
Abstract
Background:
Iodine in iodinated contrast agents (ICAs) interferes with radioactive iodine treatment (RAIT) and diagnostic scans in patients with differentiated thyroid carcinoma (DTC) because it can compete with 131I. Published guidelines recommend delaying RAIT for three to four months in patients who have been exposed to ICA. Spot urinary iodine concentration is a useful marker to reflect the body iodine pool. We investigated the impact of ICAs administered at preoperative computed tomography (CT) scan on the body iodine pool to determine the proper time interval between preoperative CT and RAIT in DTC patients.
Methods:
We performed a retrospective review of 1023 patients with DTC who underwent a preoperative CT scan with ICA, total thyroidectomy, and one week of low-iodine diet in preparation for RAIT. Urine iodine excretion (UIE) was measured in spot urine by inductively coupled plasma mass spectrometry and reported both in simple concentration (μg/L) and divided by gram creatinine (μg/gCr). Patients were divided into five groups by time interval in days between preoperative CT scan and spot urine iodine measurement (A, 31–60 [n=29]; B, 61–90 [n=155]; C, 91–120 [n=546]; D, 121–150 [n=226]; E, 151–180 [n=67]).
Results:
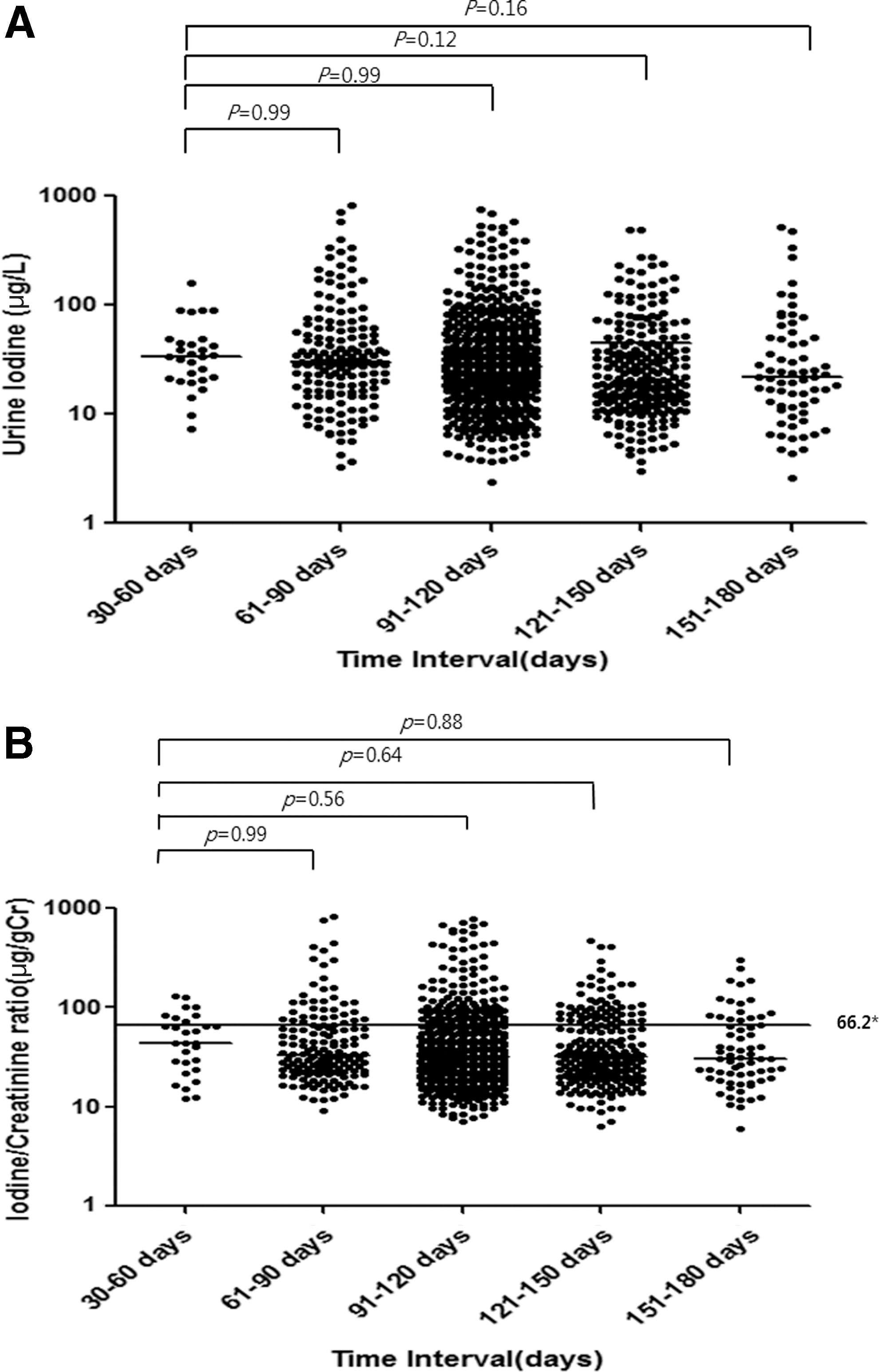
The median (interquartile range) of UIE (μg/gCr) in each group was 44.4 (27.7–73.2) in group A, 33.3 (22.8–64.7) in group B, 32.7 (20.8–63.0) in group C, 32.0 (20.6–67.0) in group D, and 30.4 (19.6–70.8) in group E. There was no significant difference between group A and the remaining groups (p>0.05) Also, the proportion of patients who achieved the appropriate UIE for RAIT according to our hospital's cutoff (≤66.2 μg/gCr) was not different between groups (A, 72.4%; B, 76.1%; C, 77.5%; D, 74.8%; E, 74.6%) (p=0.78).
Conclusion:
This study shows that a UIE of one month after preoperative CT scan with ICA was not higher than that of six months after CT scan in patients who underwent total thyroidectomy for DTC. Thus, current guidelines that recommend delay of RAIT for three to four months after CT scan with ICA should be revisited and future studies to clarify the appropriate time interval between CT scan with ICA and RAIT are warranted.
Introduction
R
