
Abstract
Background:
HLA-G is a nonclassical major histocompatibility complex molecule that has well-recognized immunomodulatory properties. The expression of HLA-G in tumor cells has been considered to be detrimental, permitting tumor spreading and decreased survival. We evaluated the expression of HLA-G in histologically normal thyroid tissue, goiter, and benign and malignant thyroid tumors, and studied the relationship between HLA-G expression and patient clinical variables.
Patients and Methods:
The immunohistochemistry expression of HLA-G was performed on 72 specimens of papillary thyroid carcinoma (PTC), 19 follicular thyroid carcinomas (FTC), 22 follicular adenomas (FA), 22 colloid goiters (CG), and 14 histologically normal thyroid glands (NT). The percentage of HLA-G staining was graded from absent (−) to intense (+++).
Results:
HLA-G was faintly expressed in areas of hyperplasia in NT and CG. In PTC, FTC, and FA, the percentage of cell staining was significantly higher than in NT and CG (p<0.001 for each comparison). The tumor area with HLA-G expression was greater in FTC (p=0.0059) and PTC (p=0.0330) compared to FA. According to the magnitude of HLA-G staining, PTC tumors >1 cm exhibited increased HLA-G staining when compared to smaller tumors (p=0.03). Aggressive histologic subtypes of PTC have a higher median stained tumor area. No association was found between HLA-G expression and tumoral staging or patient disease-free survival.
Conclusions:
The gradual increase of HLA-G expression from hyperplasia to carcinomas, and the association of strong HLA staining with some variables implicated in poor prognosis corroborate the unfavorable role of HLA-G in tumor thyroid cells, inhibiting cytotoxic immune system cells and facilitating tumor evasion and progression.
Introduction
T
Malignant thyroid tumors have a variable clinical presentation. Some progress with slow growth, without interfering with life expectancy, while others progress rapidly, leading to death within a short time. Papillary thyroid carcinomas (PTC) and follicular thyroid carcinomas (FTC) are classified as differentiated tumors, represent 90% of the cases, and are derived from follicular cells. Anaplastic carcinomas (AC) are undifferentiated ones and correspond to <5% of the cases (4). Nowadays, clinical and pathological staging is most commonly used to determine the prognosis of thyroid cancer. However, patients with similar stages may experience different outcomes. The identification of prognostic tumor markers could help in therapeutic decisions and in the development of effective treatments.
The immune response plays an important role in tumorigenesis, and the human leukocyte antigen G (HLA-G) plays a well-recognized role in the modulation of the immune response against tumor cells (5). The aberrant HLA-G expression in tumors has been proposed to be an additional tumor cell strategy to evade host immune response.
HLA-G is a nonclassical class I antigen of low polymorphism and restricted tissue distribution, being constitutively expressed in thymus cells, the maternal–fetal interface on cytotrophoblast cells, the pancreas, and in chorionic and corneal tissues (6,7). The HLA-G gene exhibits several alternative splicing products, including membrane-bound (HLAG-1, HLA-G2, HLA-G3, HLA-G4) and soluble isoforms (HLAG-5, HLA-G6, HLA-G7) (8,9). HLA-G has been extensively studied in many pathological conditions such as tumors (10), autoimmune diseases (11), organ transplantation (12), and viral infections (13). HLA-G expression in tumors has been identified in trophoblastic neoplasia; melanoma; colon, renal, lung, ovarian, breast, and endometrium carcinomas; glioblastoma; cutaneous lymphoma; leukemia; and others (14). In the context of tumor biology, higher in situ HLA-G expression has been observed in more than 20 types of tumors, and it was preferentially detected in tumor tissue and rarely in the adjacent normal tissue, suggesting its specific association with tumor growth and progression (15).
HLA-G has been implicated in antitumor immune responses by inhibiting natural killer (NK) and antigen-specific CD8+ T-cell cytotoxicity through interaction with ILT-2 and ILT-4 leukocyte receptors, primarily when HLA-G dimers are formed in situ (16). In addition, HLA-G induces apoptosis of activated CD8+ T lymphocytes (17), suppresses CD4+ T-cell proliferation in response to allogeneic stimulation, and promotes T helper2 cytokine polarization (18,19).
