
Abstract
Background:
The diagnostic limitations of thyroid fine-needle aspiration (FNA), such as the indeterminate category, can be partially overcome by molecular analyses. However, until now, rearrangements have only been detected in fresh FNA material and the number of follicular thyroid carcinomas (FTCs) was rather low in previous studies. We aimed at investigating the impact of point mutations and rearrangement detection in a set of routine air-dried FNA smears with a higher percentage of FTCs.
Methods:
RNA and DNA was extracted from 310 FNAs (164 indeterminate, 57 malignant, 89 benign) and corresponding formalin-fixed paraffin-embedded tissue (156 follicular adenomas [FAs], 32 FTCs, 44 papillary thyroid carcinomas [PTCs], 9 follicular variant PTCs, and 69 goiters). PAX8/PPARG and RET/PTC rearrangements were detected by qPCR, BRAF and RAS mutations by high-resolution melting PCR and by pyrosequencing.
Results:
Forty-seven mutations were detected in the FNAs: 22 BRAF, 13 NRAS, and 3 HRAS mutations, 8 PAX8/PPARG, and one RET/PTC-rearrangement. While the presence of a BRAF and RET/PTC mutation was associated with cancer in 100% of samples each, the presence of a RAS and PAX8/PPARG mutation was associated with cancer in only 12% and 50% of samples, respectively. In the indeterminate group 4 of 25 carcinomas were identified by molecular FNA screening, which increased the sensitivity from 67% (cytology alone) to 75% (cytology plus molecular screening).
Conclusion:
Molecular screening for point mutations and rearrangements is feasible in air-dried FNAs. Although the impact of detecting point mutations and rearrangements in FNAs has most likely been overestimated in previous studies, molecular FNA analyses improve presurgical diagnostics. The detection of BRAF mutations in FNA may improve the choice of surgery and postsurgical treatment. Further data are necessary to elucidate the true impact of detecting RAS and PAX8/PPARG mutations in FNAs. The inclusion of additional rare somatic mutations and miRNA markers might further improve the impact of molecular FNA diagnostics.
Introduction
T
Materials and Methods
Patients and samples
Air-dried FNA slides from 310 consecutive patients who underwent surgery for thyroid nodules at the Odense University Hospital from 1995 to 2009 were retrospectively included in this study. The patients were selected for the availability of formalin-fixed paraffin-embedded (FFPE) samples to be able to analyze these simultaneously. All FNAs were graded according to the 2006 American Thyroid Association (ATA) guidelines (17) by an experienced pathologist (A.K.). Cytological evaluation of the FNAs revealed 57 malignant, 164 indeterminate, and 89 benign samples. Moreover, all FNA slides were cytologically diagnostic and, in addition, the cellularity of the FNA smears was semiquantitatively graded according to the presence of thyroid epithelial cells: + (<20 cells), ++ (20–50 cells), and +++ (>50 cells). Histological evaluation of the corresponding FFPEs revealed 156 FAs, 32 FTCs, 44 PTCs, 9 fvPTCs, and 69 benign nodular goiters. The predominance of indeterminate FNA samples makes FTCs more likely. In addition, the selection of only those indeterminate FNAs that were verified by surgery is likely to further increase the probability of FTC. As Odense was iodine-deficient until ∼10 years ago, this may also have impacted on FTC numbers. The study was approved by the ethics committee of the Odense University Hospital and was conducted in accordance with the Danish law for scientific ethics committees. The authors were released from obtaining patient consent by the ethics committees because of using anonymous data.
DNA and RNA extraction from FNA smears
Routine air-dried, May-Grünwald Giemsa (MGG)–stained FNA smears were incubated in xylene for 4–5 days to remove the cover slips. Thereafter, RNA was extracted from the upper phase of the initial QIAzol:chloroform extraction step according to the recently published RNA extraction protocol (9); DNA was extracted from the lower phase according to the recently published DNA extraction protocol (16).