Computed tomography (CT) scans are commonly performed with iodinated contrast agents (ICAs) that contain a large amount of organic iodine, which is approximately 450–4200 mg of iodine content in a single injection of ICA (3). Costa et al. suggest that ICA substantially increases total body iodine stores for at least three months, and in some cases for as long as two years (4). If the body iodine pool stays elevated for several months or even years after CT scan with ICA, it might cause problems in postoperative ablation or RAIT in patients with DTC. Therefore, current guidelines recommend delaying RAIT for three to four months in patients who have been exposed to ICA, and emphasize the importance of measurement of a spot urinary iodine level in these patients (5,6). However, the reference data are from patients with an intact thyroid gland, and the exact time interval required for the body iodine pool to return to its baseline has not been well studied in patients who have undergone total thyroidectomy. Recently, Padovani et al. reported that urinary iodine returns to its baseline four weeks after a patient undergoes a CT scan with ICA after total thyroidectomy and they proposed that the time interval could be even shorter (7).
In this study, we investigated the impact of ICA administration in preoperative CT scanning on the body iodine pool in patients with DTC who underwent total thyroidectomy with the aim of determining a sufficient time interval between preoperative CT with ICA and postoperative RAIT or remnant ablation in these patients.
Methods
Patients and study design
We retrospectively reviewed 1023 patients who underwent a preoperative CT scan (neck or chest) with ICA followed by total thyroidectomy, and were tested with spot urine iodine before postoperative remnant ablation or RAIT between January 2009 and March 2012 at Samsung Medical Center, Seoul, Korea. Patients were advised to follow a one-week low-iodine diet (LID) before spot urine sampling because iodine intake is categorized as excessive in Korea according to the World Health Organization. Urinary iodine and creatinine (Cr) were measured in spot urine samples after an eight-hour fasting state. Patients with renal failure and exposure to iodine-rich medications such as amiodarone within four months were excluded.
