
Abstract
Background:
Ultrasound-guided thermal laser ablation (LA) is a nonsurgical technique that has been proposed, but not fully assessed, for papillary thyroid microcarcinoma (PTMC) treatment. The objectives of this study were to evaluate the clinical feasibility of LA on PTMC as a primary treatment and to prove histologically the absence of residual viable tumor after LA procedure.
Methods:
Three patients with a Thy 6 diagnosis at fine-needle aspiration cytology with a single PTMC smaller than 10 mm volunteered after full explanation of the protocol. At ultrasound examination, patients had no extrathyroid extension and no evidence of lymph node metastasis. Patients underwent percutaneous ultrasound-assisted LA of the PTMC in the operating room under general anesthesia. One 300 μm plane-cut optic fiber was inserted through the sheath of 21G Chiba needle, exposing 5 mm of the nude fiber in direct contact with tumor tissue, and connected with a laser source operating at 1.064 μm with 3 W output power. Total energy delivery was 1800 J. The surgeon directly started a standard total thyroidectomy. During surgical inspection, no remarkable laser sign was observed in the muscles, the perithyroidal tissues, or the recurrent laryngeal nerves.
Results:
Conventional histology showed destructured and carbonized tissue. Lack of vitality was demonstrated by complete loss of TTF1 and antimitochondria antibody expression in the whole ablated area and in the rim of normal tissue surrounding the tumor. BRAF V600E mutation was detected in cases 1 and 2. Furthermore, in cases 2 and 3, incidental papillary microfoci were found. A lymph node micrometastasis (200 μm) was observed in case 2.
Conclusions:
This study demonstrates that percutaneous LA is technically feasible for complete PTMC destruction. Now, LA may be useful in selected patients with PTMC, either when the surgeon or a patient refuses surgery, or when the patient is at high risk for an operation. LA may become a primary choice of treatment for PTMC only if future new knowledge would permit preoperative recognition of multifocality and lymph node metastasis.
Introduction
U
The aims of this study were to evaluate the clinical feasibility of LA on PTMC as a primary treatment and to prove histologically the absence of residual viable tumor after the LA procedure.
Materials and Methods
The study protocol was approved by the Ethics Committee of Arcispedale Santa Maria Nuova & Clinical Cancer Research Institute (IRCCS), Reggio Emilia, Italy.
Three patients diagnosed by fine-needle aspiration cytology as positive for malignancy consistent with papillary thyroid carcinoma (category Thy 6 according to the Bethesda fine-needle aspiration cytology classification system) (7) were enrolled in the study after a full explanation of the protocol. The cut-off for enrollment was a positive fine-needle aspiration cytology for papillary thyroid cancer with US evidence of only one nodule 10 mm or less in greatest dimension, and no other evidence of tumor in the thyroid gland or neck. In this feasibility study, we arbitrarily considered that three PTMC patients with similar clinical characteristics and identical cytological features would have been a sufficient number to demonstrate cancer destruction. Among the PTMC subjects, we selected patients in whom the whole tumor was surrounded by normal thyroid tissue as judged by high-resolution US. Among four consecutive suitable patients, one patient refused and three patients accepted giving written informed consent. The subjects were euthyroid and had normal serum calcitonin levels.
All patients underwent percutaneous LA of the PTMC in the operating room under general anesthesia immediately before surgical removal of the thyroid gland. One 300 μm plane-cut optic fiber was inserted through the sheath of a 21G Chiba needle, exposing 5 mm of the nude fiber in direct contact with tumor tissue. The optic fiber was connected with the laser source, a continuous-wave, solid-state laser operating at 1.064 μm wave length. The output power was 3 W, and the total energy delivery was 1800 J. The amount of watts and joules delivered was chosen on the basis of our and other authors' experience, in order to deliver an energy able to destroy an area larger than the lesional volume (1,2). During LA, real-time US showed the vapor from the tissue as an echogenic area enlarging progressively until it filled the tumor area. Percutaneous US-guided LA was performed by an operator, an assistant echographer, and a nurse. The standard time taken to complete LA was 10 min. No immediate adverse effect was observed. After LA completion, the surgeon directly started a standard total thyroidectomy. During surgical inspection, no remarkable alterations were observed in the muscles, the perithyroidal tissues, or the recurrent laryngeal nerves.