DNA and RNA extraction from FFPE slides
RNA was extracted from the FFPE slides according to the recently published RNA and DNA extraction protocols, respectively (9,16).
cDNA synthesis
cDNA was synthesized using the miScript Reverse Transcription Kit (Qiagen, Hilden, Germany) according to the manufacturer's protocol. In brief, 7.5 μL template RNA was added to a master mix consisting of 2 μL 5× miScript RT buffer and 0.5 μL miScript Reverse Transcriptase Mix and incubated for 60 minutes at 37°C. Subsequently, the miScript Reverse Transcriptase Mix was inactivated for 5 minutes at 95°C.
Detection of rearrangements by quantitative PCR
PAX8/PPARG, RET/PTC1, and RET/PTC3 rearrangements were detected in multiplex-qPCRs using the QuantiTect SYBR Green PCR kit (Qiagen), one primer pair amplifying an intron spanning 125 bp control fragment of PAX8 mRNA (exon 5–6) (for cDNA quality control), and one rearrangement-specific primer pair (Supplemantary Table S1; Supplementary Data are available online at
Detection of point mutations by high-resolution melting peak analysis
BRAF (codons 600/601), KRAS (codons 12/13), and NRAS (codon 61) point mutations were detected by real-time PCR and high-resolution melting (HRM), using primers flanking the mutations hotspots (Supplementary Table S2) and the LightCycler 480 High Resolution Melting Master chemistry (Roche, Mannheim, Germany) on a LightCycler 480 (Roche). Although several primer pairs were tested to establish a HRM-PCR to detect point mutations in codon 61 of HRAS, none of the PCRs gave reliable results. PCRs were processed through an initial denaturation at 95°C for 10 minutes followed by 55 cycles of a three-step PCR, including 3 seconds of denaturation at 95°C, a 12-second annealing phase at 58°C (NRAS, KRAS)/60°C (BRAF), and an elongation phase at 72°C for 10 seconds. Thereafter, an HRM curve was assessed from 75°C to 95°C with an increase of 0.02°C per second and 25 acquisitions per degree.
DNA from patient specimens known to carry BRAF, KRAS, and NRAS point mutations were used as positive controls in each analysis. Samples tested positive were subsequently analyzed by pyrosequencing on a PyroMark Q24 (Qiagen).
Detection of point mutations by pyrosequencing
Point mutations in BRAF, KRAS, and NRAS were detected by pyrosequencing using the therascreen BRAF Pyro Kit, therascreen NRAS Pyro Kit, and PyroMark KRAS Kit (all from Qiagen) according to the manufacturer's instructions. In brief, 5 μL of genomic DNA was amplified using template-specific PCR primers (including one biotin-labeled primer) and template-specific PCR conditions. Afterwards, the PCR products were immobilized on streptavidin sepharose beads and single-stranded DNA was prepared allowing subsequent annealing of the sequencing primer to the template DNA. Then, the primed single-stranded DNA was released from the streptavidin surface and transferred to a PyroMark Q24 (Qiagen) for pyrosequencing. HRAS point mutations were detected by pyrosequencing using self-designed primers (Supplementary Table S1) and the following PCR conditions: PCRs were processed through an initial denaturation at 95°C for 15 minutes followed by 45 cycles of a three-step PCR, including 20 seconds of denaturation at 95°C, a 30-second annealing phase at 64°C, and a 30-second elongation phase at 72°C followed by a final 5-minute extension phase at 72°C. Then, the PCR products were treated as described above.
