
Abstract
Background:
Population-based studies investigating the sex-specific association between thyrotropin (TSH) levels and serum lipid concentrations are scarce. We examined the association between TSH and total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglycerides in men and women from the general population. Furthermore, the association with TSH outside and within the reference range and lipid levels was studied.
Methods:
Individual data of 13,571 men and women without lipid medication of four population-based studies conducted in Western European adults were pooled for cross-sectional analyses. The association between TSH levels and lipid concentrations were analyzed by calculating sex-specific multivariable median regression models.
Results:
In the pooled population, serum TSH levels were significantly positively associated with triglyceride values in men and with total cholesterol, LDL cholesterol, and triglyceride values in women. In the pooled male population, low serum TSH levels (<3.0 mIU/L) were significantly associated with lower total cholesterol, while high serum TSH levels (≥3.0 mIU/L) were associated with higher triglyceride values. In the pooled female population, low serum TSH levels were significantly associated with lower total cholesterol, LDL cholesterol, and HDL cholesterol. High TSH levels were associated with higher total cholesterol and LDL cholesterol in the pooled female population. In both sexes, serum TSH levels within the reference range (0.3–3.0 mIU/L) were significantly positively associated with triglyceride concentrations.
Conclusions:
Increasing levels of TSH were associated with a less favorable lipid profile in both men and women from the general population. In both sexes, TSH levels within the reference range were significantly positively associated with triglyceride concentrations.
Introduction
T
In the present study, we pooled data of four large population-based studies conducted in Western Europe including more than 14,000 individuals to investigate the association between TSH, the most important marker for thyroid function, and total serum cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride levels. Furthermore, these associations were studied for TSH within the reference range as well as low and high serum TSH and lipid levels.
Material and Methods
Study population
Data from three population-based German studies using a common standardized protocol, the Study of Health in Pomerania (SHIP-0) (19), the Cooperative Health Research in the Region of Augsburg Survey F4 (KORA F4) (20), the Cardiovascular Disease, Living and Ageing in Halle (CARLA) Study (21), and the population-based Danish INTER99 study (22) were pooled together for analysis.
Study characteristics are summarized in Table 1. Comprehensive information on these studies is given elsewhere in more detail (19 –22). In all studies, participants gave informed written consent, and the studies followed the recommendations of the Declaration of Helsinki and were approved by the local Ethics Committees.
TSH, thyrotropin; SHIP, Study of Health in Pomerania; CARLA, Cardiovascular Disease, Living and Ageing in Halle Study; KORA F4, Cooperative Health Research in the Region of Augsburg Survey F4.
Exclusion criteria
From each study, we excluded all participants with missing data in any of the considered variables. The number of excluded subjects were 113 (2.6%) in SHIP, 1088 (16.0%) in INTER99, 59 (3.3%) in CARLA, and 95 (3.1%) in KORA. Furthermore, we excluded all participants with lipid-affecting medication (365 in SHIP, 8.7%; 70 in INTER99, 1.2%; 284 in CARLA, 16.5%; and 360 in KORA, 12.1%).
Interview and physical examination
In all studies, trained and certified staff administered standardized personal interviews and conducted standardized examinations (19 –22). Hypertension was defined as systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg and/or use of antihypertensive medication. Use of antihypertensive medication was assumed in subjects answering “yes” to the question “Was medication against high blood pressure prescribed by a physician during the last year?” Smoking status was categorized into the three categories: smokers, former smokers, and never smokers. Former smokers were individuals who had smoked during their lifetime but not in the last 12 months prior to the time of the baseline examination. Height and weight were measured for the calculation of the body mass index (BMI), calculated as weight in kilograms divided by height in meters squared. Individuals who participated in leisure time physical training during summer and winter and were active for at least one hour per week in either season were classified as being physically active.
Laboratory measurements
In the INTER99 and the KORA study, blood was collected in a fasting state, while in the other studies, blood was drawn from nonfasting participants. The measurement procedures for TSH, total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides in the four studies are given in Table 1. The TSH reference range was defined as 0.3–3.0 mIU/L (23). Serum TSH levels <0.3 mIU/L were defined as low, and serum TSH levels ≥3.0 mIU/L were defined as high.
