
Abstract
Background:
Voice problems following thyroid surgery are well known, and perioperative voice analysis in patients undergoing thyroidectomy no longer seems optional. However, multiple means of assessing vocal function are time-consuming, require specific instruments and specialists, and increase costs. Therefore, we designed this study to develop an efficient and cost-effective screening tool for detecting voice disorders following thyroidectomy.
Methods:
We developed the Perioperative Voice-Screening Protocol for Thyroid Surgery (PVST) using the Thyroidectomy-Related Voice Questionnaire (TVQ) to provide a cost-effective diagnostic flow chart for patients following thyroidectomy. The TVQ is a simple questionnaire that was developed at our institution and has already demonstrated its effectiveness in detecting pre- and postthyroidectomy voice-related disorders in our previous studies. To investigate the PVST, we enrolled 242 subjects who underwent thyroidectomy and let them follow the PVST. All subjects underwent a voice work-up by a voice specialist to verify the predictive value of the protocol.
Results:
Using PVST, we could effectively screen for abnormal preoperative laryngeal findings with sensitivity and specificity of 82.1% and 50.5%, respectively, especially laryngeal benign mucosal disease with sensitivity and specificity of 100% and 45.6%, respectively. We could also screen for postoperative voice-related problems with sensitivity and specificity of 100% and 50.4% for detecting vocal-cord palsy, and 66.7% and 51.2% for detecting a low-pitched voice, respectively. If all 242 patients followed the protocol, US $42,768 would be saved, and the PVST was estimated to decrease costs by 43.5%.
Conclusions:
The PVST is a reliable and cost-effective perioperative screening tool that enables thyroid surgeons to detect patients with voice problems in their routine outpatient clinic for early and appropriate referral to voice specialists.
Introduction
The Thyroidectomy-Related Voice Questionnaire (TVQ) was developed at our institution. It is a self-assessment tool that measures voice quality (Table 1). This questionnaire was developed based on the voice handicap index (VHI) and other subjective symptoms related to thyroid surgery (14,15). We have demonstrated that the questionnaire is a simple and effective screening tool with which to detect pre- and postthyroidectomy voice-related disorders that can affect voice quality (13,16). Based on these encouraging results, we developed and adopted the Perioperative Voice-Screening Protocol for Thyroid Surgery (PVST) using this questionnaire to provide a safe and cost-effective diagnostic flow chart for patients following thyroidectomy. In this study, we evaluated the efficacy and effectiveness of the PVST for screening voice disorders following thyroidectomy.
Instructions. These statements describe your voice and voice-related symptoms and the effects that these symptoms have on your life. Circle the response that indicates how frequently within the past month you have encountered the same experience: 0, never; 1, almost never; 2, sometimes; 3, almost always; or 4, always.
Materials and Methods
Study design
The study group comprised 242 patients who underwent thyroidectomy for benign or malignant thyroid tumors at Seoul St. Mary's Hospital, Korea, between January 2012 and July 2012. Subjects were excluded if they had a history of head and neck surgery (including prior thyroid surgery), or if they planned to undergo modified radical neck dissection to eradicate cervical lymphatic metastasis, partial laryngeal or tracheal resection due to tumor invasion, or an endoscopic or robotic approach. One surgeon performed all operations in all patients using the same surgical technique under the same conditions. An intraoperative nerve-monitoring device was not used in any subjects.
All subjects enrolled in this study were asked to complete the TVQ at the outpatient clinic before and 2 weeks after thyroid surgery. All subjects underwent the same preoperative and postoperative voice work-ups and were subsequently classified into four groups according to the indications of the voice work-up of the PVST (Fig. 1). The PVST is the perioperative voice-screening protocol for thyroid surgery using our questionnaire (TVQ) to provide a safe and cost-effective diagnostic flow chart for patients after a thyroidectomy (Fig. 2). The voice work-up includes fiber-optic laryngoscopic examination, videostroboscopic examination, perceptual voice analysis, and acoustic analysis. We investigated the efficacy and effectiveness of the PVST for screening voice disorders following a thyroidectomy. All subjects were informed of the nature of the study and gave informed consent. The institutional review board of our institution approved the protocol of our study.