Detection of HLA-G in tumor tissue has been correlated with clinical and pathological variables in lymphoma; melanoma; and breast, ovarian, endometrial, lung, esophagus, colon, and bladder carcinoma. Evidence indicates that HLA-G can serve as a diagnostic and prognostic tumor marker (20). Data available about the presence of HLA-G in thyroid disease are scant. Therefore, we performed a study to identify the presence of HLA-G molecule in the normal and the neoplastic gland, comparing the semi-quantitative HLA-G expression and correlating these findings with patient clinical outcomes.
Patients and Methods
Patients
The Institutional Ethics Committee for human research of the University Hospital, School of Medicine of Ribeirão Preto—University of São Paulo, Brazil approved this study, and informed consent was obtained from all subjects (protocol # 10938/2009).
We studied 138 patients with malignant and benign thyroid diseases who underwent tyroidectomy from 2000 to 2011, and who were followed up at the Thyroid Outpatient Clinic of the Division of Endocrinology of the School of Medicine of Ribeirão Preto. We selected patients whose thyroid specimens were collected during surgery and filed in a tumor database of the Division of Endocrinology. Histopathological analyses revealed 72 papillary thyroid carcinomas (PTC), 19 follicular thyroid carcinomas (FTC), 3 anaplastic carcinomas (AC), 22 follicular adenomas (FA), and 22 colloid goiters (CG). An additional 14 thyroid tissues obtained from deceased individuals without known thyroid diseases and exhibiting no macroscopic or histological abnormalities were studied. Demographic and clinical features of patients and tumor characteristics are shown in Table 1. The median follow-up time for patients with benign or malignant lesions was 4, 4, 5, and 5.25 years for PTC, FTC, FA, and CG groups respectively.
CG, colloid goiter; FA, follicular adenoma; PTC, papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; AC, anaplastic carcinoma.
Immunohistochemical analysis of HLA-G in PTC, FTC, AC, FA, CG, and normal thyroid tissues
Four-micrometer-thick sections of paraffin-embedded tissue blocks were cut and mounted on polylysine-coated slides. Tissues sections were dewaxed in xylene and rehydrated in graded series of ethanol. Antigen retrieval treatment was performed at 95°C for 40 minutes in 10 mmol/L sodium citrate buffer (pH 6.0; Synth, Diadema, Brazil). The endogenous peroxidase activity was blocked treating the slides with two consecutive baths of 3% hydrogen peroxide in methanol. To block nonspecific reactions, tissue sections were washed three times (5 minutes each) in phosphate buffered saline (PBS) 0.01 M (pH 7.2), and incubated in PBS enriched with 1% nonfat milk. Samples were incubated overnight with the primary monoclonal antibody 5A6G7 anti-HLA-G antibody (EXBIO Antibodies, Vestec, Czech Republic). We selected the 5A6G7 antibody after performing a randomized pilot study testing two types of anti-HLA-G monoclonal antibodies (4H84 and 5A6G7) in thyroid specimens. The 4H84 mAb recognizes the free heavy chain of all the HLA-G isoforms. The 5A6G7 mAb recognizes the encoded intron part of the soluble HLA-G5/-G6 proteins and reacts with the major soluble HLA-G monomers and dimers, frequently observed in tumor cells (16). No discordant results were found in this pilot study. In addition, in a previous study of our group, evaluating the HLA-G staining in liver specimens that were positive or negative for hepatitis B virus infection, Souto et al. performed all analyses with 5A6G7 and 4H84 antibodies, observing no distinct liver-staining patterns (21).
After incubation with the primary antibody, the slides were treated with streptavidin complex Ultra–Biotin–Peroxidase (EP-USA/500; Signet, Belmont, CA) for 40 minutes at 37°C. Finally, the sections were revealed with diaminobenzidine solution (Sigma, Saint Louis, MO) at 37°C for 10 minutes, and counterstained with hematoxylin for 60 seconds, washed with water, dehydrated, and mounted.
