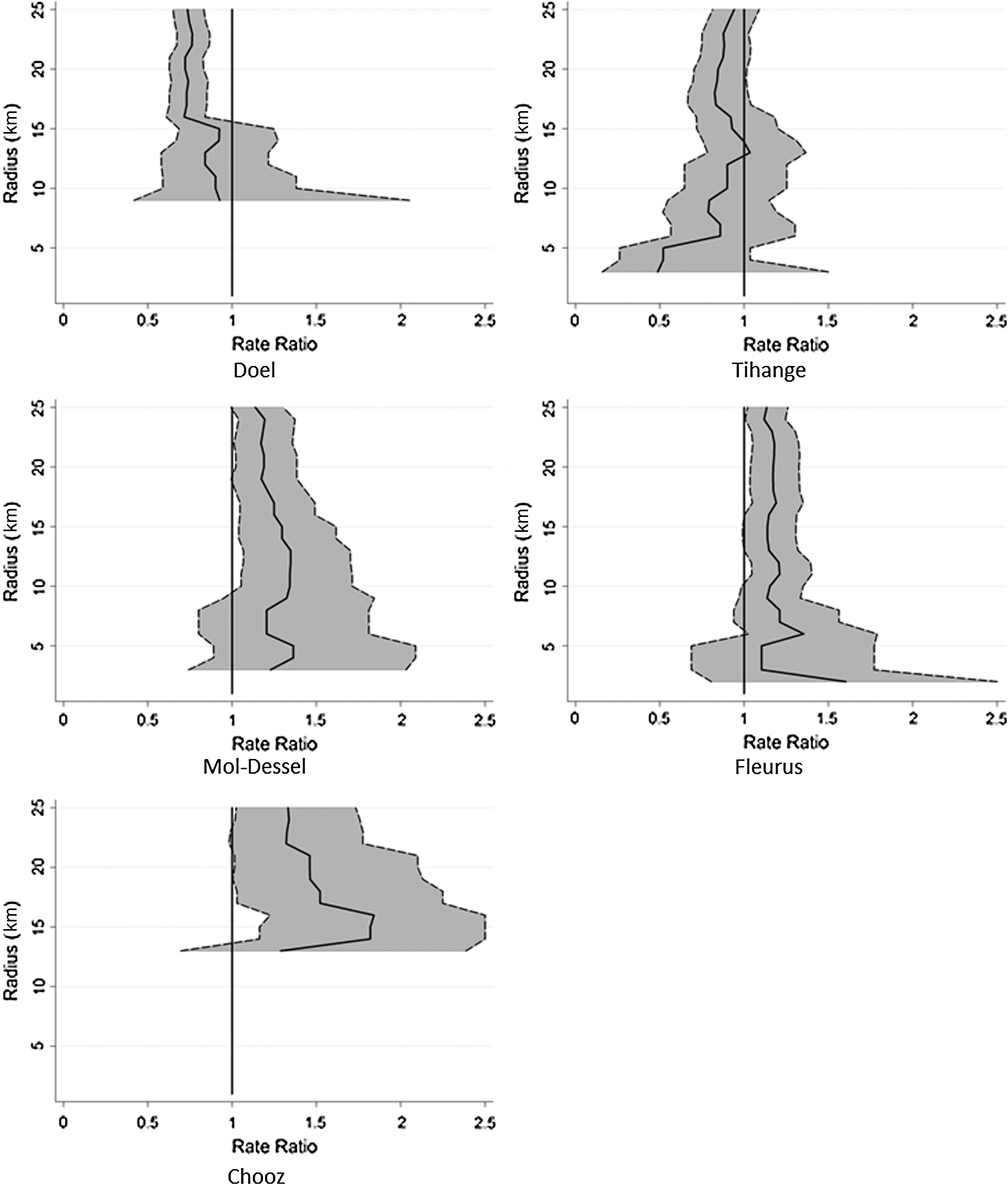
Incidence rate ratios (RRs) of thyroid cancer in the vicinity of nuclear sites by increasing circle radius (km) of the proximity area. The 95% confidence intervals are represented by the dotted lines.
For the nuclear sites of Fleurus and Mol-Dessel, significant excesses in thyroid cancer incidence were regularly found for proximity areas with radii from ∼10 to ∼25 km. Around the nuclear power plant of Chooz, significance showed to be sensitive to varying radii of the proximity area. Observe that all confidence intervals narrow for increasing radius r as the population denominator increases.