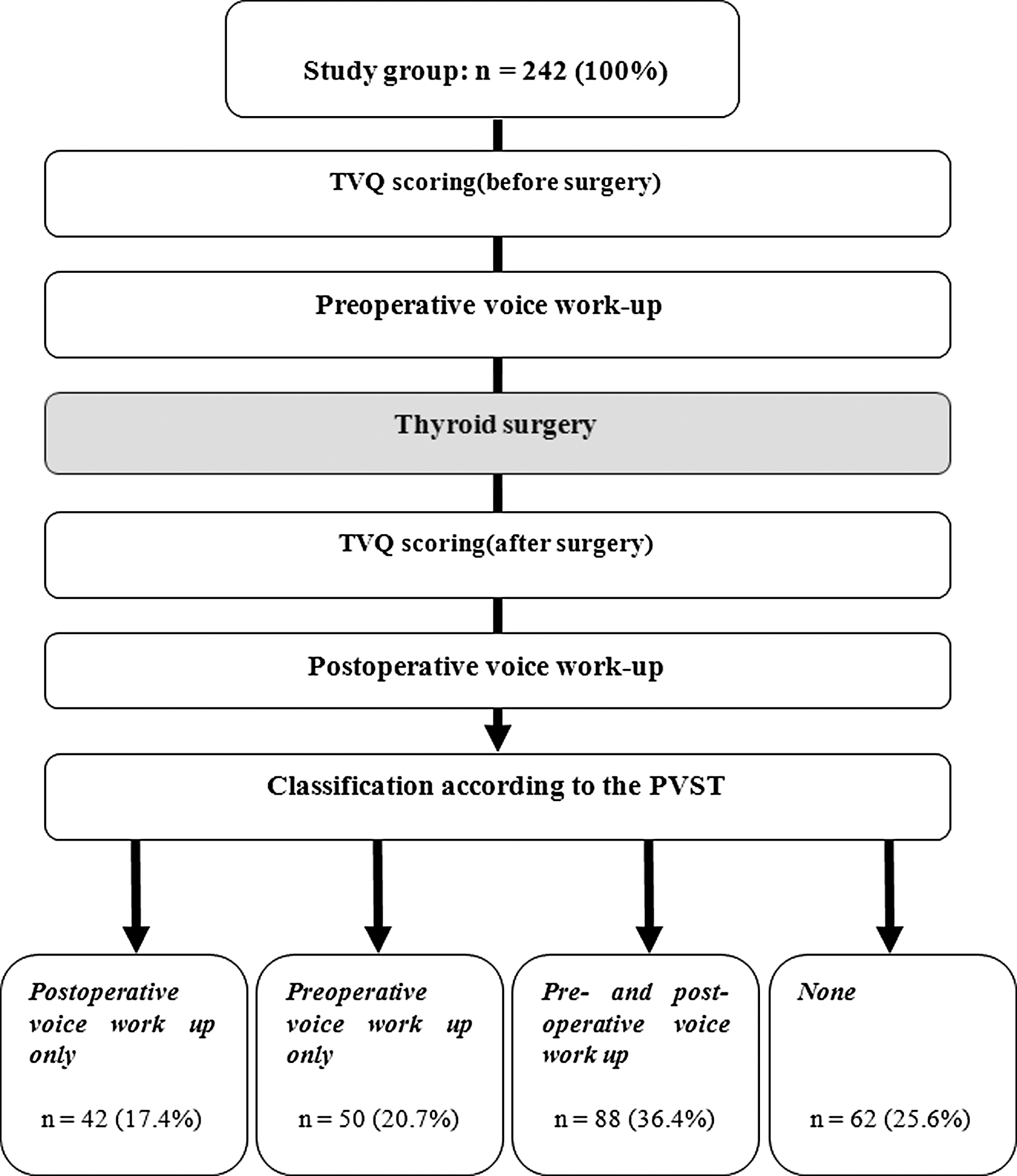
Study design to investigate the efficacy and effectiveness of the Perioperative Voice-Screening Protocol for Thyroid Surgery (PVST) for screening voice disorders following thyroidectomy.
