
Abstract
Background:
The incidence of thyroid cancer has increased at an alarming rate in both men and women in the United States. The etiology of this epidemic is unclear. We tested the hypothesis that a significant component of this epidemic is due to increased detection of occult disease. We examined whether the density of endocrinologists and general surgeons as well as employment of cervical ultrasonography were factors associated with this epidemic.
Methods:
Thyroid cancer incidence rates by states were obtained from the United States Cancer Statistics 1999–2009 reported by the National Program of Cancer Registries. The densities of endocrinologists and general surgeons and the employment of cervical ultrasonography were calculated on a statewide basis and correlated with the incidence of thyroid cancer.
Results:
Age-standardized incidence rates of thyroid cancer have increased in every state in the United States. Significant regional variations were noted, with the highest incidence rates in the northeast and the lowest in the south. The incidence rates were significantly correlated with the density of endocrinologists (r=0.58, p<0.0001 for males; r=0.44, p=0.0031 for females) and the employment of cervical ultrasonography (r=0.40, p=0.0091 for males; r=0.36, p=0.0197 for females). Both the density of endocrinologists and general surgeons and employment of cervical ultrasonography could explain 57% of the variability in state-level incidence for males and 49% for females.
Conclusions:
These data offer evidence to suggest that the epidemic of thyroid cancer is due to increased detection of a reservoir of previously occult disease. The increased detection of thyroid cancer results in therapeutic interventions including surgery and radioactive thyroid treatment that may be of limited benefit.
Introduction
O
It has been suggested that the increasing incidence of thyroid cancer in the United States was predominantly due to the increased detection of subclinical disease, not an increase in the true occurrence of thyroid cancer, because the vast majority of cases were small tumors and the mortality of the disease remained stable (2). A recent ecologic study using the Surveillance, Epidemiology and End Results (SEER) data indicated that higher levels of healthcare access are associated with higher papillary thyroid cancer rates, which provided supportive evidence for the overdiagnosis of thyroid cancer (3). However, other studies offered divergent opinions (4,5). The study based on the Department of Defense's Automated Central Tumor Registry found that the age-adjusted incidence rate of thyroid cancer in the military was significantly higher than the general population, and the rates varied by military service branch, suggesting that heightened medical surveillance does not appear to explain the temporal increase in thyroid cancer incidence fully (4). Nonetheless, the results of this study are consistent with overdiagnosis.
To examine further the hypothesis ascribing that the epidemic of thyroid cancer is due to increased detection, we analyzed data from the United States Cancer Statistics 1999–2009 to study the incidence variation across the United States and to ascertain whether the variation could be explained by the density of endocrinologists or general surgeons and employment of cervical ultrasonography in a given region.
Materials and Methods
To examine the secular trends and variation in the incidence of thyroid cancer statewide, age-standardized incidence rates and confidence intervals (CIs) were obtained from the United States Cancer Statistics (USCS) from 1999–2009, as reported by the National Program of Cancer Registries (NPCR) (6). All rates were age adjusted to the 2000 U.S. population. The number of endocrinologists and general surgeons in each state was obtained from the LifeScript Doctor Review (7). The LifeScript Doctor Review includes more than 720,000 doctors nationwide, which represents about 75% of the total number of U.S. doctors. The densities of endocrinologists, general surgeons, and primary care physicians by state were calculated as the number of members per 100,000 population in each state. Data on neck ultrasonography came from the retrospective administrative patient claims data affiliated with OptumInsight (8). OptumInsight includes data from United Health Group (UHG) and non-UHG plans, and the individuals covered by these health plans (approximately 32 million annual lives in 2010) are geographically diverse across the United States. The plans provide fully insured coverage for professional (e.g., physician), facility (e.g., hospital), and outpatient prescription medication services. The frequencies of neck ultrasonography in 2000–2011 were expressed as the counts of neck ultrasonography per 100,000 insured individuals for each state. This was a retrospective cohort analysis, and no identifiable protected health information was extracted or accessed during the course of the study. The study protocols are compliant with the Health Insurance Portability and Accountability Act (HIPAA).
