
Abstract
Background:
In the last decade, significant contributions have been made to our knowledge on the connection between the thyroid and adipose tissue. Modern society is faced with climbing rates of obesity and metabolic syndrome, and there is accumulating evidence of an association between obesity and increased cancer risk. The aim of this review is to summarize clinical data on the association between thyroid cancer (TC) and obesity and briefly to present plausible hypotheses explaining this interplay.
Summary:
We performed a search on the PubMed database for studies published in English from 1980 to March 2013 using the terms “thyroid cancer,” “obesity,” and “body mass index.” Although there is inconsistency among the clinical studies, it seems that overweight and obesity are related to a modestly increased TC risk. Various factors, such as sex, ethnicity, and body changes during certain life periods, for example adolescence, may influence the association between obesity and TC risk. There are preliminary data linking obesity with a less favorable clinicopathologic profile of TC. However, validation with larger multicenter studies is needed. The precise underlying mechanisms have not yet been elucidated, but the insulin–IGF axis and adipokines, such as leptin and adiponectin, might be implicated in the link between excess weight and TC.
Conclusions:
Given the rising prevalence of TC and the development of obesity as an epidemic, it is important to clarify its connection with TC as well as the mediating pathways. However, unless this association is confirmed and causation proven, screening for TC in overweight and obese subjects—a rapidly increasing body of the general population—does not seem justified.
Introduction
T
Review
Association of obesity with thyroid cancer risk
In recent decades, the incidence of TC has increased along with a marked rise in obesity rates (6). As shown in Figure 1, the increase in obesity rates preceded the rise of TC prevalence by some years, and although there is no sharp rise in the incidence of the latter, the two curves show a parallel steady increase after a certain point. Several studies have evaluated the effect of obesity on TC risk. In one of the first reports, Ron et al. identified a positive relation between obesity and TC risk in women (7). In a similar vein, Goodman et al. performed a population-based study and showed more than a fivefold increase in the risk for TC among males, and more than a twofold increase among females in the highest compared to the lowest quartiles of weight (8). In a large meta-analysis including 282,137 cancer patients, a 5 kg/m2 increase in body mass index (BMI) was related to a slightly higher TC risk (hazard ratio [HR] 1.14 [95% confidence interval (CI) 1.06–1.23] in females, and HR 1.33 [CI 1.04–1.7] in males) (5). Similarly, in a pooled analysis of five prospective studies examining a total of 434,953 males and 413,989 females, increasing BMI was associated with a higher risk for TC in both men and women after adjusting for potential confounding factors (9). In accordance were the results of a meta-analysis by Zhao et al. (10), the risk of TC was significantly increased in the presence of excess body weight, either overweight or obesity (odds ratio [OR] 1.18 [CI 1.11–1.25]). According to a recent systematic review, most studies agree that obesity is positively but modestly correlated with TC risk. However, the risk estimates range widely from 1.1 to 2.3 in men and 1.0 to 7.4 in women (11).