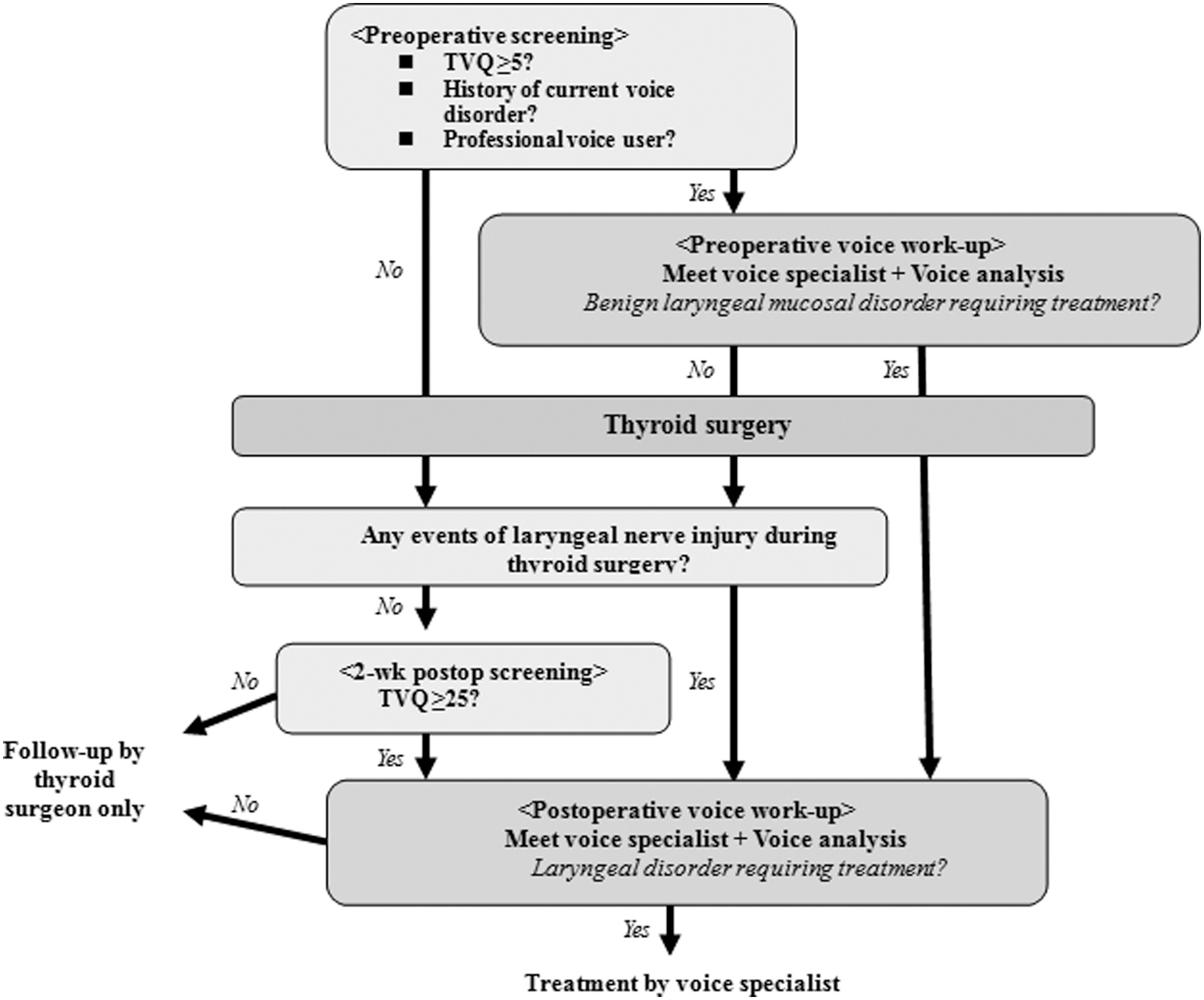
Perioperative Voice-Screening Protocol for Thyroid Surgery (PVST).
TVQ ( Table 1 )
The TVQ comprises 20 questions; responses to each are scaled from a minimum of 0 (no voice alterations or symptoms) to a maximum of 80 (highest voice impairment and multiple vocal symptoms).
