
Abstract
Background:
Few studies have systematically examined the immune cells that infiltrate thyroid tissue at the time of the onset of Graves' disease (GD). The role of viruses in the pathogenesis of autoimmune thyroid diseases is controversial. The present study analyzed inflammatory responses with respect to signs of virus infection.
Methods:
Thyroid tissue was obtained from 22 patients with newly diagnosed and untreated GD, 24 patients with chronic GD, and 24 controls. Inflammation was assessed by immunostaining for CD4+ and CD8+ T cells, plasma cells (CD138+), and plasmacytoid dendritic cells (PDCs). The production of interferon-inducible myxovirus resistance protein A (MxA) was analyzed as a sign of virus infection.
Results:
The degree of thyroid inflammation and fibrosis was significantly higher in both patient groups compared with that in controls. The number of CD4+ T cells and plasma cells (activated B cells) was significantly higher in both patient groups. CD8+ cells were only present in patients with chronic disease. MxA expression and the number of PDCs increased only in patients with newly diagnosed GD. There was a strong positive correlation between the number of PDCs and the number of MxA+ leucocytes.
Conclusion:
The increase in CD8+ T cells during the chronic stage of GD suggests that they may play a role in progression of the autoimmune process from early to chronic thyroiditis. Upregulation of MxA expression during the early stages of the disease, and the positive correlation between the number of PDCs and the number of MxA+ leucocytes, suggests that activated PDCs secrete type I IFNs at the lesion site, possibly in response to viral infection.
Introduction
A
The etiopathogenesis of GD disease is still not clear. The concordance rate of 30–40% observed in monozygotic twins indicates that genetic factors are important (4 –6). However, this rather low concordance rate also suggests that external factors are important. Although definitive studies are lacking, there is a growing body of evidence suggesting that viruses play a role in autoimmunity (7 –10) and in the development of AITD (11).
Most previous studies of GD were conducted on peripheral blood or thyroid tissues obtained from treated patients. However, direct examination of thyroid tissue in the early stage of disease is of paramount importance if we are to identify the factors underlying disease onset and progression. Such studies are scarce and involve very few patients.
We previously reported that enteroviruses (EVs) were more common in the thyroid tissue of GD patients than in that of controls (12). Thyroid epithelial cells express a variety of molecules involved in antiviral responses (13). The interferon (IFN) family of cytokines is a key component of the innate immune response and forms the first line of defense against viral infection (14,15). Plasmacytoid dendritic cells (PDCs) produce large amounts of type I IFNs when stimulated by viruses (16). Type 1 IFNs induce the synthesis of myxovirus resistance protein A (MxA protein) (15), and the number of PDCs correlates with the number of cells expressing this protein in patients with various disorders (17,18).
In the present study, we conducted a detailed immunohistochemical analysis of the inflammatory cells that infiltrate the thyroid tissue of patients with early-onset untreated GD or chronic GD, focusing on cells that play a role in the response to viral infection. In situ detection of MxA was used both as a surrogate marker for type I IFNs and as a general “viral footprint” marker in the thyroid tissue.
Materials and Methods
All study subjects were recruited at Oslo University Hospital, Aker, Norway. Twenty-two consecutive patients with newly diagnosed GD, with clinical symptoms of hyperthyroidism and high titers of TRAb, were included. In addition, thyroid tissue samples were obtained from 24 patients with chronic GD who underwent total thyroidectomy. The control group included 24 patients (with no history of autoimmune thyroiditis and who were negative for autoantibodies) who underwent neck surgery for other reasons (primary hyperparathyroidism or a suspected thyroid nodule).
Thyroid function tests were performed at the time of tissue sampling (Table 1). TRAb were measured using a competitive immunoassay (BRAHMS Diagnostica GMBH, Berlin, Germany). Thyroid peroxidase (TPO) antibodies (TPOAb) and thyroglobulin (Tg) antibodies (TgAb) were measured using a sequential immunoluminometric assay (Immulite 2500; Siemens Medical Solutions Diagnostics, LA, CA).