Cytotrophoblast from first-trimester human placenta was used as an HLA-G–positive control. A negative control was performed omitting the primary antibody.
Two experienced pathologists blindly analyzed, under a light microscope, all specimens encompassing the entire thyroid sample at different moments. According to the percentage of stained tumor cells, HLA-G immunoreactivity was stratified into four categories: (i) tissue specimens without staining (–); (ii) mild expression, tissue specimens with <25% of cell staining (+); (iii) moderate expression, tissue specimens presenting 25–50% of cell staining (++); and (iv) strong expression, tissue specimens exhibiting >50% of cell staining (+++).
Statistical analyses
The results were expressed as mean with standard deviation (SD) and median with range. Association between the degree of staining and the various thyroid diseases studied were calculated using the chi-square test or the exact chi-square test, as indicated. HLA-G staining was compared between groups and with clinical variables using the nonparametric Mann–Whitney U-test or the Kruskal–Wallis test, followed by Dunn's post-test. The Kaplan–Meier method was used to estimate the survival rate as a function of time. Survival differences among the immunostaining categories were evaluated using the log-rank test. Patients with AC were not included in statistics due the small number of cases.
All analyses were performed with IBM SPSS software (Statistical Package for the Social Sciences, IBM Corp., Armonk, NY) version 17.0. A 5% level of significance (α=0.05) was considered for rejection of the null hypothesis.
Results
HLA-G expression in thyroid tissues
The immunohistochemical HLA-G expression, when present, was visualized as a brown-stained product primarily observed in the cytoplasm of follicular cells.
HLA-G staining was not observed in normal thyroid samples (Fig. 1A). However, a faint expression was observed in small hyperplasic areas (14.3% of cases). In biopsies of patients with colloid goiter, the majority exhibited no HLA-G expression (60%), and the remaining presented only mild expression in the hyperplasic follicular areas (Fig. 1B). No difference was observed between normal thyroid follicular cells and colloid goiter cells (p=0.1798). All thyroid tumors (benign or malignant) exhibited some degree of HLA-G expression (Fig. 1C, D, and E), which was significantly increased compared to nonaffected thyroid tissue and colloid goiter (p<0.0001 for all comparisons; Table 2). In non-neoplastic areas surrounding thyroid tumors—that is, nonaffected areas—no HLA-G staining was observed. The median stained HLA-G tumor area was 77.5% for PTC, 90% for FTC, 67.5% for FA, and 20% for CG. Among PTC specimens, 3% presented mild, 17% moderate, and 80% strong HLA-G expression. In FTC, 5% had mild and 95% moderate to intense HLA-G staining. Regarding FAs, we observed mild HLA-G staining in 13%, moderate in 32%, and intense expression in 55% of the cases.