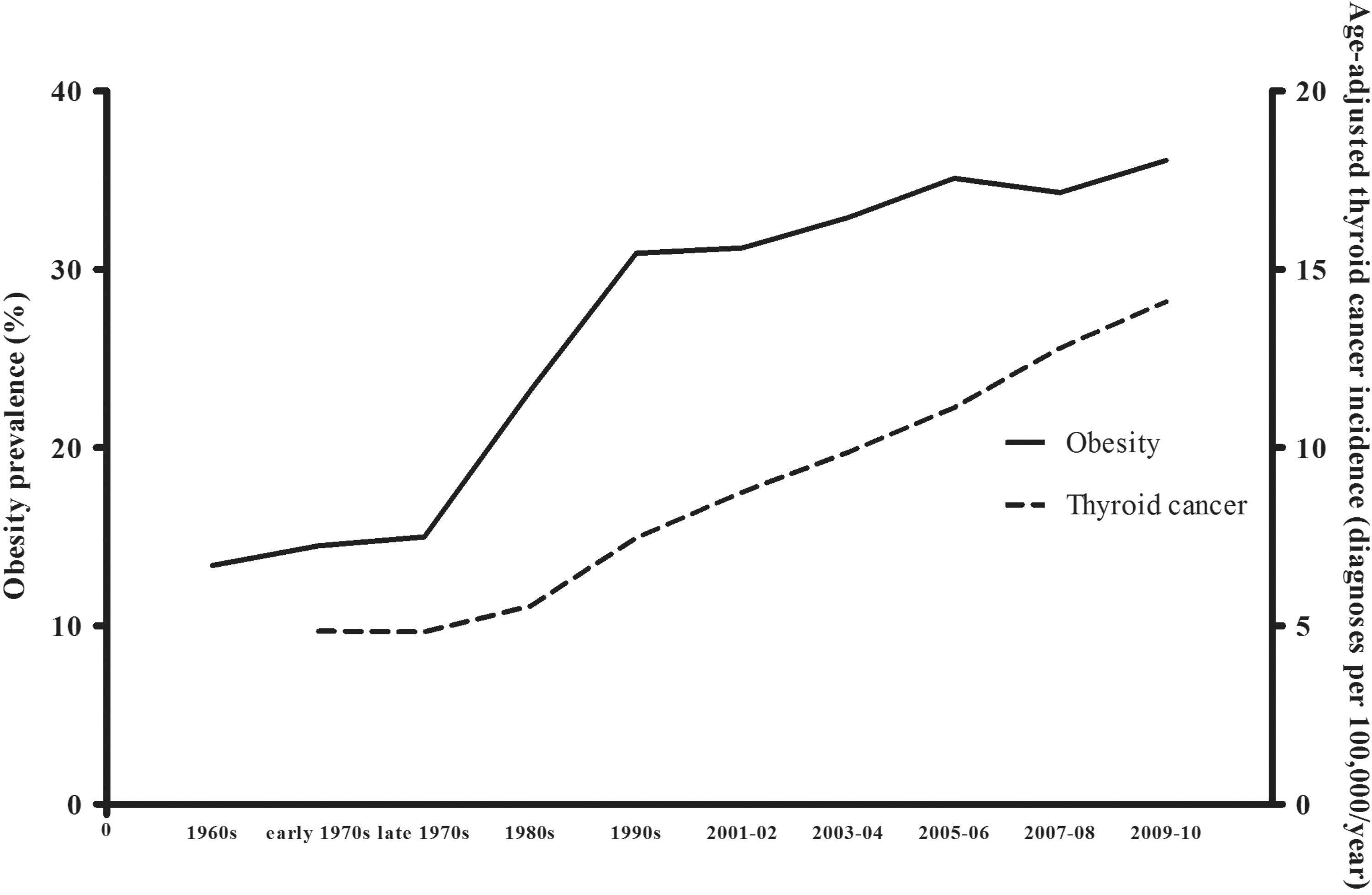
Obesity prevalence and age-adjusted thyroid cancer incidence in the United States; trends from 1960 through 2010 using data from the National Health and Nutrition Examination Survey (for obesity rates) and the National Cancer Institute's Surveillance Epidemiology and End Results data set (for thyroid cancer).
It is likely that sex influences the association of obesity status with TC, as several studies have found such associations only in women. In a population study performed in New Caledonia, BMI was found to be strongly related to TC risk in women but not in men (12), and a similar association was reported in a European prospective study by Rinaldi et al. (13), who found an association of TC risk with obesity only in women (HR highest vs. lowest BMI quintile 1.41 [CI 1.03–1.94]). Likewise, in an American cohort studied by Meinhold et al., only women with a BMI >35 kg/m2 (and not men) had a significantly higher risk of TC compared to normal-weight individuals (14). Higher BMI was also related to increased TC incidence in women in the prospective European cohort study by Almquist et al. (15). Similarly, in a recent large Korean study that used thyroid ultrasonography screening in 15,068 euthyroid subjects, obesity was found to be significantly related to TC risk in women. This finding was independent of age, smoking, and TSH levels. Again, this relation was not significant in males (16).
Hence, it may well be that the strength of the association of TC risk with obesity is heightened in the female population. Yet, there are also reports that elevated BMI is linked with TC risk in both sexes, or even only in males. In a large Norwegian study comprising two million participants, BMI was positively associated with TC in both sexes, but the degree of this relation was modest (17). It appears that there is considerable discrepancy between the various epidemiological reports. In a 10-year follow-up cohort of 781,283 Korean men, a significant relation of obesity with papillary thyroid cancer (PTC) was reported (18), in accordance with a study performed in American male veterans (19). Somewhat different results were reported from a prospective study of 484,326 American subjects followed up for eight years, where a higher TC incidence with increasing BMI was found in men but not in women (20). To summarize, although there is no uniform conclusion, most studies support a stronger association of obesity with TC risk in the female population. However, one should acknowledge that this could be partially attributed to the lower incidence of TC in men and, consequently, to the low statistical power of studies performed in male subjects.