The preoperative CT was performed within one to six months before urine iodine measurements. All patients received nonionic ICA (Ultravist 300 or Omnipaque 300 or Iomeron 300), which has an iodine concentration of 300 mg/mL during CT scan. The ICA dose ranged from 80 to 100 mL, with an amount of iodine ranging from 24,000 to 30,000 mg per preoperative CT scan. Patients were divided into five groups according to time interval in days between preoperative CT scan and spot urine sampling for iodine measurement. The five groups were as follows: group A, 31–60 days; group B, 61–90 days; group C, 91–120 days; group D, 121–150 days; group E, 151–180 days. This study was approved by the Institutional Review Board at Samsung Medical Center.
Laboratory methods
Urine iodine was measured by inductively coupled plasma mass spectrometry using an Agilent 7500 series instrument (Agilent Technologies, Inc., Tokyo, Japan), which has been demonstrated to provide extremely accurate measurements of urine iodine concentrations (8 –10). The intraday coefficient of variation was 0.3–1.2% and the interday coefficient of variation was 1.4–3.3% for urine iodine measurement. Urine Cr was measured using a Cobas Integra 800 instrument (RocheDiagnostics, Basel, Switzerland). We previously reported that the iodine/creatinine (I/Cr) ratio from spot urine can serve as a useful and reliable alternative to 24-hour urine collection and that the cutoff I/Cr ratio for appropriate LID preparation was <66.2 μg/gCr (11). The estimated glomerular filtration rate (eGFR) was calculated with the abbreviated Modification in Diet and Renal Disease Study equation (12). The equation is as follows: GFR=186× (serum creatinine)−1.154×(age)−0.203, from which the result is multiplied by 0.742 for female patients.
Statistical analysis
The Mann–Whitney test was used to compare the median urine iodine excretion (UIE) of group A versus the UIE of group B, group C, group D, and group E. The UIE was described as the median and interquartile range. The one-way ANOVA test was used for comparison of age between the five groups. The Mantel–Haenszel chi-square test was used for comparison of categorical variables between the five groups. All statistical analyses were performed with PASW 17.0 software, version 9.1.3 (SPSS, Inc., Chicago, IL). A p-value <0.05 was considered significant.
Results
A total of 1023 patients were included in this study. Among them, 1012 patients underwent a neck CT scan and 11 patients underwent a chest CT scan. The mean age was 45.2 years (SD 11.4), and the female-to-male ratio was 3:1 (767 females, 256 males). There were 29 patients in group A, 155 patients in group B, 546 patients in group C, 226 patients in group D, and 67 patients in group E. All patients underwent total thyroidectomy and were diagnosed with papillary thyroid carcinoma on final pathology. The age and sex ratios were not different between groups (Table 1).
Between preoperative CT scan and spot urine iodine measurement after a one-week LID.
The cutoff for this definition is ≤66.2 μg/gCr according to our previous report (11).
Cr, creatinine; CT, computed tomography; LID, low-iodine diet; NS, nonsignificant (group A vs. groups B–E); SD, standard deviation.
Urine iodine concentration according to time interval from ICA administration for CT scan
The median simple urine iodine concentrations of groups A through E were 33.8 μg/L (A), 30.1 μg/L (B), 27.3 μg/L (C), 20.6 μg/L (D), and 21.7 μg/L (E), respectively (Fig. 1A). The median urine I/Cr ratio of each group was 44.4 μg/gCr (A), 33.3 μg/gCr (B), 32.7 μg/gCr (C), 32.0 μg/gCr (D), and 30.4 μg/gCr (E). There were no significant differences in spot UIE (simple iodine concentration and urine I/Cr ratio) between group A and groups B through E (Fig. 1A, B). In addition, the proportion of patients who achieved the proper LID preparation status according to our cutoff (≤66.2 μg/gCr) was not different between groups (A, 72.4%; B, 76.1%; C, 77.5%; D, 74.8%; E, 74.6%) (p=0.78) (Fig. 1B).