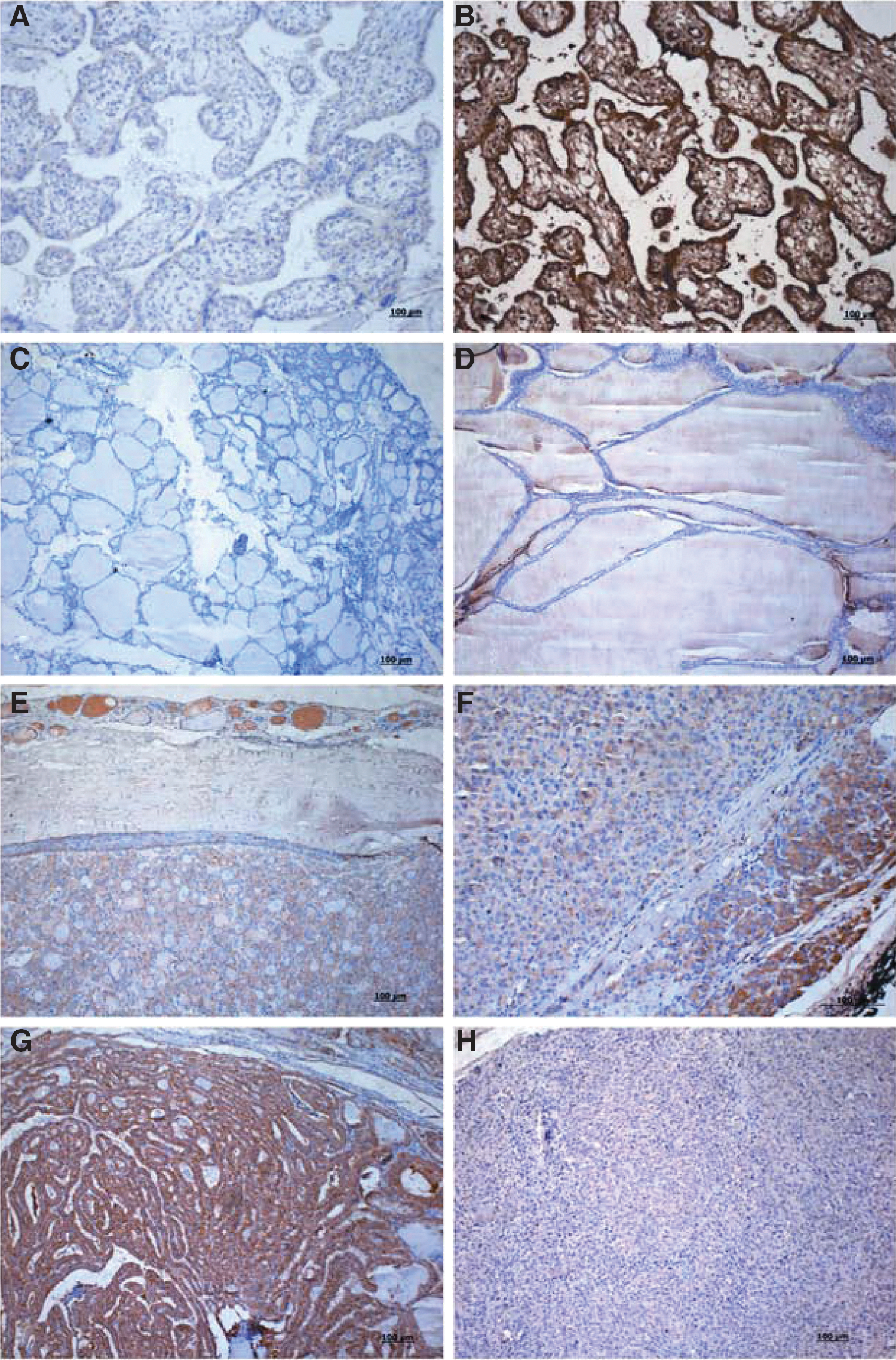
Immunostaining for HLA-G (shown in brown). Negative control: cytotrophoblast tissue was performed omitting the primary antibody
Comparison of the percentage of cell staining from PTC×FTC revealed p=0.0274, PTC×FA revealed p=0.0330, and FTC×FA revealed p=0.0059.
p-Value compares normal thyroid to CG, FA, PTC, and FTC separately (p<0.0001).
p-Value compares CG to FA, PTC, and FTC separately (p<0.0001).
NT, normal thyroid; −, tissue specimens without staining; +, mild expression, tissue specimens with <25% of cell staining; ++, moderate expression, tissue specimens presenting 25–50% of cell staining; +++, strong expression, tissue specimens exhibiting >50% of cell staining.
Concerning the percentage of HLA-G cell staining, FTC showed higher expression compared to PTC (p=0.0274) and FA (p=0.0059), and PTC showed higher expression compared to FA (p=0.0330).