Statistical analysis
Results of continuously measured characteristics are expressed as median and interquartile range; distributions of categorical variables are expressed as percentages and absolute numbers. TSH levels were associated with lipid variables by sex-specific multivariable median regression models adjusted for age, body mass index (BMI), smoking status, alcohol consumption, and physical activity. All regression models were calculated separately for each individual study. Because in each of the included studies the same directions of associations between TSH values and the different lipid values were found, the analyses were also conducted for the pooled population. Pooled data analysis was additionally adjusted for study. In SHIP, CARLA, and the pooled analyses, all models were adjusted for time of blood taking and fasting status. In the analyses with categorized TSH (low and high), serum TSH levels within the reference range are the reference. In all analyses, fractional polynomials were applied to explore and graph nonlinear associations (24). The dose–response relation was found using fractional polynomials up to degree 2 with all possible combinations of powers selected from the set (−2, −1, −0.5, 0, 0.5, 1, 2, 3) and compared using the log likelihood to determine the best-fitting model. If none of the fractional polynomials models fitted the data significantly better than the linear model, serum TSH levels were used untransformed. For all multivariable analyses, TSH was transformed by a power transformation to reduce the effects of outliers on the fractional polynomials (24). A p-value of <0.05 was considered as statistically significant. All analyses were performed using Stata v11.1 (Stata Corp., College Station, TX).
Results
Total cholesterol, LDL cholesterol, and HDL cholesterol levels were comparable between the studies, while triglyceride levels were lower in the INTER99 and the KORA study, probably due to blood collection in a fasting state (Table 2).
Data are expressed as median and inter-quartile-range (continuous data), or as number and percentage (categorical data).
Defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or intake of antihypertensive medication.
LDL, low-density lipoprotein; HDL, high-density lipoprotein.
There were significant interactions between sex and TSH for LDL cholesterol (p<0.001), HDL cholesterol (p<0.001), and triglycerides (p<0.001), but not between sex and TSH for total cholesterol (p=0.252). In men, multivariable regression analyses stratified by study revealed significantly positive association between serum TSH levels and LDL cholesterol values in CARLA and between serum TSH levels and triglycerides in SHIP, INTER99, and KORA (Table 3). In females, however, there was a significantly positive association between serum TSH levels and total cholesterol, as well as LDL cholesterol concentrations in SHIP, CARLA, and KORA, and between serum TSH concentrations and triglyceride levels in SHIP, INTER99, and KORA. In none of the studies were serum TSH levels associated with HDL cholesterol values. In the pooled population, serum TSH levels were significantly positively associated with triglyceride values in men and with total cholesterol, LDL cholesterol, and triglyceride values in females (Table 3 and Fig. 1). The magnitude of the association between serum TSH levels and lipid levels can be seen in Figure 1. For example, a female with a serum TSH level of 3.0 mIU/L has a 0.175 mmol/L higher total cholesterol value compared to a female with a serum TSH level of 0.3 mIU/L.