Urine iodine concentration according to age and eGFR
When we compared the urine iodine concentration according to age, urine iodine concentration tended to increase with age, but there was no statistical significance between younger age (<30 years old) and older age (>40 years old) groups (Table 2). We also compared the urine iodine concentration according to eGFR. eGFR data were available in 865 patients. There was no significant difference in urine iodine concentration between eGFR groups (Table 3). Although it seems that the urine iodine concentration in the group with an eGFR less than 30 mL/min was higher than that in the remaining groups, it did not reach statistical significance because there were only 4 people in the group with an eGFR less than 30 mL/min.
Comparison of median urine iodine of age groups: age ≤30 vs. other age groups.
Comparison of median urine iodine of eGFR groups: eGFR ≥90 vs. other eGFR groups.
eGFR, estimated glomerular filtration rate; NA, not available.
Discussion
Our findings demonstrate that the urine iodine concentration at one month after preoperative CT scan with ICA is not different from that at six months in patients with DTC who have undergone total thyroidectomy. Since patients need at least four weeks (almost one month) of thyroxine withdrawal to raise the serum TSH after total thyroidectomy, unless recombinant human TSH is used, and considering the recovery time from surgery before radioactive iodine administration, a preoperative CT scan with ICA is not a hurdle for subsequent remnant ablation or RAIT after surgery. When preparing patients for RAIT or a diagnostic scan using radioactive iodine, depleting the inorganic iodine pool is required to enhance radioactive iodine uptake (1,2,13,14). ICAs contain an enormous amount of iodine and thus can interfere with radioactive iodine uptake in remnant thyroid or tumor tissue because it can compete with 131I (15,16). Therefore, there has been concern about the effect of ICA on subsequent remnant ablation or RAIT in patients with DTC. Although the mechanism of reduced radioactive iodine uptake by ICA is not clear, it is believed that free inorganic iodine in the ICA is involved (17). The amount of free iodide is estimated to be between 0.01% and 0.15% of the amount of organically bound iodine administered in ICA (15,17). Consequently, 100 mL of ICA, which has 300 mg of iodine per mL, can provide 3000–45,000 μg of free iodide. The amount of free iodine is about 20–300 times the daily requirement of iodine for adults (150 μg/day) recommended by the World Health Organization.
When exposed to high iodine intake, our body stores iodine in interstitial fluids, in colloid within the thyroid gland and in virtually every organ in the body. Costa et al. reported that giving a patient ICA substantially increases total body iodine stores for at least three months, and in some cases for up to two years (4). Another study by Spate et al. showed that it took a minimum of 3 months for the body iodine level to return to baseline after a single injection of ICA and that the time required to achieve this baseline level in most patients in their study was 6–10 months (18). However, these studies were restricted to patients with an intact thyroid gland.
On the basis of these results, most guidelines focusing on patients with DTC recommend a three- to four-month delay of RAIT in patients who have been exposed to ICA. The American Thyroid Association guidelines recommend that ICA should be avoided if RAIT is planned within the subsequent few months (5). The European consensus guidelines also state that radioactive iodine administration should be postponed for two to three months after the event of iodine contamination (e.g., ICA) (6). Some even recommend that ICA should not be used in patients with DTC before surgery (19).
However, water-soluble nonionic ICAs are currently used for enhanced CT scan and these are quickly eliminated by the kidney rather than by the hepatobiliary system (15). According to a study by Nygaard et al., 131I uptake was moderately reduced to 53.4% at one week after the injection of nonionic ICA, but became normal within approximately three to four weeks (20). The reduced and short inhibition of radioactive iodine uptake by nonionic ICAs might be explained by the rapid clearance compared with old lipid-based ICAs (20). Also, it is well known that biliary contrast media, which circulate longer in the body, result in the release of a significant amount of free iodide in circulation (15).