Subsequent to surgery, the thyroid glands were submitted for histological evaluation. After an overnight 10% buffered formalin fixation, the resected thyroid glands were sliced at 1 cm thickness and routinely processed in toto. The paraffin blocks with the ablated areas were then serially sectioned. We did not use whole-mounted blocks.
The specimens were stained with hematoxylin and eosin. Sections were photographed and measured with a Nikon digital sight DS-L1 camera system on a Nikon Eclipse 50i microscope (Nikon).
Tumor and surrounding parenchymal cellular vitality analysis were evaluated by immunohistochemistry on selected paraffin-embedded blocks using both thyroid transcription factor-1 (TTF-1; clone 8g7g3/1; Roche) and antihuman mitochondria antibodies (clone 113-I; Biogenex). TTF-1 positivity was defined by nuclear labeling, while antihuman mitochondria antibody reactivity corresponded to a granular cytoplasmic staining.
The presence of the V600E mutation in the BRAF gene was determined preoperatively by DNA sequencing on selected cytological slides. The slides used for the molecular analysis were selected, after Papanicolaou staining and microscopy examination, by one of the authors (S.P.) to ensure an appropriate content of neoplastic cells (>90% of total cells). This selection should guarantee the reliability of the genetic test. Genomic DNA was extracted using the Biostic formalin-fixed and paraffin-embedded tissue DNA isolation kit (Mobio Laboratories) according to manufacturer's instructions. Polymerase chain reactions for exon 15 of the BRAF gene were performed as previously described (8). Briefly, polymerase chain reaction products were purified using the polymerase chain reaction purification kit (Qiagen) and sequenced using the Genome Lab DTCS-quick start kit (Beckman Coulter) according to manufacturer's instructions. The DNA sequence was performed using a CEQ 8000 Genetic Analysis Systems (Beckman Coulter).
Results
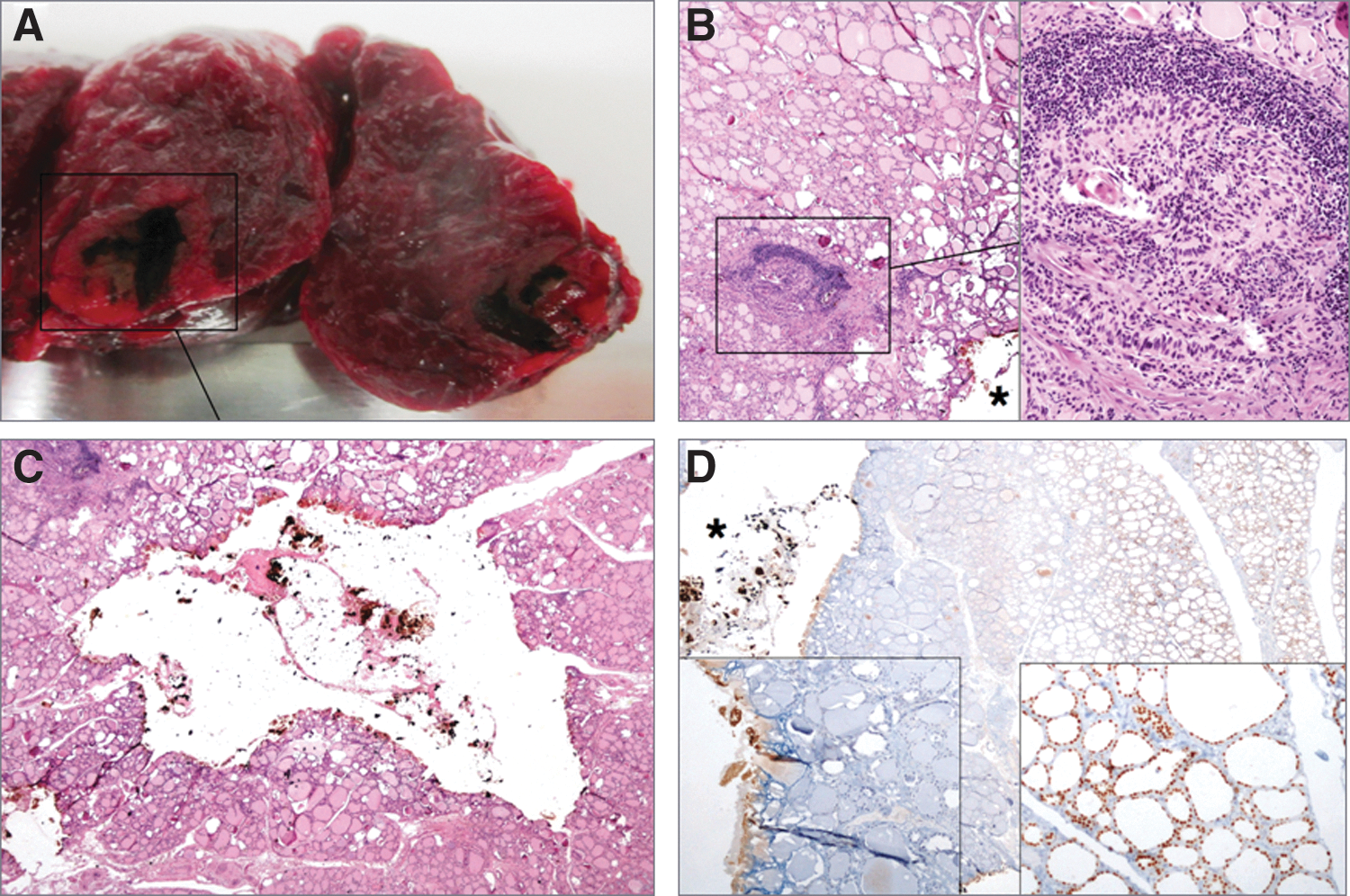