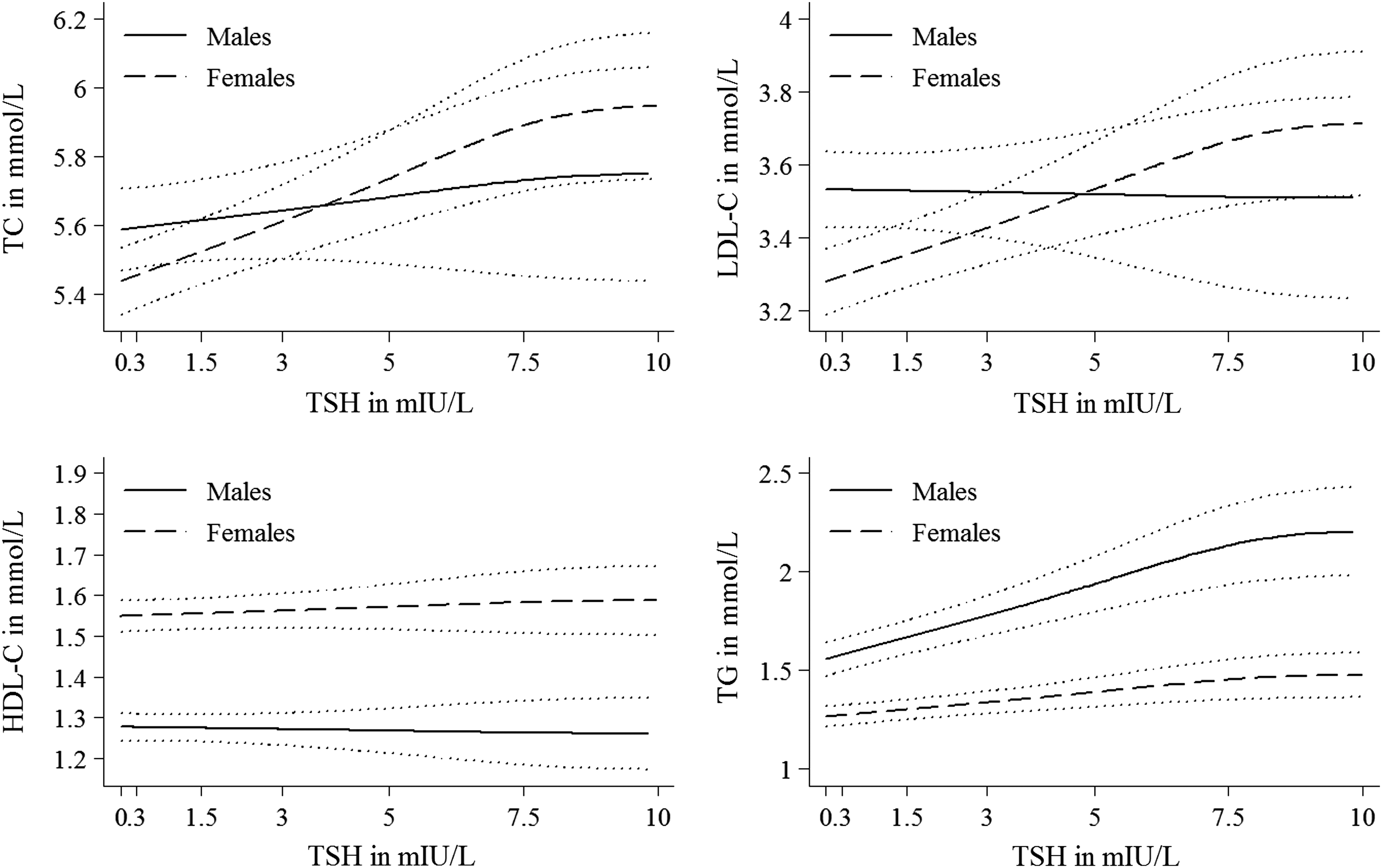
Sex-specific adjusted regression curves showing the association between TSH levels and the different serum lipid levels based on the pooled sample. Dotted lines represent confidence intervals (CIs). TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; TSH, thyrotropin.
Median regression; all models adjusted for age, BMI, smoking status, alcohol consumption, and physical activity. Pooled analyses were additionally adjusted for study. In SHIP, CARLA, and the pooled analyses, all models were adjusted for the time blood was taken and fasting status. Fractional polynomials were applied to test for a nonlinear association between power-transformed serum TSH levels and the respective outcome. There was no evidence of a nonlinear relationship.
p<0.05.
CI, confidence interval.
In males, low serum TSH levels (<0.3 mIU/L) were negatively associated with total cholesterol in SHIP and positively associated with LDL cholesterol in KORA, but not with the other lipids in any of the single studies or in the pooled population (Table 4). High serum TSH levels (≥3.0 mIU/L) were positively associated with triglyceride values in INTER99 and in the pooled male population. In females, low serum TSH levels were significantly negatively related to total cholesterol in CARLA and also in the pooled population. Furthermore, low serum TSH levels were significantly inversely associated with LDL cholesterol in INTER99 and the pooled population, and with HDL cholesterol in the pooled population. High serum TSH levels were positively related to total cholesterol in the pooled population and with LDL cholesterol in SHIP and the pooled female population (Table 4).
Median regression; all models adjusted for age, BMI, smoking status, alcohol consumption, and physical activity. Reference: TSH within the reference range (0.3–3.0 mIU/L). Pooled data analysis additionally adjusted for study. In SHIP, CARLA, and the pooled analyses, all models were adjusted for the time blood was taken and fasting status.
p<0.05.
In males, serum TSH levels within the reference range (0.3–3.0 mIU/L) were positively associated with triglyceride values in INTER99 and in the pooled population, but there were no further associations with lipids in the single studies or the pooled population (Table 5). In females, there were significant positive associations between serum TSH levels within the reference range and total as well as LDL cholesterol in CARLA, but not in any of the other single studies or in the pooled population. Serum TSH levels within the reference range were significantly associated with triglyceride values in females of SHIP, KORA, and the pooled population.