PVST (Fig. 2)
All patients are asked to complete the TVQ at the outpatient clinic before thyroid surgery. Patients who meet the following indications undergo evaluations including videostroboscopy, perceptual voice analysis, and computerized acoustic analysis, as well as a physical examination and counseling by a voice specialist before thyroid surgery. Indications for a voice work-up before thyroid surgery are as follows: (i) a preoperative TVQ score of ≥5, (ii) a current voice disorder, and (iii) a professional voice user, defined as someone whose voice is essential to their job and in whom special or unique voice qualities are often the essential feature of their careers (e.g., singers, actors, broadcast personalities). If any laryngeal disorder requiring surgery is found (vocal polyps, cysts, etc.), laryngeal surgery should be planned to be performed simultaneously with thyroid surgery so that patients can avoid additional general anesthesia. After thyroid surgery, all patients are asked to complete the TVQ at the outpatient clinic 2 weeks postoperatively. Patients who meet the following indications undergo voice evaluations including videostroboscopy, perceptual voice analysis, and computerized acoustic analysis and meet with a voice specialist postoperatively. Indications for a voice work-up after thyroid surgery are as follows: (i) any occurrence of laryngeal nerve injury during thyroid surgery, (ii) any preoperative benign laryngeal mucosal disorder requiring treatment, and (iii) a TVQ score of ≥25 at 2 weeks after thyroid surgery. For all patients with laryngeal disorders to be treated during the postoperative voice work-up, treatment is started according to the individual disease by a voice specialist. Patients who do not meet the indications are followed-up by a thyroid surgeon only with no additional voice work-up or examination by a voice specialist.
Fiber-optic laryngoscopic and videostroboscopic examinations
We examined the entire larynx, including the mucosal status and the presence of vocal fold diseases, using fiber-optic laryngoscopy (Machida Instruments, Tokyo, Japan) and videolaryngostroboscopy (model 9200C; KayPENTAX, Lincoln Park, NJ). The diagnosis of vocal fold disease and the RFS score were judged by two speech therapists and one otolaryngologist by consensus.
Perceptual voice analysis
Voice samples were recorded for all patients. They were instructed to read “Sanchaek (a walk)” at a comfortable volume and rate. Each patient's voice was also perceptually evaluated during a conversation. The patients provided information on their voice history and social history. A grade, roughness, breathiness, asthenia, strain (GRBAS) score was given at the end of the evaluation session. Then the recorded audiotapes of the reading were replayed after the evaluation session to reconsider the GRBAS scores. Any variation in the GRBAS scores between reading and conversation was considered, and preference was given to the scores obtained during conversation. The voice was scored using the five GRBAS parameters: grade=overall degree of voice deviance, roughness=irregular fluctuation of the fundamental frequency, breathiness=turbulent noise produced by air leakage, asthenia=overall voice weakness, and strain=impression of tenseness or excess effort. Each parameter was scored on a scale of 0 to 3 (0, normal; 1, slight disturbance; 2, moderate disturbance; and 3, severe disturbance). The voices were judged by two speech therapists and one otolaryngologist by consensus.
Acoustic analysis
Patients were instructed to produce the vowel “a” at a comfortable volume and constant pitch. Each vowel pronunciation was recorded with a constant mouth-to-microphone distance of 5 cm using Computerized Speech Lab (CSL, model 4150; KayPENTAX). All digital recordings were made in a quiet room. Each patient sustained an “a” for at least 3 sec at a comfortable pitch level. The task was repeated four times or more, and the fourth trial was often the recorded sample. Each analysis was made by the Multi-Dimensional Voice Program (MDVP, model 5105, ver. 3.1.7; KayPENTAX). The parameters that were considered in the analysis were fundamental frequency, perturbations of fundamental frequency (jitter), amplitude (shimmer), glottal noise (i.e., the noise-to-harmonic ratio), and speaking fundamental frequency. The software defines normal jitter values up to n<1.1% and shimmer values up to n<3.8%. The normal noise-to-harmonic ratio is n<0.2.
Statistical analysis
Statistical analyses were performed using SPSS v18.0 for Windows (SPSS, Chicago, IL). The chi-square test, Fisher's exact test, Student's t-test, and correlation analysis were used as appropriate to identify significant differences in the clinical parameters according to the TVQ score. A p-value of <0.05 was considered statistically significant.
Results
Characteristics of the patients
A total of 242 patients were enrolled in this study with a mean age of 46 years. The patients' characteristics are summarized in Table 2. According to the PVST, 88 patients (36.4%) underwent both preoperative and postoperative voice work-ups, 62 (25.6%) underwent no work-up, and 92 (38.1%) were either evaluated with a preoperative or postoperative voice work-up (Fig. 1).