Recently, Padovani et al. reported that the required period for urine iodine values to return to baseline after ICA exposure was no more than four weeks, which is very similar to the results from our study, even though the patient groups were a little different between the studies (7). They prospectively evaluated 25 patients with DTC who received ICA for enhanced chest or neck CT scan postoperatively, unlike our subjects, who have undergone a CT scan with ICA preoperatively. They measured spot urine iodine levels before performing the CT scan, and at one week and at one, two, and three months after the CT scan with ICA. Even though the urine iodine concentration at one week after ICA was significantly higher than that of baseline, it dropped rapidly to baseline by at least one month after ICA (7). Thus, their results are very similar to our results.
Circulating iodine is cleared from the blood principally by the kidney, and the renal clearance of iodine depends on GFR. Therefore, patients with end-stage renal disease are known to have decreased renal iodine clearance, and an elevated serum iodine concentration (21). We have compared the urine iodine concentration according to different age groups and different eGFR groups. There was a positive trend between urine iodine concentration and age, although there was no statistical significance. This might be associated with (i) decreasing eGFR with age or (ii) the traditional food-intake style among old individuals in Korea, which is rich in sea-related foods, even though they are educated to avoid iodine-containing foods. The urine iodine concentration was not different between eGFR groups. The urine iodine concentration in the group with an eGFR less than 30 mL/min tended to be higher than that in the remaining groups. However, because there were only four subjects in this group, the difference did not reach statistical significance. An eGFR less than 30 mL/min indicates severely reduced kidney function and requires planning for end-stage renal failure (e.g., dialysis). Thus, the results obtained in this study in old patients or a significantly decreased eGFR need to be interpreted with caution.
There are some limitations in our study. First, this study was not a prospective study comparing baseline urine iodine concentration before and after the CT scan with ICA. Therefore, we cannot propose an exact time interval when the urine iodine level returns to baseline. However, our data suggest that the time required for UIE to return to its baseline after the CT scan with ICA is one month and possibly earlier. Second, about one-fourth of patients did not achieve the hospital cutoff for appropriate iodine restriction status for RAIT even though they were instructed to follow an LID. The cause of failure to achieve appropriate preparation of LID was not studied in this retrospective analysis, but we suspect that noncompliance would be the main cause of failure with LID, especially in areas where iodine intake in food is excessive. Third, the number of subjects in group A (n=29) and the number of subjects in group E (n=67) were relatively small because of the limits associated with the retrospective study design, and it might affect the statistical findings. However, the Mann–Whitney test is believed to be a reliable statistical method even if the sample size is small in the comparison of nonnormally distributed variables. Further clarification by a prospective design would be helpful. Fourth, this study was done in Korea, where the iodine intake is considered high. However, we can deduct a hypothesis from previous results. (i) A one-week LID is sufficient to reach the target iodine concentration even in an iodine-rich area (22). On the contrary, an LID is not strictly recommended in iodine-deficient areas during preparation for RAIT (23). (ii) Prior ICA use one month or earlier does not affect the urine iodine concentration in an iodine-rich area (this study). (iii) Recent published data by Padovani et al. from Brazil, where iodine is relatively deficient and the government implements that all the salt for human consumption should be iodized, showed that four weeks is enough for urine iodine to return to its baseline in postthyroidectomy patients studied in prospective protocol (7). Considering these three facts, we may deduce that the urine iodine concentration after prior ICA administration one month or earlier will show the same results in iodine-deficient areas. However, before applying these study findings to iodine-deficient areas, we need to verify the results with further analyses.
In conclusion, we found that UIE at one month after a preoperative CT scan with ICA was not higher than that after six months in patients who underwent total thyroidectomy for DTC. Thus, current guidelines that recommend a three- to four-month delay of RAIT after CT scan with ICA should be revisited and future studies to clarify the appropriate time interval between CT scan with ICA and RAIT are warranted.
Author Disclosure Statement
The authors have nothing to declare.