Discussion
This article presents the first Belgian study investigating health risks associated with living in the vicinity of the largest nuclear sites. This study is in response to the public health concern following the accidental gaseous release of 131I in 2008 in Fleurus, one of the major production sites of radioiodines in Europe. Because the study has been ordered for the whole of Belgium, it focused on all Class 1 installations [defined as facilities with the highest potential radiologic risk (22)] including the Fleurus site. All of these installations may be potential sources of radioisotope release from accidental emissions and during routine operations. The multidisciplinary research group that had been launched after the Fleurus 2008 incident advocated the use of an ecological study design, because the study was to (i) be a first approach to answer the question on possible increased health risks around nuclear facilities and (ii) make use of data that were readily available. To this end, the cancer incidence data from the BCR, which is a population-based registry for the whole of Belgium, were used.
The health outcome of interest described in the current study is thyroid cancer. This specific type of cancer is known to occur after exposure to radioactive isotopes of iodine. For the current study, thyroid cancer incidence data were available for the period 2000/2004–2008. The cross-section of thyroid cancer cases of all ages (from 0 until 85+ years) was taken. It should be noted that the ecological design and the time window of the available data do not allow investigating the health effects of the Fleurus 2008 incident itself. Instead, as the cross-section over all ages was taken, it allows investigating the potential health effects of (possibly undetected or unreported) past exposures. In addition, the uncertainty and heterogeneity in latency period is accounted for by taking the cross section over all ages. The two main pathways of exposure from release of radionuclides in the atmosphere by nuclear installations are gamma radiation and ingestion of radionuclides through food contamination. The ecologic design allows taking into account only the first pathway. This is also the way the population around the nuclear sites is mostly exposed. Furthermore, as a result of the open food economy in Belgium, the exposure through food contamination is generally not considered to be a geographical risk factor around the nuclear sites themselves.
Based on arguments presented by Korblein and Hoffmann (8) and by Fairlie (28), more advanced statistical analyses techniques were used. In particular, the indirect standardization method (SIRs) was complemented with Poisson regression models (incidence RRs). These models are advantageous over SIRs because they enhance model flexibility, allowing more covariates to be taken into account simultaneously and to elaborate on more evolved (exposure) modeling (29). More specifically, the Poisson regression enabled accounting for the observed increasing time trend in thyroid cancer incidence in the north of Belgium and for the regional differences in thyroid cancer incidence that were observed between the northern and the southern part of Belgium. In addition, the classic analyses on the 20 km proximity area were complemented by sensitivity analyses to investigate whether the results vary with expanding proximity areas. Indeed, as the choice of the proximity area is to a certain extent arbitrary, and as it has been shown that the model results can depend on this choice (30), a sensitivity analysis is highly recommended to test the robustness of the model results to the choice of proximity area.
Based on the current analyses, no increased incidence of thyroid cancer was found around the nuclear power plants of Doel and Tihange. In contrast, increases of 20% in thyroid cancer incidence were observed around the two nuclear sites where a combination of nuclear research and industrial activities are located. These results around the Belgian sites were robust to the choice of the size of the proximity area. Finally, the small number of expected cases for the Belgian territory around the French nuclear power plant of Chooz gave unstable results, and thus did not allow for any scientifically valid interpretation.
Because the increased thyroid cancer incidences were observed around the two nuclear sites with research and industrial activities and not around the nuclear power plants, it could be hypothesized that these differences are associated with differences in exposure or risk between the two types of sites. Radiation-induced thyroid cancers are characterized by a long latency period and individual variation in latency time exists (31). Generally, latency times between 10 and 15 years (and in some studies even up to 40 years) have been described in the literature (6,7,32), when this irradiation concerns children less than 15 years old. Exposure during adulthood (after the age of 20 years) has not been linked convincingly to thyroid cancer (33). The Chernobyl accident, however, demonstrated that latency times may be much shorter when exposure occurs at younger age and may also decrease with increasing exposure (21). This difference is explained by the higher sensitivity of children to ionizing radiation. The dose received by the thyroid of a child is higher than that of an adult exposed in the same conditions because of the lower volume of the thyroid gland and the more pronounced concentration phenomenon in children compared to adults (34). Moreover, young children have an increased susceptibility to cancer induction compared to adults, mainly related to their higher mitotic index (35). Therefore, supplementary analyses were performed comparing age-specific incidence rates of thyroid cancer within the proximity area of Mol-Dessel and of Fleurus with the corresponding rates of the respective reference population. In the younger age groups, the number of cases were low and no significant increases were observed (results not shown).