Fluorescence in situ hybridization
For the detection of rearrangements of the PPARG gene and the RET gene, interphase-fluorescence in situ hybridization (I-FISH), either with a PPARG two-color break-apart probe or a RET two-color break-apart probe (PanPath, Budel, The Netherlands) was performed on FFPE tissue sections. With respect to PPARG and RET, respectively, both probes consist of a distal localized green fluorescent probe labeled with AlexaFluor488 and a proximal localized red fluorescent probe labeled with AlexaFluor555. With a few modifications, pretreatment of 4 μm tissue sections was performed as described previously for FFPE tissue sections (18). Digestion with a pepsin ready-to-use solution (DCS, Hamburg, Germany) was performed at 37°C. Incubation time for digestion was adapted for each tissue. Slides were each treated with 15 μL of a break-apart probe. Codenaturation was performed on a ThermoBrite (Abbott Molecular, Wiesbaden, Germany) for 5 minutes at 85°C followed by overnight hybridization in a humidified chamber at 37°C. Posthybridization was performed at 39°C or 42°C for 2 minutes in 0.4× SSC/0.3% NP-40. Interphase nuclei were counterstained with DAPI (0.75 μg/mL) and slides were examined with an Axioskop 2 plus fluorescence microscope (Carl Zeiss, Göttingen, Germany). Images were captured with a high performance CCD-camera (Visitron Systems, Puchheim, Germany) and were edited with FISH View (Applied Spectral Imaging, Migdal HaEmek, Israel). Two hundred nonoverlapping nuclei from different (at least four) areas of the tumor were scored. Cutoff values were calculated for each probe. The cutoff values were defined as means plus three standard deviations (M+3SD) of the number of nuclei with abnormal signal patterns in control specimens (19). As control specimen tissue, sections of two differentiated thyroid carcinomas without any evidence for a PPARG and a RET rearrangement, respectively, were used. For calculation of the cutoff values, the signal patterns of 200 nonoverlapping nuclei of the control specimen were determined independently by two different observers. A normal nonaberrant nucleus is characterized by two fusion signals, i.e., two colocalized red and green signals (2RG), both for the PPARG and the RET break-apart probe. A PPARG as well as a RET rearrangement is indicated by one colocalized signal along with a single red and a single green signal (1R1G1RG).
Statistics
Sensitivities, specificities, positive predictive values (PPV), and negative predictive values (NPV) were calculated as follows:
In the comparisons cytology versus histology, molecular FNA analysis (mFNA) versus histology, and for the comparisons of cytology and mFNA versus histology, histology is the gold standard and a mutation-negative FA is considered as true negative, while a mutation-positive FA is considered false positive. To investigate the concordance of the mutation analysis for FNA and the corresponding FFPE samples, mFNA was compared to molecular FFPE analysis (mFFPE). Therefore, in this comparison, mFFPE is the gold standard and the decision solely depends on whether a mutation present in the FFPE sample was detected in the corresponding FNA sample or not.
Results
Inadequate PCR product/detected mutations
The percentage of samples that could not be analyzed due to inadequate PCR products varied depending on the source of DNA (FNA or FFPE material) and the mutation screened (BRAF, NRAS, HRAS, KRAS, PAX8/PPARG, RET/PTC). In the FFPEs we observed inadequate PCR products on average at a rate of 0.4% per point mutation screening and 7.1% per rearrangement screening. In the FNAs the percentage of samples, with inadequate PCR products per point mutation screening was, on average, 8% and per rearrangement screening 3.9%. All the FNAs and FFPEs characterized by at least one inadequate PCR and that were mutation-negative in all the other screenings were classified not detectable (ND). Interestingly, we observed a significant difference in the number of ND samples depending on the cellularity of the FNA slides (+: 48% ND, ++: 21% ND, and +++: 11% ND, χ2 p value=2.2×10−6). FNAs and FFPEs that were mutation-positive in at least one analysis were classified mutation-positive. Only FNAs and FFPEs that were mutation-negative in all screenings were classified as wild-type (WT). FNAs and FFPEs classified as ND were not considered in the calculation of sensitivity and specificity.