Besides the effect of current BMI status, there is also accumulating data on the role of anthropometric parameters during certain life periods or significant changes in body weight and their relation to TC risk. Weight gain during the transition from early to late adulthood was significantly associated with TC risk in postmenopausal women, but this relation was not significant in premenopausal individuals (8). Body weight in early adulthood was identified as a significant risk factor for TC in a case control study. In the same study, current BMI was identified as an independent risk factor for TC in the overall analysis after adjusting for age and other confounding variables, whereas high BMI during early adulthood was significantly related to TC risk only in males. Changes in weight and BMI did not have an effect on the risk for TC in either sex (21). Similarly, obesity in early adulthood was significantly associated with TC risk in a case control study in French Polynesia (22). Women who were overweight or obese at age 18 were at a significantly greater risk for TC compared to women with normal weight lifelong (OR 6.2 [CI 2.5–15.5]), and similar trends were observed for males. The longer the time period in the obese state, the higher the TC risk appeared to be. In this study, BMI changes from age 18 were linked to a higher TC risk in women independently of their menopausal status (22). Likewise, in a French cohort of 91,909 middle-aged women, a 5 kg/m2 increase in BMI was associated with a 21% increased risk of TC. The greatest risk was reported in women experiencing an increase in their body shape from lean to large during transition from menarche to adulthood with a HR of 2.17 [CI 1.04–4.53] compared to women who remained lean (23). In a pooled analysis of 12 TC studies, Dal Maso et al. found a direct association of BMI with TC risk in women but not in men. However, no consistent TC risk pattern could be associated with the BMI in early adulthood (24).
BMI status and weight gain in early adult life are likely to play a promoting role in TC and warrant further investigation. It could be hypothesized that there is sexual dimorphism on the effect of BMI and weight gain on TC risk and, if so, estrogens, also derived from peripheral aromatization in the adipose tissue, might be implicated in the underlying process. Despite the lack of data, one could speculate that the increase in circulating estrogens resulting from the peripheral aromatization in the adipose tissue might have a differential action in the two sexes. For example, in females, already producing significant amounts of estrogens, this might more easily exceed a “threshold” of estrogenic load, above which immune responses are possibly altered and mitogenic processes augmented. This effect could be more pronounced during transition to adulthood, a period of significant hormonal changes. Similarly, pre- and postmenopausal women also exhibit a different hormonal profile. Estrogenic deprivation after menopause might alter the response to an obesity-associated rise in circulating estrogens and its potential consequences on thyroid cell differentiation and proliferation.
The role of obesity among different TC subtypes has also been examined. Engeland et al. performed a histopathology-focused analysis showing that the relative risk for follicular and PTC increased with higher BMI values, and this was more prominent in women, whereas there was a trend toward decreased incidence of medullary cancer with higher BMI (17). Additionally, in a large U.S. prospective study, the relative risk for PTC increased with rising BMI values, whereas only a trend was noted for follicular and anaplastic TC and no relation could be demonstrated for medullary TC (20). Clearly, more studies are needed to elucidate the differential effect of obesity in the various TC types. According to the existing literature, obesity appears to be associated with follicular-cell derived well-differentiated thyroid tumors, whereas its effect on tumors of parafolicullar and poorly differentiated cells, if any, is not clear. Of course, this may be due to the fact that these latter tumors are rare and any effect would require larger numbers in order to be shown.
Sedentary lifestyle is considered one of the major contributing factors to obesity. There are inconsistent data on the role of physical activity on TC risk. In the previously mentioned study, Leitzmann et al. found that the level of physical activity was unrelated to TC (20). Strangely, in a pooled analysis of five prospective studies, physical activity was associated with a higher risk for TC. This relation referred only to overweight and obese subjects and was not evident in normal-weight individuals (25). In the opposite direction, in a 15-year follow-up study, there was a trend toward lower risk for TC in women with long-term physical activity compared to their inactive peers (RR 0.77 [CI 0.57–1.04]) (26). Central adiposity was also identified as an independent determinant of higher TC risk, which is more striking in men, whereas TC risk is further increased in the co-existence of central adiposity and obesity (27). It is also possible that not only excess weight but also the source of energy excess influences TC risk. Marcello et al. recently suggested that nutrient intake may play an important role in the link between obesity and TC (28). In their case control study, excess protein and carbohydrate consumption were significantly higher in TC patients compared to controls, whereas no difference was demonstrated in lipid and fiber intake and level of physical activity. When data from two case control studies with a predominantly female population from New Caledonia and French Polynesia were analyzed jointly, body surface area rather than BMI was identified as an independent determinant of TC risk (29). The association of obesity with thyroid carcinogenesis is apparently not straightforward but rather complicated, and there are several metabolic factors to be considered in the obesity–TC connection.