Associations between HLA-G expression and clinical variables in papillary thyroid cancer
To verify the influence of HLA-G expression in thyroid cancer, we associated HLA-G staining with clinicopathological features such as age, sex, tumor size, histological subtype, local invasion, tumor multicentricity, metastasis at diagnosis, stage of the disease, and clinical outcome. Significant associations were primarily observed for the PTC group, and no association was found for FTC. In PTC, the percentage of tumor cells exhibiting strong HLA-G staining (+++) was higher in patients with tumor size >1.0 cm when compared to lesions <1 cm (p=0.03). We observed no significant association regarding age (p=0.67), sex (p=1.00), tumor multicentricity (p=0.10), local invasion (p=0.44), metastasis at diagnosis (p=0.12), and clinicopathological staging (p=0.50). Regarding PTC variants, the classical subtype exhibited median tumor HLA-G staining (80%) similar to the follicular variant (70%), whereas the trabecular, tall-cell, and diffuse sclerosing subtypes (95%) exhibited increased staining when compared to classical (p=0.006) and follicular variants (p=0.006).
The median tumor area with HLA-G expression tended to be greater in patients with disease recurrence or death (87.5%) compared to patients without signs of tumor relapse (75%; p=0.09). Disease recurrence was considered when local disease was documented or elevated serum thyroglobulin was detected in the follow-up. No significant difference was observed in the follow-up time of patients with or without PTC recurrences (p=0.4317). Patients older than 45 years seemed to present with higher HLA-G expression, exhibiting larger tumor areas with HLA-G staining (p=0.09), as shown in Table 3.
p-Value compares tumor size <1 cm to lesions >1 cm.
Others refer to trabecular, tall-cell, and diffuse sclerosing subtypes.
p-Value compares histological subtype other to classical and follicular variants.
Staging: At presentation or time of initial diagnosis for all patients. According to American Joint Committee on Cancer/TNM (tumor, node metastasis, distant metastasis) for differentiated thyroid carcinoma. AJCC Cancer Staging Manual, sixth edition. American Joint Committee on Cancer (
Recurrence: Evidence of local recurrence or functional relapse with elevated thyroglobulin.