The features of clinical cases, with gross/histologic/BRAF findings, are shown in Table 1. In all patients, US characteristics were suggestive of malignancy. The macroscopic examination of the resected specimens in all cases showed a well-defined brownish area (Fig. 1A) measuring 5 mm across. In cases 2 and 3, the lesion was cavitated and centrolobular, while in case 1, the ablated zone was eccentric in the lobe and was detectable, at gross examination, as a subcapsular thin empty space.
Tissue sample treated by ablation: gross, microscopic, histological, and immunohistochemical examinations.
AJCC, American Joint Committee on Cancer.
On histology, the cavitations in cases 2 and 3 contained a small amount of brownish debris corresponding to carbonized tissue (Fig. 1B), which is the expected result in human thyroid tissue after an LA procedure (9).
The histological features were comparable in all three cases; that is, the neoplastic tissue around the cavitation showed typical changes of thermal damage, including cell shape distortion or cell shrinkage and nuclear chromatin condensation. The cytoplasm and occasional psammoma bodies were still identifiable (Fig. 1C). On higher-power view, cases 2 and 3 were found to have incidental papillary microfoci far from the ablated zone. In case 2, a micrometastasis (200 μm in the greatest axis) was observed in 1 perithyroidal lymph node out of 3 resected lymph nodes. There was no continuity between intrathyroidal PTMC foci and the lymph node metastasis. All cases were staged according to the AJCC Cancer Staging Manual, 7th edition (10).
The signs of thermal damage included a 2–3 mm rim of normal tissue around the tumor that faded away at the border of the cavitation. In the residual thyroid tissue, the follicular architecture was maintained, and there was no extrafollicular colloid spillage or hemorrhage. No vascular invasion was noted. A mild lymphocytic thyroiditis was observed in all thyroid tissues.
In all cases, there was complete loss of TTF-1 and antimitochondria antibody staining in the whole ablated area and in the rim of normal tissue surrounding the tumor (Fig. 1D). In contrast, the immunoreactivity for TTF-1 and antimitochondrial antibodies was easily detectable in nontargeted tissue. This demonstrates that the ablated neoplastic tissue was irreversibly damaged. The BRAF V600E mutation was detected in cases 1 and 2, but not in case 3.