Results are expressed as means and standard deviation.
TSH, thyrotropin; fT4, free thyroxin; fT3, free triiodothyronine; TRAB, thyrotropin receptor antibody; TPOAb, thyroid peroxidase antibody; TgAb, thyroglobulin antibody; ns, not significant.
Ultrasound-guided core needle biopsies of thyroid tissue were obtained using a Magnum® reusable biopsy device and a 16-gauge needle (Bard Medical, Bard Peripheral Vascular, Inc., Tempe, AZ). All core needle biopsies were performed by a single experienced surgeon (T.P.). All patients with newly diagnosed disease were treated with antithyroid drugs after the biopsy, and were followed up until remission.
Biopsy specimens were fixed in 10% neutral-buffered formalin and paraffin-embedded within 24 hours. Sections of formalin-fixed, paraffin-embedded (FFPE) tissue samples were cut into 3-μm-thick sections and mounted on glass slides.
Histological examination was performed on tissue sections stained with hematoxylin and eosin (H&E) to estimate the area of tissue inflammation and fibrosis. The mean diameter of the follicles in each section was measured by superimposing an ocular grid. The inflammatory reaction was examined by immunostaining of FFPE tissue sections using monoclonal antibodies specific for the following antigens: CD4 (helper T cells; Clone 4B12; NeoMarkers, Fremont, CA; dilution 1:100) and CD8 (cytotoxic T cells; Clone C8/144B; Dako, Carpinteria, CA; dilution 1:20) (both examined by sequential staining), and CD138 (plasma cells; Clone B-A38; AbD Serotec, Raleigh, NC; dilution 1:100) (examined by monostaining).
PDCs were identified by their high expression of CD123 (IL-3R α-chain; Clone 9F5; BD Pharmingen, Franklin Lakes, NJ; dilution 1:200). To ensure that the CD123+ cells were PDCs, they were costained with CD45RA (19,20). MxA+ cells were detected with an anti-MxA antibody (IgG2a; clone M143; dilution 1:100; kindly provided by Dr. O. Haller, Freiburg, Germany) (21). MxA is expressed on leucocytes, endothelial cells, and epithelial cells. To perform semiquantitative comparisons of the two latter cell types, both the extent and intensity of MxA staining was evaluated in thyroid epithelial cells and endothelial cells using an arbitrary scale (follicular epithelial cells: negative to 4; vessels: negative to 3).
All stained cells within a single tissue unit (defined by superimposing an ocular grid representing an area of 0.058 mm2) were counted at a magnification of ×400. The mean tissue area examined was 0.5 mm2. The examiners were blinded for all clinical data and the diagnoses pertaining to the patients and controls.
This clinical study was approved by the governmental Regional Ethics Committee for Medical and Health Research, South-East region, Norway. This study was conducted in accordance with the guidelines set out in The Declaration of Helsinki. Written informed consent was obtained from all participants prior to inclusion.
Statistical analysis
Data are expressed as the mean±standard deviation (SD), median and range, or number and percentage. Mean values were tested for statistical significance using the Student's t-test. The Mann–Whitney U-test was used for nonparametric data. One-way analysis of variance (ANOVA) was used to compare different groups. Correlations between variables were determined by the Spearman's correlation coefficient. A significance level of 5% (p<0.05) was applied when comparing patients and controls. All statistical analyses were performed using SPSS software v19 (SPSS Inc., Chicago, IL) and GraphPad Prism 4 (San Diego, CA).
Results
Forty-six patients with GD were included in the study: 22 (48%) with newly diagnosed, untreated GD, and 24 (52%) with chronic GD. The 24 control subjects had normal thyroid function and autoantibody titers (TRAb, TPOAb and TgAb) below reference ranges (Table 1).