To estimate the influence of the HLA-G tumor expression on patient disease-free survival, we constructed survival curves using the Kaplan–Meier method and applied the log-rank test to compare the variable degree of HLA-G expression among PTC patients. We considered death or signs of recurrence (elevated serum thyroglobulin or local relapse) as censored data. We grouped + and ++ HLA-G staining and compared it to +++. No difference in disease-free survival was found among PTC patients with recurrences when compared to patients without recurrences (χ2=1.28; p=0.2565; Fig. 2).
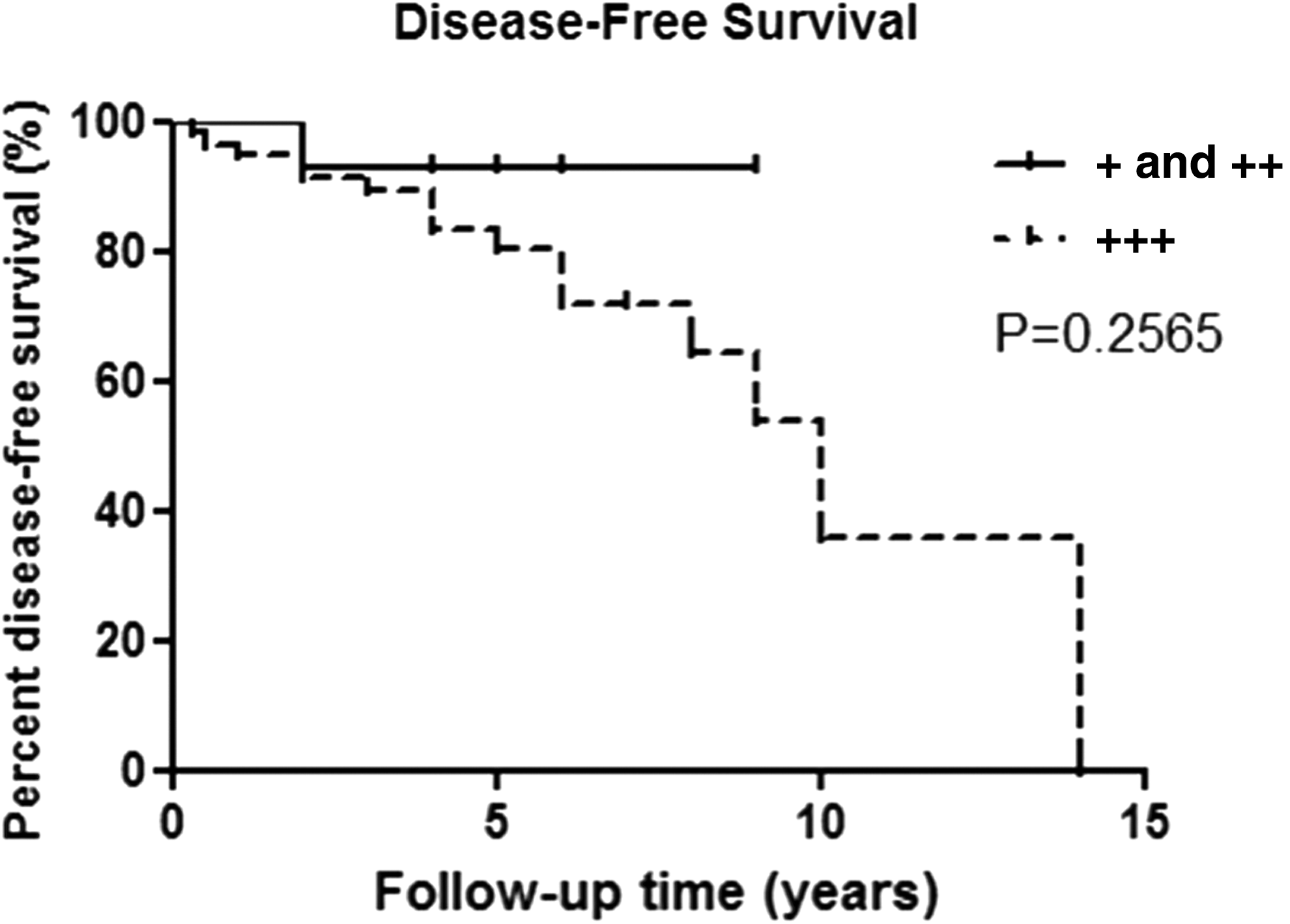
Disease-free survival curve for patients with papillary thyroid cancer. Patients with + and ++ HLA-G staining were grouped and compared to +++ HLA-G staining.
Discussion
Recent advances in cancer are increasingly being applied to the study of clinical samples in the search for diagnostic biomarkers and therapeutic targets. We demonstrate that HLA-G is differently expressed in thyroid tumors.
Scarce information is available about the behavior of HLA-G expression in thyroid tissue. A previous study evaluating autoimmune thyroid disease revealed that HLA-G is not expressed in either thyrocytes or thyroid tissue (22). On the other hand, Dardano et al. showed significantly higher plasma soluble HLA-G (sHLA-G) levels in PTC patients or Hashimoto's thyroiditis when compared to healthy individuals (23). Moreover, no differences in the frequencies of the 14bp insertion/deletion polymorphism were observed between the studied groups (23). In cancer, the relationship between plasma levels and tumor expression has not been established, and may depend on several factors, including the presence or absence of metastasis, the amount of systemic and soluble factors that modulate the expression of HLA-G, and the genetic background of the individuals. Nunes et al. (24), using the MEM-G/2 anti-HLA-G antibody that recognizes a peptide in the alpha 1 domain common to all isoforms, reported HLA-G expression in 44% of the PTC cases, for which the HLA-G expression was correlated with higher frequency of lymph-node metastasis. However, the expression of HLA-G in distinct types of benign and malignant thyroid tumors is poorly known.