PSVT as a preoperative screening tool
The comparative results of voice-related parameters between patients who were and were not found to have an indication for a postoperative voice work-up according to the PVST are summarized in Table 4. Of the 242 patients, 130 (53.7%) were found to have an indication for a postoperative voice work-up according to the PVST: (i) TVQ ≥25 (n=130) and/or (ii) any laryngeal nerve injuries during thyroid surgery (n=2) and/or (iii) patients who were found to have benign laryngeal mucosal disease during the preoperative voice work-up (n=14). The study group was again divided into the two subgroups (Not Indicated and Indicated). According to the patients' characteristics, the rate of female patients was significantly higher in the Indicated than in the Not Indicated group (88.5% vs. 75.9%, p=0.01). According to the results of the postoperative voice analysis, the TVQ score, grade (G), and jitter were significantly higher in the Indicated than in the Not Indicated group (p=0.000, p=0.000, and p=0.033, respectively). The rate of surgery-related voice problems (low-pitched voice/vocal-cord palsy) was significantly higher in the Indicated than in the Not Indicated group (28.5% vs. 10.7%, p=0.001). The specificity, sensitivity, positive predictive value, and negative predictive value of the PVST for identification of surgery-related voice problems (vocal-cord palsy/low-pitched voice) are shown in Table 5. The sensitivities and specificities of the PVST were 66.7% and 51.2% and 100% and 50.4% for detection of a low-pitched voice and detection of vocal-cord palsy, respectively.
p<0.05.
Not Indicated, patients who did not require a postoperative specialized voice work-up; Indicated, patients who required a preoperative specialized voice work-up; TVQ, Thyroidectomy-Related Voice Questionnaire; F0, fundamental frequency; NHR, noise-to-harmonic ratio.
PSVT as a postoperative screening tool
The comparative results of voice-related parameters between patients who were and were not found to have an indication for a postoperative voice work-up according to the PVST are summarized in Table 4. Of the 242 patients, 130 (53.7%) were found to have an indication for a postoperative voice work-up according to the PVST: (i) TVQ ≥25 (n=130) and/or (ii) any laryngeal nerve injuries during thyroid surgery (n=2) and/or (iii) patients who were found to have benign laryngeal mucosal disease during the preoperative voice work-up (n=14). The study group was again divided into the two subgroups (Not Indicated and Indicated). According to the patients' characteristics, the rate of female patients was significantly higher in the Indicated than in the Not Indicated group (88.5% vs. 75.9%, p=0.01*). According to the results of the postoperative voice analysis, the TVQ score, grade (G), and jitter were significantly higher in the Indicated than in the Not Indicated group (p=0.000*, p=0.021, and p=0.036 respectively). The rate of surgery-related voice problems (low-pitched voice/vocal-cord palsy) was significantly higher in the Indicated than in the Not Indicated group (28.5% vs. 10.7%, p=0.001). The specificity, sensitivity, positive predictive value, and negative predictive value of the PVST for identification of surgery-related voice problems (vocal-cord palsy/low-pitched voice) are shown in Table 5. The sensitivities and specificities of the PVST were 66.7% and 51.2% and 100% and 50.4% for detection of a low-pitched voice and detection of vocal-cord palsy, respectively.
p<0.05.
GRBAS, Grade, Roughness, Breathiness, Asthenia, Strain.
n=242.
TP, true-positive; FP, false-positive; FN, false-negative; TN, true-negative; PPV, positive predictive value; NPV, negative predictive value.
Discussion
Voice change is a well-known and relatively frequent complication in patients who have undergone thyroid surgery, and many patients still suffer from voice-related problems with or without obvious accidental nerve injury or vocal-cord palsy. An appropriate screening tool is required for early detection and management of this problem. The required conditions for a screening tool with which to predict significant voice alterations in patients who have undergone thyroidectomy include (i) cost-effectiveness, (ii) noninvasiveness, (iii) not time-consuming, and (iv) the ability to be performed and interpreted by a thyroid surgeon, not a voice specialist. In the search for such a tool, some authors have reported the perioperative use of the VHI for patients undergoing thyroid operations to evaluate postthyroidectomy dysphonia (8,14,17). The TVQ was developed at our institution and is based on the VHI. The questions concern general voice complaints, representative symptoms related to LPR and vocal-cord palsy, and swallowing-related symptoms associated with thyroidectomy. We previously investigated its correlation with objective voice parameters, and the TVQ showed a statistically significant correlation with shimmer and G (correlation coefficients of 0.091 and 0.260, respectively). We also previously demonstrated that the questionnaire is an effective screening tool with which to detect pre- and postthyroidectomy voice-related disorders (13,16). We designed the PVST for patients who have undergone thyroidectomy using the TVQ, and the present prospective study was designed to investigate the predictive value and efficiency of PVST for determining voice problems not only in the postoperative period but also in the preoperative period of thyroid surgery.