States (n=37) that had incidence data for the entire time period 1999–2009 were included for trend analysis. Trends in age-adjusted incidence rates were examined for males and females combined and separately. The annual percentage change in thyroid cancer rates between 1999 and 2009 was calculated for each state to show the relative change in incidence for overall population and male and female separately. Incidence rates of thyroid cancer for the states (n=43) that have populations of more than one million were presented for the time period 2005–2009. Pearson correlation was used to assess the linear correlation between thyroid cancer incidence rates and the densities of endocrinologists, general surgeons, and primary care physicians, as well as the frequencies of neck ultrasonography and thyroid biopsy. Overall strength of the association was determined by a generalized least-squares regression model weighted by state population through calculating the overall R 2 of the model. Median household income by state in 2011 inflation-adjusted dollars, obtained from the U.S. Census Bureau population survey annual social and economic supplements (9), was also included in the final model. Statistical analysis was performed using SAS software (v9.3, SAS Institute Inc., Cary, NC).
Results
Thyroid cancer incidence rates in the United States are depicted in Table 1 and Figure 1 for both sexes combined and separately on a statewide basis (6). The greatest annual increase of age-adjusted incidence rate of thyroid cancer from 1999 to 2009 was 20.6% for females and 16.5% for males respectively. Although there was an increased incidence in every state, the pattern is neither random nor uniform. To analyze regional variations, thyroid cancer incidence rates between 2005 and 2009 are presented in Figure 2. The range was 2.5 times comparing the lowest incidence state (Arkansas) to the highest (Massachusetts) in females, and 2.1 times comparing the lowest (South Carolina) to the highest (Massachusetts) in males. The pattern for both sexes demonstrated that in the northeast the incidence was highest, whereas in the south the lowest incidence was observed.
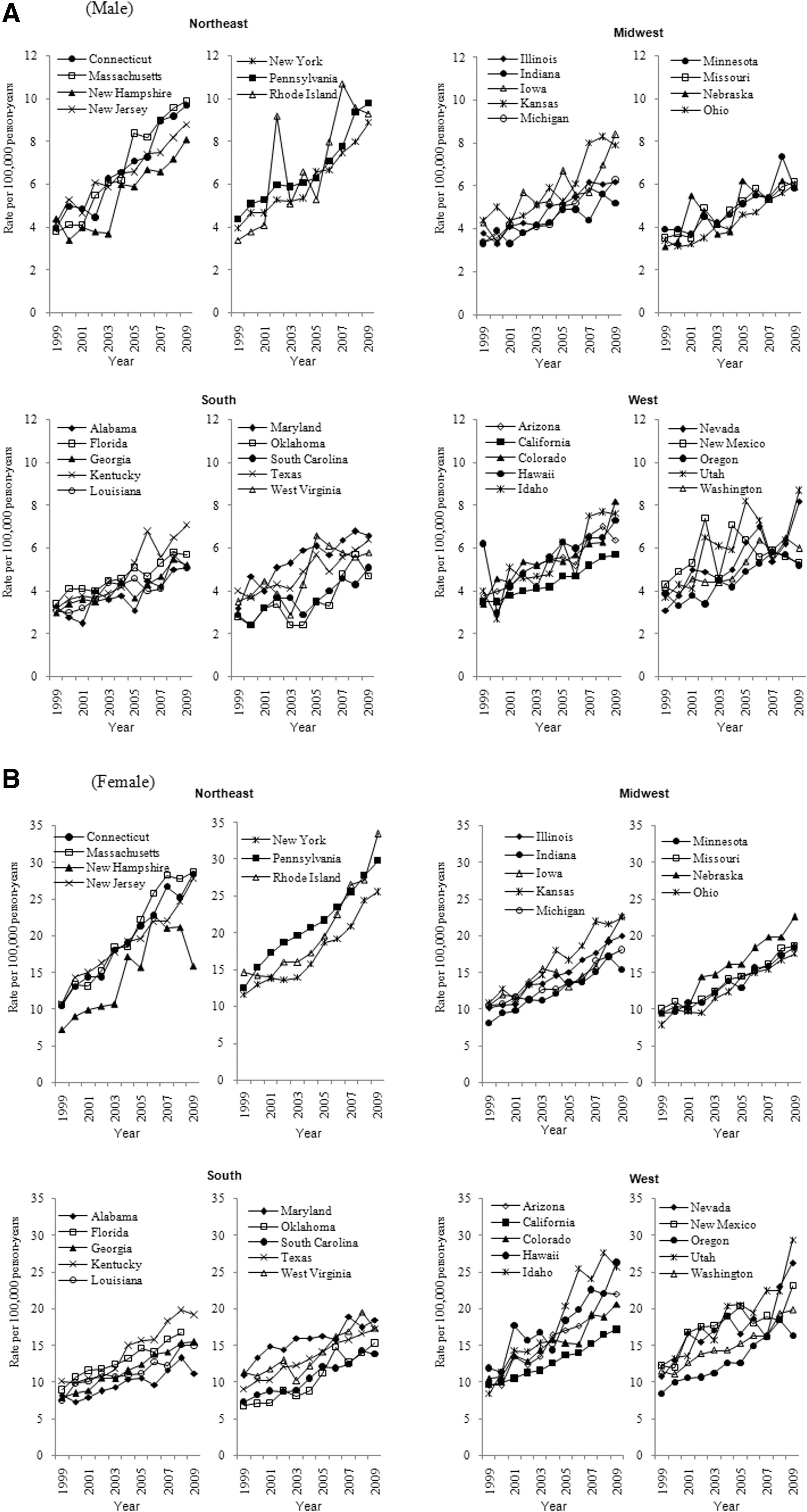
Trends in age-standardized thyroid cancer rates by gender and state for the time period 1999–2009:
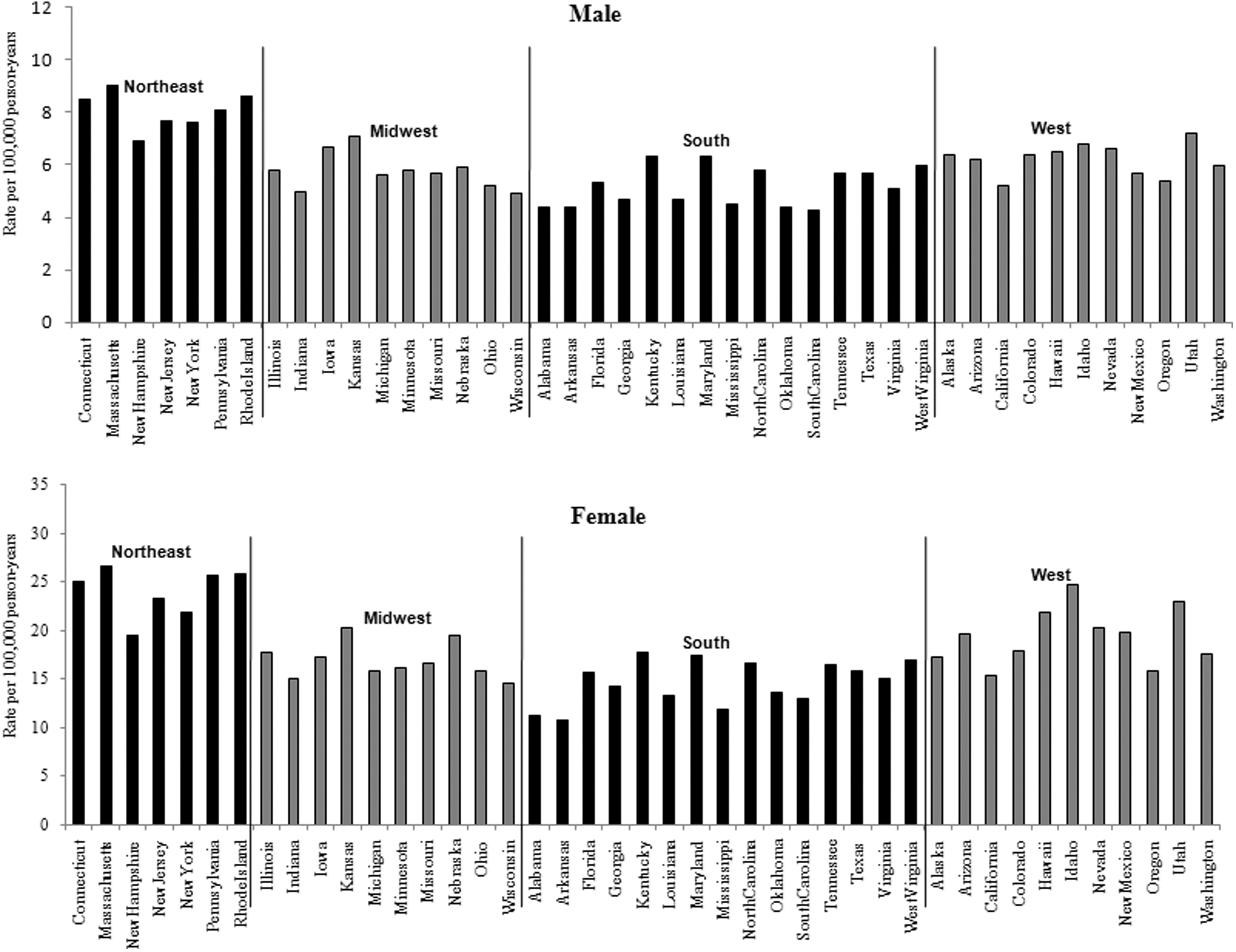
Age standardized incidence rates of thyroid cancer by U.S. state for the time period 2005–2009.
Data source: U.S. Cancer Statistics Working Group (6).
CI, confidence interval.
A total of 5923 endocrinologists, 27,533 general surgeons, and 97,936 primary care physicians were identified from the LifeScript Doctor Review list (7). As demonstrated in Figures 3 and 4, the densities of endocrinologists and general surgeons per 100,000 populations were also highest in the northeast. The incidence rates of thyroid cancer were significantly correlated with the densities of endocrinologists (r=0.58, p<0.0001 for males; r=0.44, p=0.0031 for females) and general surgeons (r=0.50, p=0.0006 for males; r=0.42, p=0.0045 for females). No significant associations between primary care physicians and the incidence rates of thyroid cancer were seen. The frequency of cervical ultrasonography was also highest in the northeast (Fig. 5). The linear correlation between the frequency of cervical ultrasonography and thyroid cancer incidence rates were statistically significant for both males (r=0.40, p=0.0091) and females (r=0.36, p=0.0197). However, there was no significant linear correlation between the frequency of thyroid biopsy and the incidence rates of thyroid cancer.