A number of studies have addressed the question of a possible association between thyroid cancer and exposure to ionizing radiation coming from nuclear sites. Thyroid cancer and thyroid nodules have been described following the atomic bombings in Hiroshima and Nagasaki due to external exposure (32,36 –39). The follow-up of the Life Span Study cohort of Japanese atomic bomb survivors showed excess relative thyroid cancer risks of 1.15 for the period 1958–1987 (39) and 1.28 for the period 1958–2005 (37) at 1 Gy of radiation exposure. Positive associations have also been described due to internal exposure following radioactive fallout. For some nuclear facilities and sites with specific high-risk activities, e.g., nuclear weapons testing sites, excessive thyroid cancer caused by radioactive fallout have been reported in relation with both periodic releases during routine operations and with accidental exposures. As such, an increased risk of thyroid neoplasms was observed in children living in Utah, Nevada, and Arizona who had been exposed to radioactive iodine from nuclear weapons testing at the Nevada test site from 1951 through 1962 (40,41). Similarly, a cohort study in the former USSR found cancer mortality to be substantially higher in inhabitants of villages exposed to the nuclear tests that occurred between 1949 and 1989 at the Semipalatinsk nuclear test site (42). With regard to accidents, an excess of thyroid abnormalities, including cancer, was observed after the 1954 BRAVO thermonuclear test on the Marshall Islands in the Pacific Ocean (43,44). In French Polynesia, a population-based case-control study, carried out after the atmospheric nuclear weapon tests in the Mururoa and Fangataufa atolls, found that the risk of thyroid cancer increased significantly with the thyroid dose received before the age of 15 years (45).
For nuclear power plants, excessive thyroid cancer caused by radioactive fallout has been observed only after major accidents. This was the case following the Chernobyl reactor accident in 1986, after which thyroid cancer, particularly of the papillary type, dramatically increased in children in Belarus and Ukraine only 4 years after the accident (21,34,46,47). Excess relative risks/Gy of 8.0 [95% CI=4.60; 15.00] and 19.0 [95% CI=11.00; 27.00]) have been reported in two recent studies (48,49). To the authors' knowledge, no increases of thyroid cancer have been reported for nuclear power plants in case of smaller accidents/incidents [Windscale Sellafield, England, 1957 (50,51); Three Mile Island, Pennsylvania, 1979 (52)] or after routine operations (53,54). It should be noted that substantial debate remains with regard to the dose-effect relationships in all of these studies, even in the case of Chernobyl, because exact doses are not known (55). Finally, it has to be stressed that the implementation of an intensive screening follow-up program after nuclear events may induce in itself the detection of more cancer cases and hence be responsible for an apparent increase in incidence (screening bias) (56).
A number of studies have also investigated the occurrence of thyroid cancer in nuclear workers (57 –59). In these studies, no consistent pattern of increase for any single cancer type was observed across cohorts. It should be noted that these studies predominantly included male workers, and workers are not exposed during the most critical period for thyroid cancer induction (early childhood).
Because of the ecological design of this study, however, no causal relationships can be inferred nor can conclusions at the individual level be drawn. Furthermore, migration phenomena cannot be taken into account. Other causes could be considered, such as predisposing thyroid disease (60), thyrotropin levels (61,62), the role of other hormones such as estrogens (63), heritable conditions (64), physical characteristics such as obesity (65), medical radiation (66), dietary iodine (67), or smoking status (68). Some factors, such as advances in diagnostic practices and differences in pathologic analyses, may also affect the incidence of thyroid cancer not by a true increase, but by an increased number of findings. Advances in diagnostic practices may lead to increasing rates of small tumors that remain otherwise undiagnosed (16,69,70). On the other hand, thyroid cancers may also be overdiagnosed because of increased pathologist scrutiny, such as increased sectioning and histologic sampling by pathologists (17,71). Indeed, an additional study by the Belgian Health Care Knowledge Center (72) showed more thyroid surgery as well as more thyroid imaging, and thus a higher proportion of small tumors, in Brussels and Wallonia as compared to Flanders. Further detailed information on potential differences in medical diagnostic practices within the regions are, however, not available at this moment in Belgium. Nevertheless, it has to be stressed that the etiology of thyroid cancer remains largely unknown.
Because the current study indicates borderline increased incidences of thyroid cancer around the nuclear sites of Mol-Dessel and Fleurus, further research is recommended. In first instance, as the etiology of thyroid cancer is still largely unknown, more advanced surrogate exposure models were used to verify whether the observed incidences could be related to nuclear activities. In view of this, three surrogate exposures were tested, i.e., residential proximity to the nuclear sites, prevailing wind directions, and simulated radioactive discharges into the environment on the basis of mathematical modeling (12). Second, it was suggested to make cancer data available at a smaller geographical level. These data are expected to be available in the near future, and will allow repeating the analyses with greater geographical detail and for an extended time period.
Footnotes
Author Disclosure Statement
No competing financial interests exist.