Based on the indications for a preoperative voice work-up in PVST, we decided to use a preoperative TVQ score of ≥5. We chose this cut-off value based on our previous report, in which a questionnaire score of 5 showed the best sensitivity (74%) and specificity (71%) in discriminating whether a laryngeal abnormality was present or not (13). We also regarded patients with current voice disorders and professional voice users to be in need for a preoperative voice work-up. We considered a professional voice user as an individual whose special or unique voice qualities are an essential feature for their careers, such as singers, actors, and broadcast personalities. In terms of cost effectiveness, we did not include other occupational voice users such as teachers, clergy, salespeople, telemarketers, and receptionists, for whom spoken communication is an essential part of what they do but unique voice qualities are not essential. In our current study, there were no professional voice users.
As previously mentioned, all subjects who did not meet the indications according to the PVST also underwent the same voice work-up and met with a voice specialist to identify the laryngeal status of all subjects. Surprisingly, 56 patients (23.1%) showed abnormal laryngeal findings in the preoperative voice work-up by a voice specialist. LPR (9.5%), benign mucosal disease (5.8%), and nonspecific vocal fold edema (4.5%) were the most frequently found preoperative laryngeal abnormalities. Diagnostic methods for LPR include 24 h double-probe ambulatory pH monitoring, but this is a relatively invasive method, and results can differ according to the interpreter (18 –20). Thus, Belafsky et al. (18 –21) developed the RSI and RFS and concluded that they were readily administered, highly reproducible, and exhibited excellent construct- and criterion-based validity. Patients with RFS scores of 7 were considered to have LPR in this study (18).
We determined that the PVST is an effective screening tool with which to detect laryngeal abnormalities, especially in laryngeal benign mucosal disease, before thyroid surgery. The sensitivity and specificity of the PVST were 82.1% and 50.5% respectively for the detection of abnormal laryngeal findings overall. PVST is a particularly sensitive diagnostic modality for detecting benign laryngeal mucosal disease. The sensitivity and specificity were 100% and 45.6% respectively for benign mucosal disease. We regarded benign pathologic lesions of the larynx as benign mucosal diseases, including vocal nodules, vocal polyps, sulcus vocalis, Reinke's edema, granulomas, and epiglottic cysts. Benign mucosal diseases were found in 14 (5.8%) patients. These diseases usually have harmful effects on the voice that may also affect the voice recovery process after thyroid surgery. If these benign mucosal diseases are not detected preoperatively, they would likely be assumed to have resulted from the ensuing thyroid surgery; as a result, proper diagnosis and treatment may be delayed, and legal problems may occur. With the knowledge of preoperative laryngeal disease, microlaryngeal surgery and thyroidectomy can be simultaneously performed if necessary without problems. If they are not simultaneously performed, patients would miss the opportunity to address both problems in one procedural step. Two patients with vocal polyps underwent simultaneous microlaryngeal surgery in this study. One patient with a vocal polyp desired nonsurgical follow-up. Patients with vocal nodules were educated about vocal hygiene and voice rest and necessary medication (proton pump inhibitor) and were followed up by a voice specialist. Patients with sulcus vocalis, granulomas, and epiglottic cysts were educated about their disease; none desired intervention, and all were followed up by a voice specialist.
Based on the PVST-based indications for a postoperative voice work-up, we chose a postoperative TVQ score of ≥25. We chose this cut-off value based on our previous report in which the most efficient TVQ cut-off values for detecting postthyroidectomy vocal-cord palsy and a postoperative lower-pitched voice were 35 and 25 respectively (16). We also regarded patients with any laryngeal nerve injury events during thyroidectomy or known laryngeal benign disorders to have an indication for a postoperative voice work-up to investigate the laryngeal status. In our current study, there were two subjects who experienced laryngeal injury and 14 with benign mucosal disease.