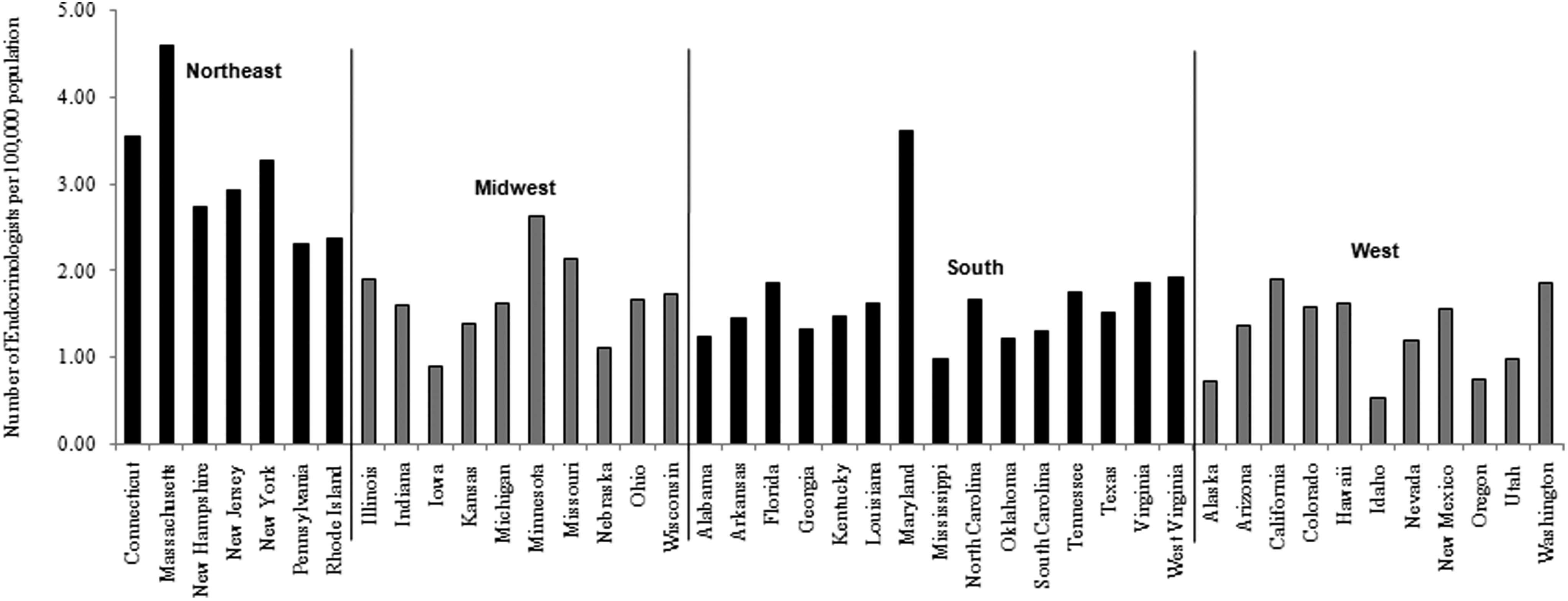
Density of endocrinologists by U.S. state (number of endocrinologists per 100,000 population).
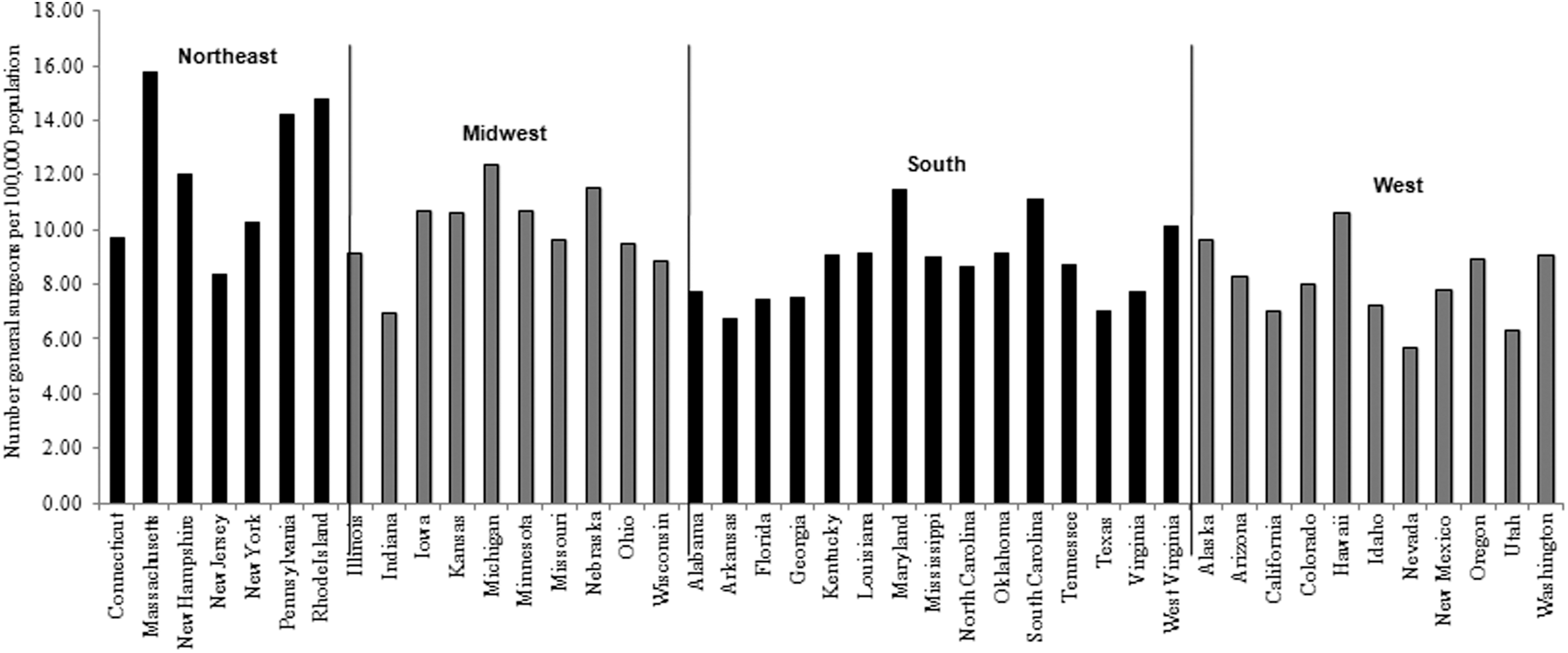
Density of general surgeons by U.S. state (number of general surgeons per 100,000 population).

The counts of neck ultrasonography per 100,000 commercially insured population for the period 2005–2009.
When the regression model included the densities of endocrinologists and general surgeons as well as the frequency of cervical ultrasonography, these three variables explained about 57% of the variability in state-level incidence for males (R 2=0.57, F=16.98, p<0.0001) and 49% for females (R 2=0.49, F=12.01, p<0.0001). After controlling for median household income, the model explained an additional 2% of the variability for both males (R 2=59, F=13.16, p<0.0001) and females (R 2=0.51, F=9.74, p<0.0001).
Discussion
Our study supports the notion that the epidemic of thyroid cancer in the United States is due in large part to increased detection. These findings have broad and significant public health and economic implications. Most thyroid cancers are small papillary tumors that are relatively slow growing that heretofore would not have been diagnosed. The diagnosis of a cytologically proven thyroid cancer results, for the vast majority of patients, in referral for surgical intervention. The most commonly performed procedure for a cytologically proven thyroid cancer according to the American Thyroid Association Guidelines is a total thyroidectomy and may also include a coincident central neck lymph node (level VI) dissection (10). It is not clear if all or even most of these patients