Forty-seven mutations were detected in the FNAs: 22 BRAF-, 13 NRAS-, and 3 HRAS-mutations, 8 PAX8/PPARG-, and 1 RET/PTC-rearrangement. 80 mutations were detected in the corresponding FFPEs: 34 BRAF-, 27 NRAS-, and 9 HRAS-mutations, 8 PAX8/PPARG-, and 2 RET/PTC- rearrangements. Four of the 8 PAX8/PPARG rearrangements detected in the FFPEs were verified by FISH analysis (Fig. 1). The remaining 4 PAX8/PPARG rearrangement positive FFPEs could not be analyzed by FISH due to low quality or signal intensity in the FISH experiments. Also, while one RET/PTC rearrangement could be verified by FISH analysis (Fig. 1), the second RET/PTC-positive FFPE was rearrangement-negative in the FISH analysis. In 87.8% the mutation found in the FNA could be confirmed in the FFPE, while 71.7% of the mutations found in the FFPE were detected in the FNA. The correlation between cytology, histology, mFNA, and molecular FFPE analyses (mFFPE) are shown in Figure 2. While the presence of a BRAF and RET/PTC mutation was associated with cancer in 100% of samples each, the presence of a RAS and PAX8/PPARG mutation was associated with cancer in only 12%, and 50% of samples, respectively (Fig. 2).
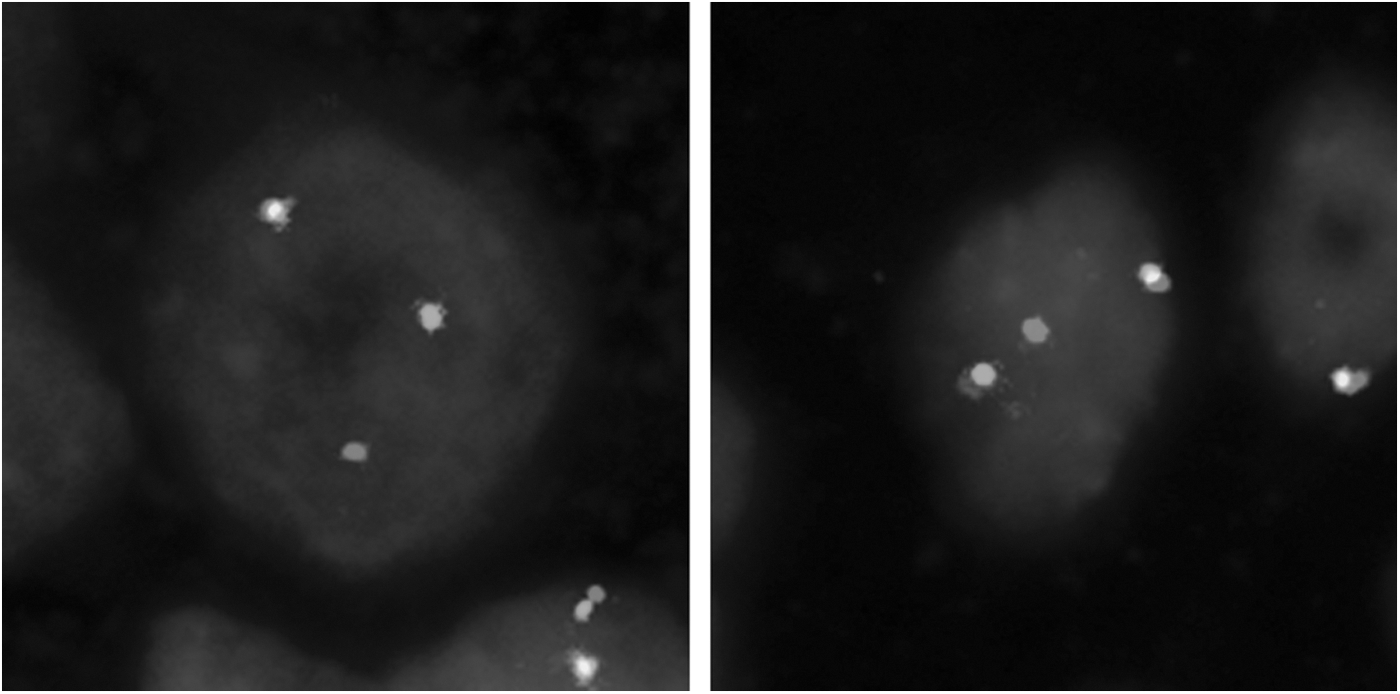
Verification of a PAX8/PPARG (left) and a RET/PTC (right) rearrangement detected by multiplex-qPCR in two formalin-fixed paraffin-embedded (FFPE) samples by fluorescence in situ hybridization (FISH).