The present study explored the HLA-G expression profile in a spectrum of thyroid disorders, reporting that the expression of HLA-G is preferentially observed in neoplastic thyroid tissues, and only mildly expressed in hyperplastic areas of goiter and normal thyroid tissues. We utilized the 5A6G7 anti-HLA-G antibody that recognizes the encoded intron part of the soluble HLA-G5/-G6 proteins and can better detect multimeric forms of HLA-G, which are more effective to interact with the ILT-2 and ILT-4 receptors, inhibiting the activity of cytotoxic T and NK lymphocytes, and are overexpressed in tumors (16).
Since the first description of HLA-G expression, its association with malignant lesions has been intensively studied. The data available so far have shown that the vast majority of tumors may express varying degrees of HLA-G isoforms, reflecting a potential immune escape mechanism. It is also worth mentioning that HLA-G expression is highly dependent on tumor microenvironment factors, particular when IL-10 and hypoxic factor are present (25,26).
HLA-G has been detected in tumor biopsies mainly by immunohistochemistry, and the expression may vary considerably among different studies and types of neoplasms due to the criteria of patient selection and methodology used (27). Since the first study reporting HLA-G expression in melanoma cells (10), several articles have demonstrated the presence of this molecule in gynecological neoplasm (choriocarcinoma, breast, endometrial, and ovarian cancers) (28,29), digestive tumors (colorectal (30), esophageal squamous cell (31), gastric carcinoma (32)), hematological malignancies such as cutaneous lymphoma, leukemia, non-Hodgkin and Hodgkin lymphomas, and multiple myeloma (27), in bladder transitional cell carcinoma (33), renal carcinoma specimens (34), and others.
In a recent review, González et al. reinforce that the high proportion of tumors expressing HLA-G contrasts with its absence in healthy tissue, suggesting that HLA-G upregulation is associated with malignant transformation (27). HLA-G may be detected in both tumor cells and immune system cells that infiltrate the neoplasm (27). Moreover, the phenomenon of trogocytosis, the transference of HLA-G from membranes of positive cells to nonexpressing cells, rendering them capable to induce immune suppression, may also occur (35). Altogether, these events may explain the high association of HLA-G with unfavorable outcomes in several malignancies.
This study demonstrates that HLA-G expression is primarily absent in histologically normal thyroid gland, and when present, it is faintly observed in areas of hyperplasia. In non-neoplastic lesions such as colloid nodular goiters, HLA-G expression is mildly observed in hyperplastic areas. Similarly, in non-neoplastic areas around thyroid tumors, we did not observe HLA-G staining, supporting the idea that the expression of HLA-G may be associated with neoplastic transformation (27). In contrast, we observed HLA-G expression in all thyroid neoplasm, varying from mild to intense staining. Overall, malignant lesions (PTC and FTC) overexpressed monomers and dimers of HLA-G in relation to nonmalignant lesions (FA). These findings suggest a progressively increased expression of HLA-G in follicular cells, starting from hyperplastic areas, passing through nonmalignant lesions and reaching larger areas in malignant lesions. Whether HLA-G participates in follicular cell proliferation, or follicular cell proliferation participates in thyroid cell transformation, are questions that have not yet been clarified. Since there are no markers to differentiate adenomas from follicular carcinomas, the identification of specific markers would be very helpful, and further studies encompassing larger series may answer the above-mentioned questions.
Additionally, in the three cases of AC included in this study, we also observed strong HLA-G expression with a median neoplastic cells staining of 80%. The diverse results obtained with these several types of neoplasm may reflect differences in tumor biology and in the representativity of the samples analyzed. The regulation of HLA-G expression may vary among different tumor types and can be influenced by tumor microenvironment.