Discussion
Surgical treatment is the current management for papillary thyroid cancer. The 2009 American Thyroid Association Guidelines suggest that the initial surgical procedure should be a near-total or total thyroidectomy for patients with thyroid cancer >1 cm. Thyroid lobectomy alone may be sufficient treatment for small (<1 cm), low-risk, unifocal, intrathyroidal papillary carcinomas in the absence of prior head and neck irradiation or radiologically or clinically involved cervical lymph node metastasis (11). On the basis of 2009 American Thyroid Association guidelines, our patients might have been candidates for lobectomy. PTMC is a low-grade, small-burden tumor. A clinical trial by Japanese authors offered surgery or observation to a large series of PTMC patients (12). Out of 1395 PTMC patients, 340 underwent observation and 1055 underwent immediate surgery. During follow-up, 109 patients were referred to surgery for various reasons. The tumor–node–metastasis characteristics of these patients were not different from those of patients who preferred immediate surgery (12).
The aim of this study was to evaluate the clinical feasibility of percutaneous LA as an alternative therapeutic strategy on PTMC by means of accurate pathological and immunohistochemical analysis. Many researchers in the field of radiofrequency ablation have obtained good results with this method (13,14), as opposed to vital dye analyses such as the nicotinamide adenine dinucleotide diaphorase, which requires fresh frozen tissue and may underestimate the extent of the necrotic areas with false-negative or false-positive results (15 –17). Immunohistochemical techniques rely on the binding between an antigen and its specific primary antibody. If the tissue antigen has been destroyed by laser-light energy, the primary antibody cannot recognize its epitope and the immunohistochemical staining is negative. If the denaturation of the proteins and the damage of the epitopes are widespread throughout the cell, either in the nucleus or in the cytoplasm, one can presume that the cell has lost its vitality.
The application of localized heating by laser on thyroid tissue makes it possible to produce histologically confirmed irreversible cellular damage (9). TTF-1 is a nuclear DNA-binding protein that is commonly used in surgical pathology for histological confirmation of either a thyroid- or lung-derived tumor (18). The antibody directed to human mitochondria recognizes a 60 kDa mitochondrial antigen and has a high sensitivity and specificity for mitochondria (19). In our cases, the nuclear reactivity for TTF-1 and the cytoplasmic reactivity for the antibody to human mitochondria were completely eliminated in the ablated area. We can therefore conclude that the ablated neoplastic tissue was irreversibly damaged.
Patients are presently followed longitudinally similar to standard patients who underwent total thyroidectomy (11). So far, in a year after LA plus total thyroidectomy, there is no evidence for residual or recurrent thyroid cancer. There is no study that compared the quality of life in patients who are submitted to LA versus patients submitted to surgery. A limitation of the LA approach is that US examination does not allow to detect very small tumor foci within the thyroid or in locoregional lymph nodes. However, this study demonstrates that percutaneous LA is a technically feasible option for the complete destruction of cytology-proven PTMC. LA might have similar advantages and limitations as a thyroid lobectomy, and result in the same long-term surveillance management with its associated costs.
Two issues should be discussed in the use of LA for the treatment of PTMC. First, multifocality and micrometastases cannot be detected without histological examination. Indeed, the microcarcinomas in the present study were multifocal in cases 2 and 3. The same risk of overlooking other very tiny microcarcinomas in the contralateral lobe occurs if the patient will undergo lobectomy. Also, a tiny micrometastasis was found in case 3 in a perithyroidal lymph node. Second, tumor aggressiveness is unpredictable despite the fact that many molecular studies have addressed this issue (20). Although the presence of a BRAF V600E mutation was claimed to be a major prognostic marker in metastatic PTMC (21), BRAF V600E mutation positivity was not associated with the development of distant metastases or with fatal outcomes in papillary thyroid cancer (8). In 2 out of 3 of our patients, a BRAF mutation was found in our three cases, but no correlation with histological prognostic features was noted.
In conclusion, this study proves that percutaneous LA is technically feasible for complete PTMC destruction. Now, LA may be useful in selected patients with PTMC, either when the surgeon or a patient refuses surgery, or when the patient is at high risk for an operation. LA may become a primary choice of treatment for PTMC only if future new knowledge would permit preoperative recognition of multifocality and lymph node metastasis.
Footnotes
Acknowledgment
The authors thank Dr. Giovanni Apolone, Director of the Clinical Cancer Research Institute, for his valuable advice.
Author Disclosure Statement
We declare that we have no conflict of interest.