Correlation of cytology, molecular FNA smear analysis (mFNA), histology, and molecular FFPE analysis (mFFPE) for the 310 FNA and FFPE samples. PTC, papillary thyroid carcinoma; fvPTC, follicular variant PTC; FTC, follicular thyroid carcinoma; WT, wild-type; FA, follicular adenoma; FNA, fine-needle aspiration; nd, not detectable due to inadequate polymerase chain reaction (PCR).
Cytology versus histology
Cytology revealed 57 malignant, 164 indeterminate, and 89 benign results. All 57 cytologically malignant samples were carcinomas at histology (42 PTCs, 10 FTCs, and 5 fvPTCs). The final histological classification of the 164 cytologically indeterminate samples revealed 2 PTCs, 19 FTCs, 4 fvPTCs, and 139 FAs, while the final histological classification of the 89 cytologically benign samples revealed 3 FTCs, 17 FAs, and 69 goiters (Fig. 2). As shown in Table 1, these data result in a sensitivity of 67.1%, a specificity of 100%, and a positive predictive value (PPV) and negative predictive value (NPV) of 100% and 88.9%, respectively.
The comparison of mFNA and mFFPE analysis results gives a measure of the concordance of the mutation analysis between FNA and corresponding FFPE samples.
Mutation-positive adenomas considered as false positives.
Mutation-positive adenomas considered as true positives.
mFNA, molecular fine-needle aspiration smear analysis; mFFPE, molecular formalin-fixed paraffin-embedded analysis; PPV, positive predictive value; NPV, negative predictive value.
mFNA versus histology
mFNA revealed 47 mutations in total. Twenty-two BRAF mutations were detected. Of these lesions, 20 were PTCs and 2 were fvPTCs on histology. Furthermore, 13 NRAS mutations were detected in the FNAs representing 12 FAs, and 1 FTC on final histology. In addition, 3 HRAS mutations could be detected in the FNAs (1 FTC and 2 FAs). Eight PAX8/PPARG rearrangements were detected in the FNAs corresponding to 3 FTCs, 1 fvPTC, and 4 FAs on final histology. Only one RET/PTC rearrangement was detected in the FNAs corresponding to a PTC on final histology (Fig. 2). Two hundred six FNAs were mutation-negative, representing 9 PTCs, 4 fvPTCs, 24 FTCs, 114 FAs, and 55 nodular goiter samples on final histology (Fig. 2). These data result in a sensitivity of 43.9%, a specificity of 90.4%, and a PPV and NPV of 61.7% and 82%, respectively (Table 1).
Cytology and mFNA versus histology
In addition to the 57 cytologically malignant samples, mFNA detected 21 mutations (12 NRAS, 3 HRAS, and 6 PAX8/PPARG) in the 164 cytologically indeterminate samples representing 4 FTCs, and 17 FAs, and 1 NRAS mutation in the cytologically benign group representing 1 FA (Fig. 2). One hundred twenty FNAs were mutation-negative in the indeterminate group representing 2 PTCs, 2 fvPTCs, 14 FTCs, and 102 FAs on final histology. In the benign group 69 FNAs were mutation-negative, representing 2 FTCs, 12 FAs, and 55 goiters on final histology. Based on these data, the combination of cytological evaluation and mFNA allowed the detection of four additional carcinomas in the indeterminate category, while 18 carcinomas could not be identified, revealing a sensitivity of 75.3%, a specificity of 90.4%, and a PPV and NPV of 77.2% and 89.4%, respectively (Table 1). In an additional analysis we considered mutation positive FAs as (pre-)malignant tumors and thus as true positives. Based on this assumption, the sensitivity is 79.8%, the specificity is 100%, and the PPV and the NPV is 100% and 89.4%, respectively (Table 1).