Median regression; all models adjusted for age, BMI, smoking status, alcohol consumption, and physical activity. Reference range for TSH levels: 0.3–3.0 mIU/L. Pooled data analysis additionally adjusted for study, time the blood was taken, and fasting status. Fractional polynomials were applied to test for a nonlinear relationship between power-transformed serum TSH and the respective outcome. There was no evidence of a nonlinear relationship.
p<0.05.
Sensitivity analysis
The strengths of the relationships were unchanged after excluding pregnant women and adjustment for oral contraceptive use or hormone replacement therapy in the SHIP sample (data not shown).
Discussion
In the present large cross-sectional analysis including data of four population-based studies from Western Europe, increasing levels of TSH were associated with a less favorable lipid profile in both males and females. In the pooled population, serum TSH levels were significantly positively associated with triglyceride values in men and with total cholesterol, LDL cholesterol, and triglyceride values in women. However, neither in males nor in females were TSH levels associated with HDL cholesterol values. In both sexes, TSH levels within the reference range were significantly positively associated with triglyceride concentrations only.
A prior population-based study, including 30,656 males and females aged 20 years and older, investigating the relationship between TSH within the reference range and serum lipid concentrations found that TSH was positively associated with total serum cholesterol, LDL cholesterol, non-HDL cholesterol, and triglyceride values. The study also showed a linear inverse association between TSH and HDL cholesterol concentrations (18). In another study from Norway including 5143 individuals, a positive association between serum TSH levels and total cholesterol as well as LDL cholesterol levels was shown (25). Very recently, a cross-sectional study including more than 20,000 Spanish individuals from several primary healthcare centers reported a significant direct trend between TSH categories and total cholesterol, triglycerides and LDL cholesterol levels, and an inverse trend with HDL cholesterol values in both men and women (26). Further recent studies—one conducted in a Hispanic population (27), another in a Chinese population (28)—found a significant association between TSH values and total cholesterol and triglycerides in euthyroid subjects. Additionally, Lee et al. showed a significantly positive correlation between TSH within the reference range and total cholesterol, triglycerides, and LDL cholesterol, but not HDL cholesterol (29). These findings are in contrast to the present study. In the pooled sample, in sex-stratified analysis, we also found only a significantly positive association between TSH within the reference range and triglyceride values in both men and women. This is also contrary to the sex-specific results of the population-based EPIC Norfolk study, which reported a significant association between TSH within the reference range and total cholesterol, LDL cholesterol, and HDL cholesterol levels in men, and a significant association between normal TSH levels and HDL cholesterol in women (17). In another community-based study including Australian women aged 18–75 years, total cholesterol and triglyceride values, but not LDL cholesterol or HDL cholesterol values, were positively correlated with serum TSH levels (30).
In our study, a significantly inverse association between low serum TSH levels and total cholesterol was found in men. In females, low serum TSH levels were significantly inversely associated with total cholesterol, LDL cholesterol, and HDL cholesterol values. These findings are in line with prior studies on this issue (31,32).
In males, high serum TSH levels were positively associated with triglyceride values, while in females high TSH levels were positively associated with total cholesterol and LDL cholesterol levels. These results are in concordance with prior studies showing that hypothyroid patients have increased levels of total cholesterol and LDL cholesterol values (3,33,34). Dyslipidemia associated with overt hypothyroidism predisposes to the development of atherosclerotic coronary artery disease (35,36). Constantini et al. found that decreased thyroid function not only increases the number of LDL particles, but also promotes LDL oxidability (37). However, another study reported that hypothyroidism leads to decreased concentrations and oxidation rates of lipid intermediates in the presence of unaltered rates of lipolysis (38). In addition, prior studies have shown that hypothyroidism has an adverse impact on other cardiovascular risk factors such as arterial hypertension, C-reactive protein, and glucose metabolism, and can thus further contribute to an increased atherosclerotic coronary artery disease risk (39,40).
A number of mechanisms suggest that thyroid hormones might affect changes in lipid metabolism. It was assumed that thyroid hormones enhance the utilization of lipid substrates, increase the synthesis and mobilization of triglycerides stored in adipose tissue, and increase the concentration of nonesterified fatty acids (36). Thyroid hormones affect enzyme activities, transfer proteins, and receptors involved in lipid metabolism (13). In addition, it could be shown that serum TSH levels were positively associated with BMI and waist circumference (41), and it was assumed that the association between serum TSH and cholesterol is modified by insulin resistance (42).