Despite the large body of literature linking overweight and obesity with elevated TC risk, there are some contradictory epidemiological studies showing no significant relation—or even an inverse one—between obesity and TC risk or the presence of thyroid nodules (30 –32). In a recent case control study, Kitahara et al. evaluated 23 obesity-related gene regions in 341 TC cases and 444 control subjects (33). No association could be established between the obesity-related single-nucleotide polymorphisms and TC risk. There are also data even showing the opposite. In a case control study, Cappelli et al. found a lower prevalence of thyroid nodules in morbidly obese women compared to the normal-weight control group (34). In another study performed on 253 subjects with indeterminate thyroid nodule fine-needle aspiration biopsies, obesity was linked to lower malignancy rates in men. This was also shown in women under 45 years old, whereas in older women a positive relation of obesity with thyroid malignancy was present (35). Despite the few studies supporting the opposite, the majority of available literature and of large population studies favors the association of increasing BMI with higher risk of thyroid tumors. A summary of available studies evaluating the link of obesity with TC is presented in Table 1.
TC, thyroid cancer; BMI, body mass index; HR, hazard ratio; CI, 95% confidence interval; OR, odds ratio; FNAB, fine needle aspiration biopsy; PTC, papillary thyroid carcinoma; BSA, body surface area.
Obesity and thyroid cancer profile
Three recent studies have focused on the role of obesity in the clinical and pathological features of PTC. In a retrospective study of 2057 PTC patients, Kim et al. found that higher BMI was related to a more aggressive PTC phenotype, that is, increased tumor size, extrathyroidal invasion, and advanced disease stage, independently of age, sex, and other confounding factors. No relation was found between obesity and recurrence rates (36). Similarly, greater BMI values were linked to a more advanced stage and aggressive histopathologic subtype of PTC in the study of Harari et al. assessing 443 PTC patients (37). These studies are discordant from the findings of Paes et al. (38) who found no association of BMI with stage, vascular invasion, and recurrence of differentiated TC. In fact, the authors reported an inverse relation of BMI with nodal metastasis and tumor invasion that remained statistically significant in the multivariate analyses. One has to consider the retrospective nature of these studies as a limiting factor. Clearly, more studies are needed to clarify the link of adiposity with clinicopathological features of TC and evaluate its possible role as a prognostic factor.
Possible underlying mechanisms
Various hypotheses have been offered to interpret the connection of obesity with TC, including the upregulation of mitogenic pathways in the presence of hyperinsulinemia, low-grade inflammation, and oxidative stress, common denominators of obesity, especially with central fat distribution. A plausible scenario could involve proliferative pathways activated by insulin and IGF-1. TC patients were found to have insulin resistance at a significantly higher rate compared to the control group in the study of Rezzonico et al. (50% vs. 10%, p<0.001). However, the number of cases was very small (39). There is discordance in the current literature on the association of insulin resistance with TC risk (16,40), and there are also epidemiological studies, in which this factor has not been controlled for (17,20,22,23).
Additionally, there are accumulating epidemiological data showing an independent association of TSH levels with obesity even in the absence of hypothyroidism (41), while at the same time TC patients have, as a group, higher TSH levels (42). There is also evidence of a positive association between TSH levels and advanced disease stage (43). One cannot exclude the possibility that the higher TSH levels observed in overweight and obese subjects might have a direct effect in thyroid tumorigenesis. This is supported by in vitro and animal models demonstrating a mitogenic effect of TSH on thyroid follicular cells (44). The TSH receptor mediated increase in intracellular cAMP levels is considered the major stimulus for thyroid cell proliferation. It appears that TSH interacts with other growth factors, such as insulin and IGF-1 (45), and other pathways, including the RAS-BRAF and the PI3 kinase-AKT pathways, are also implicated (46).