mFNA versus mFFPE
The direct comparison of mFNA and mFFPE results was not of diagnostic relevance in this retrospective study, but gives a measure of the concordance of the mutation analyses between FNA and corresponding FFPE samples and shows the efficiency of analyzing point mutations and rearrangements in routine air-dried FNA smears. Forty-seven mutations were detected in the FNAs; 44 of these 47 mutations could be confirmed in the FFPEs, while 3 corresponding FFPEs were mutation-negative. Two hundred six FNAs were mutation-negative. While the molecular screening of the corresponding FFPEs confirmed the mutation-negative result in 181 FFPEs, 14 FFPEs were mutation-positive and 11 FFPEs were ND. This corresponds to a sensitivity of mFNA of 75.9%, a specificity of 98.4%, and a PPV and NPV of 93.6% and 92.8%, respectively.
Discussion
Previous studies have shown the diagnostic potential of screening a panel of point mutations and rearrangements in fresh or deep-frozen FNA material from the thyroid in order to differentiate benign from malignant, especially in the cytologically indeterminate group (10 –14). However, in our opinion, molecular screening on FNA material from the same air-dried FNA smear, which is used for cytological analysis, would offer major advantages (8). Moreover, in most of the panel studies (10 –14) the cytologically indeterminate group also included cytologically suspicious samples, contributing a high number of PTCs in contrast to a low number of FTCs. This might result in an overestimation of the mFNA sensitivity. Therefore, the goal of our study was (i) to use air-dried FNA samples for molecular screening, (ii) to analyze a cytologically indeterminate group containing a higher number of FTCs to avoid an overestimation of mFNA sensitivity, and (iii) to compare our results with those of previously published panel studies (10,12 –14).
The sensitivity of 67% and specificity of 100%, obtained by cytology alone, reflects the high experience of our pathologist. By combining cytological evaluation and mFNA, the sensitivity improved to 75%, while the specificity remained at 90%. What are the reasons for this? To answer this question this study also investigated corresponding FFPE samples. The direct comparison of mFNA and mFFPE, giving a measure of the concordance of the mutation analysis between FNA and corresponding FFPE samples, revealed a sensitivity and specificity of 76% and 98%, respectively. Therefore, the low sensitivity (44%) and specificity (90%) of the mFNA in comparison to histology can only partly be attributed to methodological problems of not detecting mutations in the FNA samples. In addition to the high ND rate of low-cellularity FNA smears, which is one reason for the discrepant number of detected mutations in FNA smears, another reason for the low sensitivities might be tumor heterogeneity. Recently, a pyrosequencing approach has reported percentages of mutant BRAF alleles from 5.1% to 44.7% (20). Tumor heterogeneity has been reported for RET/PTC rearrangements by FISH (21,22). This explains why the mutation screening of the FFPE sample may in some cases reveal a positive result, while the mutation screening of the FNA sample is negative. Potential reasons for this discrepancy could be aspiration of a mutation negative subpopulation, or dilution of mutation positive cells by mutation negative cells during the aspiration process, resulting in a lower sensitivity. Tumor heterogeneity could also explain the opposite finding, i.e., the detection of a mutation in the FNA sample, while the mutation screening of the corresponding FFPE sample is mutation negative. In this situation, the aspiration of a mutation positive subpopulation can coincide with a dilution of mutation-positive cells by mutation-negative cells in the FFPE sample.