However, the reasons for the sex differences regarding the association between TSH levels and lipid profiles, particularly outside the reference range, are not clear. One explanation might be pathomechanisms driven by genetic traits (43), possibly suggesting a genetic basis for the sex differences. Furthermore, studies showed that there are sex differences in enzyme activities, for example hepatic lipase activity (44) and free fatty acid (FFA) concentrations as well as FFA turnover rates differ between men and women (45). Also, TSH levels (46) as well as lipid values (47,48) are affected by sex hormones, such as estrogens. Finally, it is well known that after the menopause, body composition changes in women, which is associated with an increase in abdominal fat deposition and adverse metabolic changes, consequently leading to a more frequent occurrence of insulin resistance (49). Thus, it could be speculated that these factors might be jointly responsible for the findings. More research is needed to elucidate what factors are responsible for the sex differences found regarding the relationship between TSH levels and lipid profile.
The cross-sectional design of the study represents a limitation, implicating that a cause and effect cannot be discerned. Further limitations arise from different measurement techniques of serum TSH levels between the included studies. In the INTER99 and the KORA study, blood samples were taken in fasting subjects, whereas in SHIP and CARLA blood samples were taken in nonfasting participants, which might explain the lower median serum TSH levels of the individuals in the SHIP and CARLA study compared to those in the other studies (50). Reasons for the difference in serum TSH levels between the studies might arise from a real difference of serum TSH levels between the studies, from an effect of fasting versus nonfasting sample taking, or from the circadian rhythm of serum TSH levels.
To address this issue, each of the pooled analyses was adjusted for study. While triglyceride concentrations are sensitive to eating, cholesterol levels are less influenced (51). Furthermore, diurnal variations in serum TSH have to be taken into consideration, with relatively higher levels in the morning in comparison with levels later in the day (52). Although it is not entirely clear whether these variations may influence the association between TSH and serum lipids, in the present analyses, we adjusted for the time the blood was drawn. In the analyses of triglycerides, models were additionally adjusted for fasting status.
The strength of the study is the large number of individuals, representative of the general Caucasian population in Western Europe.
In conclusion, the present data show that increasing levels of TSH are associated with a less favorable lipid profile in both men and women from the general population. Furthermore, in both sexes, TSH levels within the reference range were significantly positively related to triglyceride concentrations. Further studies, in particular prospective studies, are needed to investigate the impact of thyroid function on lipid profile and the clinical relevance of an association regarding the development of cardiovascular diseases.
Footnotes
Acknowledgments
The KORA research platform and the KORA Augsburg studies are financed by the Helmholtz Zentrum München, German Research Center for Environmental Health (GmbH), which is funded by the German Federal Ministry of Education, Science, Research and Technology and by the State of Bavaria. Thyroid examinations were additionally funded by Sanofi-Aventis in the framework of the Papillon Initiative. SHIP is part of the Community Medicine Research net of the University of Greifswald, Germany, which is funded by the Federal Ministry of Education and Research (BMBF 01ZZ9603 and 01ZZ0103), the Ministry of Cultural Affairs, as well as the Social Ministry of the Federal State of Mecklenburg-West Pomerania. Statistical analyses were supported by the Deutsche Forschungsgemeinschaft (DFG VO 955/12-1).
The CARLA Study was funded by a grant from the Deutsche Forschungsgemeinschaft as part of the Collaborative Research Center 598 “Heart failure in the elderly—cellular mechanisms and therapy” at the Medical Faculty of the Martin Luther University Halle–Wittenberg, by a grant of the Wilhelm–Roux Program of the Martin Luther University Halle–Wittenberg, by the Ministry of Education and Cultural Affairs of Saxony-Anhalt, and by the Federal Employment Office.
The INTER99 was undertaken at the Research Center for Prevention and Health. The Steering Committee of the INTER99 study comprises Torben Jørgensen, DMSci (principal investigator); Knut Borch-Johnsen, DMSci (co-principal investigator); Charlotta Pisinger, PhD, MPH; Hans Ibsen, DMSci; and Troels F. Thomsen, PhD. The INTER99 study was supported by the Danish Medical Research Council, the Danish Centre for Evaluation and Health Technology Assessment, Novo Nordisk, Copenhagen County, the Danish Heart Foundation, the Danish Pharmaceutical Association, Augustinus Foundation, Ib Henriksens Foundation, and Beckett Foundation.
The contribution to data collection made by field workers, technicians, interviewers, and computer assistants in all studies is gratefully acknowledged.
Author Disclosure Statement
There is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.