The mean age of the patient group was 44 years (SD=13.5) and that of the controls was 52 years (SD=14). There were no differences in sex or ethnicity between the two groups. The male:female ratio in the patient group with GD was 1:8 and that in the control group was 1:9, and 94% of patients and 96% of controls were Caucasian.
The mean duration of disease was 33 months (SD=8.4) in the group with chronic GD and <3 months in the group with newly diagnosed GD. There were no significant differences in TRAb or TPOAb titers between these groups. Twenty-nine out of 44 (65%) patients were positive for TPOAb, and 15/44 (33%) were positive for TgAb (Table 1). Twenty-three out of 24 (95%) patients with chronic GD were treated with an antithyroid drug (carbimazole), and 10/24 (42%) were treated with corticosteroids, 9 (38%) of them for severe endocrine ophthalmopathy. Six patients were treated with intravenous methylprednisolone followed by low-dose oral prednisolone. The cumulative dose of steroids was 5.75 g at the time of inclusion. Three patients were treated by oral prednisolone. As the oral treatment is not standardized, the cumulative dose is not easy to calculate. At the time of inclusion, 8/9 used a low dose of prednisolone (mean 5.7 mg/day). One patient used steroids for treatment of Addison's disease.
Histological examination of H&E-stained tissue sections showed that the areas of inflammation and fibrosis were significantly greater in both patient groups than in the controls (Fig. 1). Thyroid follicles were more abundant and smaller in patients compared with those in the controls, even though this difference did not reach statistical significance (p=0.27). Organized lymphoid follicles were observed in the thyroid tissue of two patients with chronic GD.
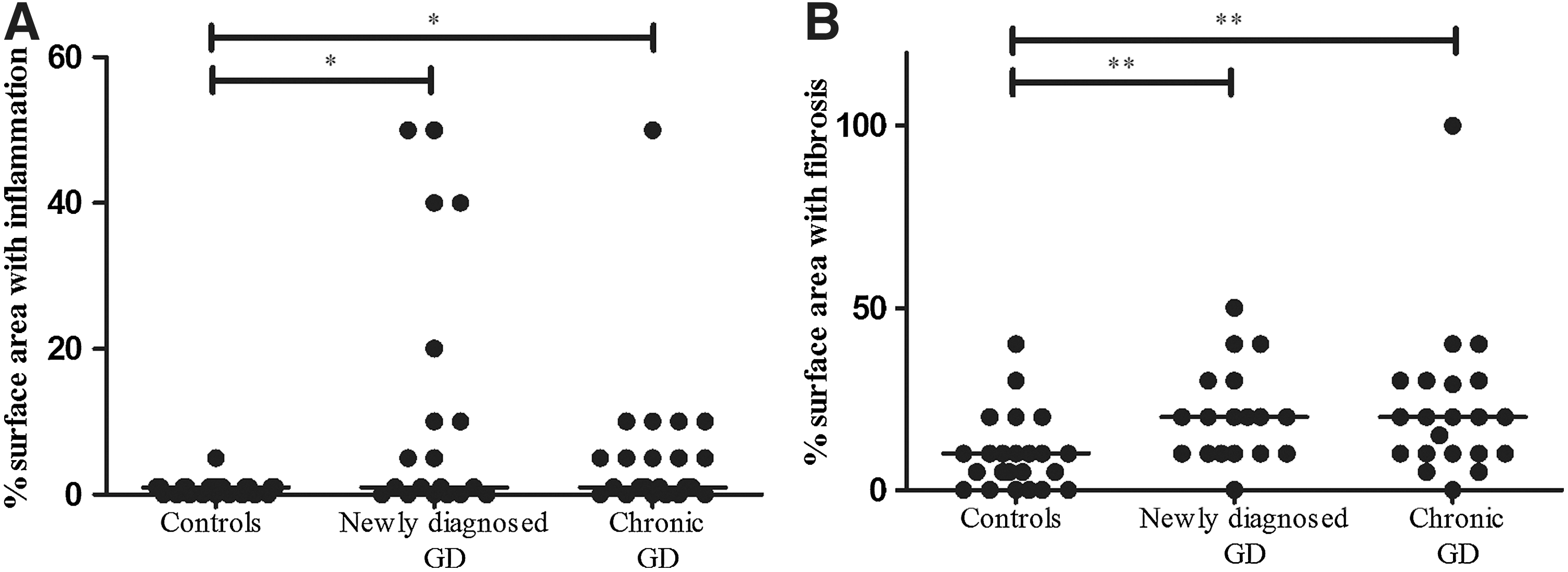
Areas of affected tissue in control subjects and patients with either newly diagnosed or chronic Graves' disease (GD).