In our opinion, the two main reasons for the low sensitivity of the mFNA compared to histology is the fact that only 8 of 32 (25%) analyzed FTCs harbored a mutation as could be shown by mFFPE (5 of these 8 FTCs were detected by mFNA), while the observed percentage of mutation-positive FAs in the mFNA was rather high (18/156; 12%) resulting in a high number of false positives and hence a lower specificity. Both of these findings are in contrast to the outcomes of the panel studies published before, with lower numbers of FTCs/FAs (12,13) or no FTCs (10,14) analyzed, and no (14) or only low numbers of RAS mutations in FAs [2% in Nikiforov et al. (13)]. In our study, these two findings are responsible for the lower diagnostic benefit of the molecular FNA screening in the indeterminate cytology group. Only 4 of 19 FTCs (21%) or 4 of 25 carcinomas (16%) could be identified by molecular FNA screening. All four mutation positive FTCs and also the mutation-negative FTCs are minimally invasive FTCs.
If mutation-positive FAs are considered as false positives, our sensitivity of 16% is much lower in comparison with the previously published panel studies (10,12 –14). This cannot only be explained by the reasons mentioned before. An additional reason seems to be the composition of the sample sets. While our indeterminate group contained 1.2% diagnosed as PTCs on final histology, the percentage was 6.4–55.8% in the other panel studies since the indeterminate group also contained cytologically suspicious samples in at least in two studies (10,12) (Table 2). Moreover, the percentage of FTCs was much higher (11.6%) in our indeterminate group in comparison to 0–7.7% in the other panel studies (10,12 –14). These differences directly influence the outcome of the mFNA, since the detected mutation rates in PTCs are much higher [∼60% in Nikiforov et al. (12), 81% in Cantara et al. (10), and 70% in our study] compared to FTCs [50% in Nikiforov et al. (12), 0% in Cantara et al. (10), and 25% in our study]. Also, while the occurrence of a BRAF mutation is highly specific for PTCs, the occurrence of RAS and PAX8/PPARG mutations is much less specific for FTCs, since these mutations can also be found in FAs. Therefore, the main reason for the discrepant sensitivities and specificities is most likely an overestimation of both sensitivity and specificity in at least some of the previous panel studies due to the inclusion of suspicious samples in the indeterminate group with a higher number of frequently mutation positive PTCs and a low number of frequently mutation negative FTCs leading to an increased sensitivity (10,12).
First, the table depicts the diverse composition of the indeterminate sample sets in the different studies. In relation to this, sensitivities and specificities vary between these studies. However, the sensitivities and specificities of the studies are comparable when reducing the indeterminate sample set to FTCs and FAs. Finally, sensitivities and specificities are given for the different studies when analyzing the whole data sets comprising malignant, indeterminate, suspicious, and benign samples.
The indeterminate groups of Cantara et al. (2010) and Nikiforov et al. (2009) also contain suspicious samples.
Mutation positive adenomas considered as false positives.
Mutation positive adenomas considered as true positives.
N/A, the respective values cannot be calculated; ?, the precise composition of the sample set is not available; PTCs, papillary thyroid carcinomas; FTCs; follicular thyroid carcinomas; fvPTCs, follicular variant papillary thyroid carcinomas; FAs, follicular adenomas; mFNAs, molecular fine-needle aspiration analysis.