benefit from surgical extirpation of what had once been clinically occult disease. Autopsy series suggest that patients who die from nonthyroid cancer-related disease frequently have occult thyroid cancers. The autopsy prevalence rate of occult thyroid cancer in the Finnish population is 35.6%, suggesting that thyroid cancer is both common and clinically insignificant for the vast majority of individuals (11).
In Japan, a subset of patients with subcentimeter cytologically proven thyroid cancer is being followed in the absence of surgical intervention (12). With more than 10 years of follow-up, surgical intervention was performed in only one third of these patients. The majority showed no evidence of disease progression, as evidenced by either tumor growth or development of nodal metastases. Importantly, no patient appears to have been harmed by prudent observation. A recent study examined the risk of secondary cancers after a first thyroid cancer primary utilizing the SEER database found that the highest risk was observed in patients with recently diagnosed microcarcinomas, indicating a potential negative impact from treatment for occult thyroid microcarcinomas (13). This epidemic of thyroid cancer is a classic example of “cancer overdiagnosis” where the diagnosis is made in a silent disease reservoir and treatment is initiated for individuals who are unlikely to develop symptoms or have their life-spans shortened (14). It is likely that individuals with clinically insignificant thyroid cancer would not benefit from either surgery or additional treatments including radioactive iodine and lifelong thyroid hormone suppression and/or replacement.