Immunohistochemical staining of thyroid tissue showed that the number of CD4+ T cells was significantly higher in both patient groups than that in controls (Figs. 2A and 3D, G), being highest in the early stage of GD. By contrast, CD8+ T cells were only present at the chronic stage (Figs. 2B and 3D, G). The number of infiltrating plasma cells (CD138+ cells) was significantly higher in both patient groups than in the control group (p<0.0001). Again, the highest numbers were observed at the early stage of GD (Figs. 2C and 3E, H). There was no correlation between the number of CD138+ plasma cells and the level of anti-TRAb (R 2=0.0, p=0.9) or anti-TPOAb (R 2=0.27, p=0.309). However, there was a weak positive correlation between the number of CD138 cells and anti-Tg-Ab levels (R 2=0.141, p=0.014).

Number of cells per mm2 in FFPE sections of thyroid tissue from patients at different stages of GD and in tissue from control subjects.
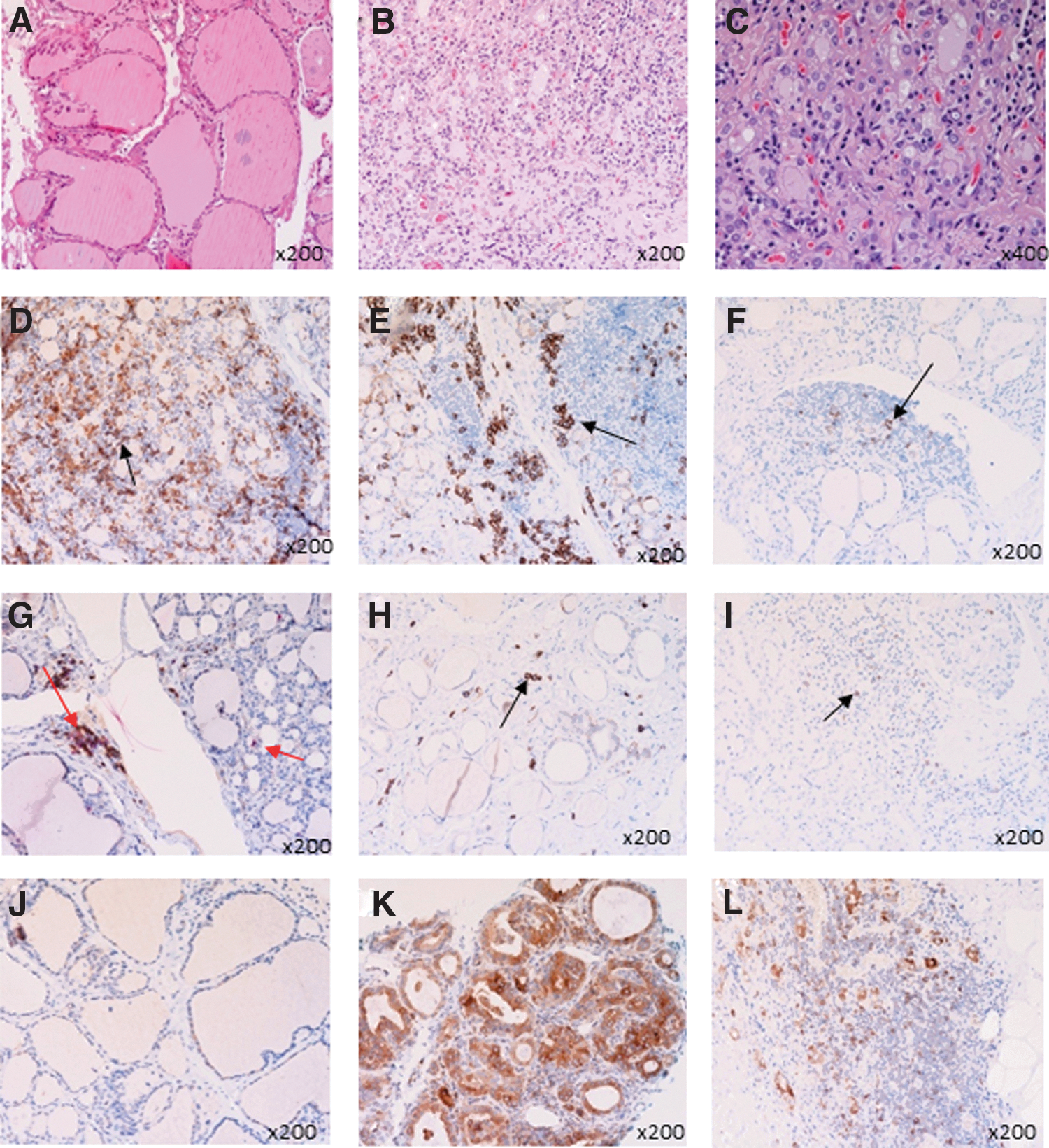
Histological and immunohistochemical staining of thyroid tissue sections. Representative examples are shown.
CD123+ PDCs were present in the thyroid tissue of a few individuals in both patient groups but not in that of the controls (Figs. 2D and 3F, I). MxA expression was higher in thyroid epithelial cells (Fig. 4A), endothelial cells (Fig. 4B) and immune cells (Fig. 4C) from patients with newly diagnosed GD than in those from control subjects (Fig. 3J–L). There was a positive correlation between the number of PDCs and the number of MxA-positive cells (R 2=0.71, p<0.0001), suggesting that PDCs may be a potential source of IFNα. No correlation was found between the number of MxA-positive cells or PDCs and the level of free thyroxin (fT4) or free triiodothyronine (fT3).

Expression of MxA in thyroid tissue from patients with GD.