As mentioned above, RAS and PAX8/PPARG positive FAs have rarely been reported in previous molecular FNA studies (12 –14). They might be preinvasive FTCs or tumors for which capsular or vascular invasion was not detected by histological examination. This assumption is also supported by the fact that two of four PAX8/PPARG-positive FAs were characterized by a microfollicular morphological pattern. Similar to the findings with PAX8/PPARG rearrangements, Nikiforov et al. showed that the presence of a RAS mutation in a FNA confers an 88% probability of malignancy in the RAS-positive cases (12). Moreover, several studies suggest that RAS mutations are involved in malignant transformation and tumor dedifferentiation (23 –26). In support of this, in vitro studies have shown that mutant RAS initiates cell proliferation, promotes chromosomal instability, and thereby may predispose to a more malignant phenotype (27,28). Interestingly, it has recently been shown that an increasing thyroid nodule size larger than 2 cm is associated with an increased risk of FTCs suggesting that the histological criteria of FTC (vascular and/or capsular invasion) may only occur once a nodule grows beyond a certain size, even if oncogenic mutations are present at its inception (29). This finding supports the hypothesis that histologically benign nodules harboring RAS or PAX8/PPARG mutations may be best characterized as carcinoma in situ (13). Moreover, transgenic mouse models carrying RAS mutations have been shown to develop thyroid carcinomas (30,31). Consequently, RAS or rearrangement positive (histologically benign) nodules may well be a subgroup of histologically benign nodules with faster growth (32) and a higher likelihood of requiring therapy during further follow-up. Thus, the 14 histologically benign RAS positive and the 4 histologically benign PAX8/PPARG-positive FAs are very likely not false positives. Hence, we considered mutation-positive but histologically benign samples as (pre-)malignant and thus as true positives. This results in a sensitivity of 80% and a specificity of 100% of our mFNA screening (Table 1).
Although the prevalence of BRAF mutations is associated with a high geographical variability (the prevalence of BRAF mutations is considerably higher in countries with a high iodine intake), the preoperative BRAF mutation testing of FNA specimens can more reliably define the extent of the initial surgery and also the medical management of PTCs: the occurrence of the BRAF mutation in the FNAs was found to be strongly predictive for extrathyroidal extension, capsular invasion, and lymph node metastasis (33). The BRAF mutation was strongly associated with PTC persistence and recurrence (33). The BRAF V600E mutation is an independent prognostic factor for a poor outcome of patients with low-risk intrathyroidal PTCs (34). A meta-analysis has shown an association of the BRAF V600E mutation with poor prognostic features of PTC (35). It follows that BRAF can be of considerable diagnostic value for cytologically malignant or suspicious nodules since the preoperative knowledge of a BRAF mutation may guide in defining the optimal extent of initial thyroid surgery (total thyroidectomy versus lobectomy), may help to decide on performing a prophylactic central neck dissection, and aid in a more appropriate planning of the postsurgical therapy (33).
In conclusion, we have shown that molecular screening for point mutations and rearrangements is feasible in routine air-dried FNA smears, offering several advantages over obtaining additional fresh FNA material. The same indeterminate material analyzed by cytopathology is analyzed for point mutations and rearrangements. This obviates the need to prepare additional FNA material for RNA preservation or to store FNA material until completion of cytological diagnosis, which would then reveal samples with indeterminate cytology that would require molecular analysis. It also obviates the need for a second FNA for molecular diagnostics. Thereby, the burden to the patient and society is reduced, specifically because there is no need for parallel morphologic and molecular diagnostics, and less diagnostic surgeries. Although the impact of detecting point mutations and rearrangements in FNAs has most likely been overestimated in previous studies, mFNA improves presurgical diagnostics. The detection of BRAF mutations in FNA may prompt primary total thyroidectomy instead of lobectomy followed by completion thyroidectomy. Further data are necessary to elucidate the true impact of detecting RAS and PAX8/PPARG mutations in FNAs. Theoretically, the inclusion of additional rare somatic mutations and miRNA markers might further improve the clinical impact of molecular FNA diagnostics.
Footnotes
Acknowledgments
This research was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico do Brasil (CNPq), Brazil, by a PhD scholarship to C.F. (290023/2009-2), by a DFG (ES162/4-1) and a Krebshilfe (109994) grant to M.E., and by an unrestricted grant by the Novo Nordisk Foundation to L.H. R.P. is supported by DFG and Krebshilfe. M.S. was funded by Leipzig Research Center for Civilization Diseases (LIFE), University of Leipzig. LIFE is funded by means of the European Union, by the European Regional Development Fund (ERDF), and by means of the Free State of Saxony within the framework of the excellence initiative.
Author Disclosure Statement
All authors declare that no competing financial interests exist.