We determined that the PVST is an effective screening tool with which to detect surgery-related voice problems (lower-pitched voice, vocal-cord palsy) in the early postoperative period. A patient was considered to have a lower-pitched voice when the difference in the value was more than 12 Hz (22). The sensitivity and specificity of the PVST for detection of a lower-pitched voice were 66.7% and 51.2% respectively, demonstrating relatively low sensitivity. A total of 12 of 39 patients with a lower-pitched voice after surgery showed relatively low TVQ scores of <25. We also compared the voice pitch, sex, age, voice abuse history, and smoking status of patients with a low-pitched voice according to the TVQ score with a cut-off value of 25, and there were no significant differences among the parameters. This lack of difference seems to depend partially on individual characteristics and situations such as sensitivity, occupational and environmental characteristics, standard of living, and individual preferences regarding singing. It also seems to be partially due to the small number of patients with a low-pitched voice among the enrolled subjects in this study. The PVST was highly sensitive for the detection of patients with vocal-cord palsy; the sensitivity was 100% in the current study. No patients had preoperative vocal-cord palsy among the 10 patients with postoperative vocal-cord palsy. The recurrent laryngeal nerve was surgically sacrificed in one patient and shaved with a knife and mosquito clamps in one patient with laryngeal nerve invasion. Intraoperative nerve monitoring devices were not used in any subjects because we usually use them only in recurrent cases. Five injection laryngoplasties were performed in patients with significant glottic insufficiency. The other five patients with minimum glottis insufficiency underwent voice therapy and were followed up. All injection laryngoplasties were performed percutaneously under local anesthesia. As the biocompatible filler for injection, we used a hyaluronic acid derivative (Rofilan®; Rofil Medical International, Oroklini Cyprus) for temporary purposes. Half (5/10) of patients recovered their vocal-cord function within 6 months, and the others (5/10) had less than 6 months of follow-up.
Voice dysfunction seems to be one of the most significant complications after thyroidectomy and may have a negative impact on the patient's quality of life. Perioperative voice analysis in patients undergoing thyroidectomy seems necessary. The voice work-up comprises videostroboscopy, perceptual voice analysis, computerized acoustic analysis, physical examination, and counseling by a voice specialist. The mean cost of a specialized voice work-up is about US$203 for each patient (based on costs in our institution). If all 242 patients underwent specialized preoperative and postoperative voice work-ups, it would cost about US $98,320. However, when patients followed the protocol, only 36.4% were found to have an indication for both preoperative and postoperative voice work-ups. A total of 25.6% of patients could skip both the preoperative and postoperative voice work-ups, and 38.1% of patients had either a preoperative or postoperative voice work-up (Fig. 1). Therefore, the mean cost of a specialized voice work-up for all patients that need to undergo an evaluation would be about US $55,551, and US $42,768 would be saved among the 242 patients. Therefore, the cost savings effect of the PVST is expected to be 43.5%.
Based on the results of this study, we recommend that a preoperative voice work-up should be performed in patients with voice disorders, in professional voice users, and/or in patients with a high preoperative TVQ score (≥5). We also recommend that a postoperative voice work-up should be performed in patients with benign laryngeal mucosal disease, patients with any events of laryngeal nerve injury during thyroid surgery, and/or patients with a high postoperative TVQ score (≥25). Ideally, the full voice work-up should include fiber-optic laryngoscopic examination, videostroboscopic examination, perceptual voice analysis, and acoustic analysis. However, considering the high cost and limited availability of equipment, a minimum evaluation involving fiber-optic laryngoscopic examination and perceptual voice analysis should be performed by the laryngologist for selected patients.
Although voice quality is a concern for patients who have undergone thyroidectomy, voice work-ups are time-consuming, expensive, and require specific instruments and specialists. Thus, many patients are inclined to skip the voice work-up. For practical screening of voice problems after thyroidectomy, there is a need for a screening tool that a nonlaryngologist can utilize in a short period of time and easily interpret. The PVST is a simple and effective perioperative screening tool for thyroid surgeons to detect patients with voice problems in their routine outpatient clinic for early and appropriate referral to voice specialists.
Footnotes
Author Disclosure Statement
No competing financial interests exist.