The number of infiltrating cells was generally higher in the group of patients with GD who had positive TPOAb or positive TgAb. However, only the number of CD4+ T cells and CD138+ cells were significantly higher in the group with positive TgAb compared to negative TgAb (p<0.01 and p<0.001 respectively).
We recently examined tissue sections from these patients by immunohistochemistry (IHC) and reported the presence of viral capsid protein (VP1). In situ hybridization (ISH) also showed that EV RNA was more frequent in patient samples than control samples (12). However, we did not identify a correlation between the presence of virus and the number of infiltrating PDCs or the expression of MxA in the present study (Fig. 4D, E).
Available data for 20 of the patients with newly diagnosed GD showed that 18 (83%) achieved remission, within a mean treatment time of 16 months. Three of these (17%) had a relapse within a mean time of four months; the three patients received antithyroid drugs for 18, 24, and 29 months respectively. The remaining 2 of the 18 (10%) patients failed to achieve remission after three years of treatment. There were no significant differences in the number of immune cells between patients who achieved remission and those that did not.
Because steroids have immunomodulatory effects, we divided the patients with chronic disease into two groups: those treated with steroids, and those that were not treated. There was no statistically significant difference in the number of immune cells infiltrating the thyroid tissues between these two groups (data not shown). However, this does not rule out potential drug-induced anti-inflammatory effects, as we can assume that the group who received steroids had more aggressive disease accompanied by more severe endocrine ophthalmopathy.