Furthermore, there are recent data supporting the notion that adipokines, such as leptin and adiponectin, may be directly implicated. Leptin levels were higher in TC patients compared to healthy subjects in the case control study of Hedayati et al. (47). In the studies of Cheng et al., leptin and its receptor were found to be overexpressed in PTC cells and associated with an aggressive phenotype, that is, larger tumor size and nodal metastasis (48). The same authors also provided evidence that epigenetic effects and stimulation by insulin regulate leptin and leptin receptor expression in PTC (49). In the same line, Uddin et al. demonstrated that leptin acts via its receptor to induce PTC cell proliferation and inhibit apoptosis (50). Leptin was also shown to enhance migration of PTC cells, whereas it inhibited migration of anaplastic and follicular cancer cells (51,52). Concerning adiponectin, an opposite pattern was identified. Although Cheng et al. showed overexpression of its receptors in certain thyroid tumor types, this was linked to a better clinicopathological profile and improved outcomes (53). In a study in humans, Mitsiadis et al. reported an inverse relation of circulating adiponectin levels with TC risk (54). The role of adipokines in the interplay between obesity and TC is an interesting subject of research and should be further explored.
Lastly, the stronger association of obesity with TC in females observed in many studies could point to a direct effect of sex steroids in thyroid carcinogenesis. There are experimental data supporting a mitogenic effect of estrogen in thyroid tumors (55), whereas a pooled analysis of clinical studies suggested a modestly increased risk in women receiving oral contraceptives, gradually decreasing after discontinuation (56). Still, both in vitro and clinical findings concern the effect of exogenous hormones, whereas the role—if any—of endogenous sex steroids has not been well determined. A significant alteration in the balance between estrogens and androgens occurs in women in the menopausal transition, a time period usually accompanied by weight gain and increase of central fat, whereas also in obese men, aromatase activity in the adipose tissue contributes to endogenous estrogen production. Should a causative link between obesity and TC exist, it is most likely multifactorial with a cross-talk between the various pathways. A summary of potential pathophysiologic pathways linking obesity with thyroid tumorigenesis is illustrated in Figure 2.
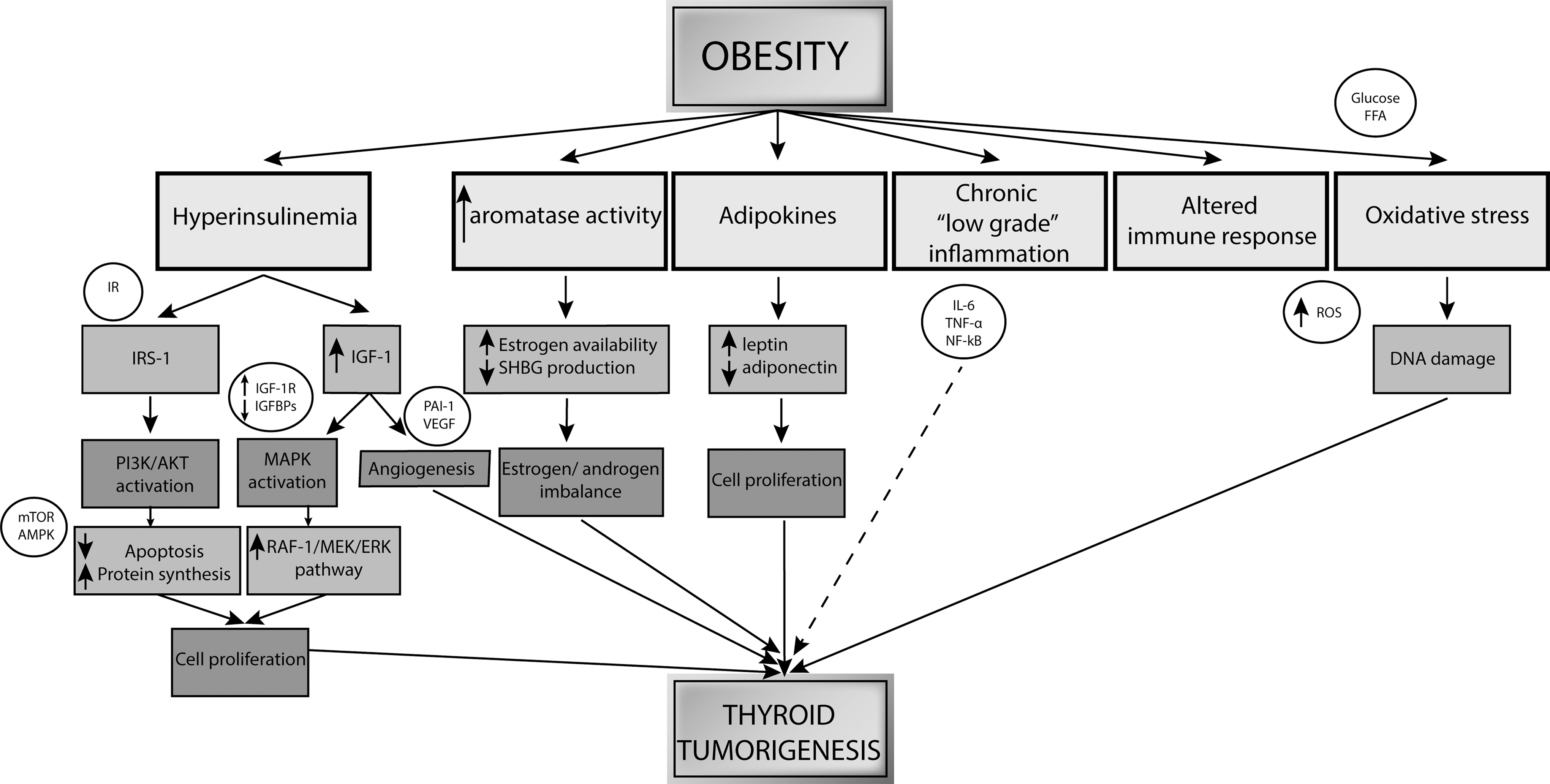