Because the results from our study and another study (3) showed that approximately half of the variability in thyroid cancer incidence in either state or county levels could not be explained by the “overdiagnosis” theory, the possibility of environmental factors resulting in the increased incidence of thyroid cancer should also be considered.
There is a clear association between the development of thyroid cancer and exposure to ionizing radiation, especially in childhood. Supportive evidence includes the dramatic outbreak of thyroid cancer, particularly in children and young adults that occurred following nuclear accidents such as the Chernobyl event in 1986 (15). A dramatic rise in medical imaging includes the increased use of nuclear medicine studies and more strikingly axial imaging, particularly computed tomography (CT) scans, employed in children and young adults (16). The thyroid gland exposure during a head and neck CT scan is up to 52.0 mGy (17). Neck CT scans are associated with an increased risk of developing thyroid cancer up to 390 per million patients (17).
Chemical exposure should also be considered. Blood concentrations of polybrominated diphenyl ether flame retardants (PBDEs) alter thyroid hormone homeostasis and cause thyroid dysfunction (18). Exposure to PBDEs in the U.S. population has increased significantly during the past decades (19), paralleling the observed increasing trend of thyroid cancer. Although there is lack of direct human evidence, these chemicals have been speculated to be responsible for some of the increasing trend of thyroid cancer (20).
Obesity influences thyroid hormone levels and leads to insulin resistance and increased production of insulin and insulin-like growth factors, which have been linked to thyroid disorders (21,22). Epidemiological studies have consistently reported that individuals who are either overweight or obese are at an increased risk of thyroid cancer (23 –27). The increasing trend of obesity might be another factor that accounts for some of the observed increasing incidence of thyroid cancer, although the degree of its contribution is unclear. Both deficiency and overconsumption of iodine have been suggested to be risk factors for thyroid cancer, although the results from epidemiologic studies have been inconsistent (28 –30). Based on the data from the National Health and Nutrition Examination Survey (NHANES), urinary iodine measurements have shown that the general U.S. population is iodine sufficient, although urinary iodine levels decreased by more than 50% between 1971 and 1974 and 1988 and 1994, and have remained stable since 2000 (31,32). It seems unlikely that the change in iodine consumption is a possible explanation of the increased trend of thyroid cancer in the Unites States.
Several limitations should be considered when interpreting the study results. The use of ultrasound is likely underrepresented by the OptumInsight. Many endocrinologists routinely use bedside ultrasound and don't bill unless there is a fine-needle aspiration. In addition, many patients would not be captured with this database, and there may be variability in the number captured based on region. While the LifeScript Doctor Review includes approximately 75% of the total number of U.S. doctors, it is unclear whether the coverage varies by state. Many identified general surgeons or endocrinologists may not focus on the thyroid. Endocrine surgeons, however, would be captured in the general surgeon population. Furthermore, we were unable to capture the density of otolaryngologists and their use of thyroid ultrasounds. Given these crude measurements, it is likely that the true associations between thyroid cancer incidence and the densities of endocrinologists and general surgeons, as well as the frequency of cervical ultrasound, were underestimated.
In conclusion, the thyroid cancer epidemic is real. The increased incidence of thyroid cancer is most likely due to overdiagnosis given that 57% of the variability in state-level incidence for males and 49% for females are due to densities of endocrinologists and general surgeons, and the use of ultrasound. It is likely that the majority of diagnosed thyroid cancer patients will not benefit from surgical and/or adjuvant interventions. As a medical community, we must critically analyze our response to treat heretofore undetectable and frequently indolent disease.
Footnotes
Acknowledgments
This research was partially supported by the NIH grant ES020361 and ACS grant RSGM-10-038-01-CCE.
Author Disclosure Statement
No competing financial interests exist for either of the authors.