Several reports indicate the presence of immune-inflammatory cell infiltrates (macrophages, immature dendritic cells, and mast cells) in thyroid cancer, and these cells may play a critical role in the regulation of carcinogenesis and carcinoma progression (36). The oncogenes in differentiated thyroid carcinomas (RET/PTC, RAS, and BRAF) activate the MAPK cascade inducing the expression of hypoxic factors, particularly hypoxic-inducible factor 1α (HIF-1α) (37). In addition, these oncogenes induce a pro-inflammatory response, recruiting innate immunity suppressive inflammatory cells (CD11b+ and Gr1+) (37), secrete immunosuppressive cytokines (IL-4, IL-10, IL8, IFN, IL6, and VEGF), chemokines, and chemokine receptors (38 –41). Considering that: (i) increased levels of IL-10, IFN-α, and HIF-1α are reported in PTC; (ii) increased levels of these mediators have been associated with survival and growth of thyroid cancer cells (36 –41); and (iii) these mediators are classically reported to be HLA-G inducers (25,26), this inflammatory milieu may contribute to the increased HLA-G expression in thyroid tumors. At the same time, the inflammatory response induces HLA-G expression, and it may be harmful to the host, impairing tumor immune response and facilitating tumoral spreading. Whether other mechanisms of immune evasion are also operating in thyroid cancer requires further study.
The relationship between HLA-G expression and tumor morbidity has also been investigated. Overall, evidence suggests that the more advanced the stage of the tumor, the more frequent the HLA-G expression. In a study of colorectal cancer, HLA-G expression was significantly correlated with depth of invasion, histological grade, decreased host immune response, increased lymph-node metastasis, and more severe clinical and pathological stages, implicating HLA-G as an independent prognostic factor (30). Similar results have been reported for esophageal squamous cell carcinoma (31). However, the expression of HLA-G in bladder transitional cell carcinoma has not been associated with tumor morbidity (33). Therefore, clinical relevance of HLA-G expression in tumors may vary among the different types of malignancies.
Regarding thyroid tumors, this study revealed interesting associations concerning the magnitude of HLA-G staining, particularly for PTC, which was the larger group. The tumor size was associated with increased HLA-G expression. Lesions <1 cm showed smaller staining areas and decreased expression. Trabecular, tall-cell, and diffuse sclerosing PTC subtypes presented larger areas of HLA-G staining. Indeed, these histological variants have been considered to be associated with less favorable outcomes (42), corroborating the idea the HLA-G expression in thyroid tumors may be detrimental to the host. HLA-G expression tended to be more intense in older patients (>45 years). Another interesting finding was that patients with disease recurrence tended to present higher HLA-G expression. Indeed, PTC recurrence, older patients, tumor size, and more aggressive histological variants have been associated with worse prognosis (43).
On the other hand, we observed no association between HLA-G expression and patient disease-free survival during a median follow-up time of four years. It is important to emphasize that despite the worldwide increased incidence of PTC, mortality has remained stable (4); that is, the 10-year survival is about 76–93%, and only 10% of patients manifest tumor persistence or recurrence, depending on their disease stage after initial therapy (44). In addition, most patients with differentiated thyroid carcinoma have a good prognosis when properly treated, exhibiting a rate of mortality that is similar to that reported for the general population.
The sample size and short follow-up time may represent possible limitations of our study. Additional analysis of the HLA-G gene polymorphism could contribute to the knowledge concerning its participation in thyroid carcinogenesis. In conclusion, our findings show for the first time that HLA-G protein expression exhibits a gradual spectrum according to thyroid disease severity, varying from weak expression in hyperplastic areas to mild expression in benign lesions and to a higher expression in malignant thyroid cancers. Risk factors associated with worse prognosis, including tumor size and PTC histological subtypes, were also associated with increased HLA-G expression. Overall, these data corroborate the detrimental role of HLA-G expression in thyroid cancers.
Footnotes
Acknowledgments
We thank Ana Maria Rocha and Denise Faria Galano (Department of Pathology, School of Medicine of Ribeirão Preto, University of São Paulo, Brazil) for slide preparation and Tarsia Giabardo (Department of Clinical Analysis, School of Pharmaceutical Sciences, UNESP, University of São Paulo State, Brazil) for her participation in immunohistochemistry methodology. This work was supported by Fapesp (protocol # 10/51649-9).
Author Disclosure Statement
The authors have nothing to disclose.