Proposed mechanisms underlying the obesity–thyroid cancer relation. IR, insulin receptor; IRS-1, insulin receptor substrate 1; PI3K, phosphatidylinositide 3-kinase; AKT, protein kinase B; mTOR, mammalian target of rapamycin; AMPK, AMP-activated protein kinase; IGF-1, insulin-like growth factor 1; IGF-1R, IGF-1 receptor; IGFBPs, IGF-1 binding proteins; MAPK, mitogen-activated protein kinase; RAF-1/MEK/ERK, proto-oncogene serine/threonine-protein kinase/MAPK kinase/extracellular-signal-regulated kinase; PAI-1, plasminogen activator inhibitor-1; VEGF, vascular endothelial growth factor; SHBG, sex hormone binding globulin; IL-6, interleukin 6; TNF-α, tumor necrosis factor alpha; NF-κB, nuclear factor kappa-beta; FFA, free fatty acids; ROS, reactive oxygen species.
Caveats
Clearly, there are certain factors that should be considered when trying to interpret studies of TC risk in overweight and obese individuals. It is possible that confounders, such as age, sex, ethnicity, smoking habits, as well as heterogeneity in study size, may explain the lack of uniformity in the reported findings. The different methodology of the studies and the varying BMI should also be taken into account. Obesity is the result of various genetic, metabolic, and environmental factors, and it is therefore very difficult to control independently for each one of these and clarify its possible contribution to the obesity–TC relation. The importance of a statistically significant finding depends on the level of its clinical relevance and the impact it could have on everyday practice. Unless larger prospective studies validate the positive association between obesity and TC and the underlying pathways are untangled, screening for TC in overweight and obese subjects, a rapidly increasing body of the general population, does not seem justified.
Conclusions
In this review, an attempt has been made to summarize clinical data on the relation of obesity with TC. The prevalence of TC is rising, and evidence is beginning to accumulate that obesity is independently related to an increased TC risk. Although there is some discordance in the existing literature, this association might be stronger in the female population. It is also possible that weight changes during early adulthood might play a role in thyroid tumorigenesis. More studies are required to elucidate the role of obesity in the progression and outcome of TC. Increased vigilance for TC among overweight and obese individuals is not justified at the moment. However, the possibility of a causative relation between obesity and TC could increase public awareness. It could potentially function as an additional motive in obesity prevention campaigns in order to pursue a healthier lifestyle and avoid weight gain. Furthermore, if the link between obesity and TC is proven to be causative and strong, a successful public health program decreasing the prevalence of obesity is anticipated to be accompanied by a decrease in TC rates in the long term. Given the development of obesity as an epidemic, it is important to clarify its connection with TC, as well as the contribution of several obesity-related signaling pathways in the pathogenesis of TC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.