Discussion
This study examined immunological and histopathological changes in thyroid tissue from patients with both untreated early stage and chronic GD, focusing on markers that indicate an immune response to viral infection. The expression of MxA was higher in the thyroid tissue of patients with recent onset untreated GD than in the controls, suggesting a possible role for IFN-α in the pathogenesis of GD. To our knowledge, this is the first biopsy study to include a significant number of patients with newly diagnosed untreated GD.
The histopathological examination revealed that lymphoplasmacytic inflammation and fibrosis were already present at the early stage of the disease, and both had increased in the chronic stage. Thyroid follicles were smaller (Fig. 3C). The inflammatory cells were dispersed throughout the thyroid tissue (Fig. 3), although organized lymphoid formations were observed in only two patients. These findings are in contrast to our previous findings in samples from patients with Hashimoto's thyroiditis, which showed a greater number of inflammatory cells (often with organized lymphoid follicles) and large areas with fibrosis (18). Thus, it appears that the damage to the thyroid tissue is less severe in GD than in Hashimoto's thyroiditis.
To date, the natural course of GD (and the associated immunological changes in the thyroid tissue) in such patients has not been described in detail because effective medical treatment is usually started immediately after diagnosis (3). Several studies report changes in peripheral blood lymphocyte subsets in patients with GD. However, the results are inconsistent. For example, Iwatani et al. reported that the proportions of CD4+ or CD8+ T cells in the peripheral blood of patients with GD were no different from those in controls (22), while others report an increase in the number of CD4+ T cells and a decrease in the number of CD8+ T cells (23), or an increase in the CD4:CD8 ratio (24). However, it is not clear to what extent changes in T cell numbers in the peripheral blood reflect the immunopathology observed in thyroid tissue. In the present study, we found increased numbers of CD4+ T cells in the thyroid tissue in the early stage of GD, indicating that this T-cell subset may play a role in initiating local disease.
Plasma cells were present in the thyroid tissue of patients in both groups but not in the controls. A subgroup of patients with newly diagnosed GD showed a very high number of plasma cells, but no correlation was found between the number of plasma cells and TRAb, TPOAb, or TgAb levels in the serum of patients with early stage or chronic disease. Thus, it is likely that the thyroid gland is not the only source of thyroid autoantibodies.
Surprisingly, distribution of CD4+, CD8+, and CD138+ cells were similar to findings in thyroid tissue from patients with Hashimoto's thyroiditis that we recently reported (18). Similarities between these two forms of AITD is even more obvious based on the fact that the number of CD4+ cells and CD138+ cells were significantly higher in the positive TgAb group.
Compared with those in the controls, both the number of PDCs and the expression of MxA (a surrogate marker for IFN-α production) were increased at the early stage of GD. Because PDCs can produce large amounts of type I IFNs in response to viral infection, our findings suggest that PDCs are directly involved in the pathogenesis of GD and may reflect the presence of viruses in these patients. Type I IFNs are a family of cytokines that have profound effects on cellular functions, such as proliferation, immune activation, and intracellular viral replication (25). The therapeutic use of IFN-α to treat a variety of disorders (e.g., hepatitis C) increases the risk of AITD (26 –30). IFN-α has clear antiviral effects and plays an important role in innate immune responses to viral infection. However, the ensuing inflammatory reaction may also cause tissue damage and lead to disease progression. Surprisingly, there was no correlation between virus-positive samples and the presence of MxA+ cells. One possible explanation for this may be that EV proteases can cleave molecules involved in the innate immune response and downregulate interferon-inducible genes in infected cells (31,32). This is one mechanism by which the virus can evade immune surveillance, resulting in viral persistence. The PDC numbers observed in the present study are consistent with those reported by Ruiz-Riol et al., who showed increased expression of IFN1 genes in the thyroid tissues of patients with GD (33). However, there is still no real evidence that this occurs in response to viral infection. High expression of MxA also occurs in patients suffering from other autoimmune diseases such as lupus erythematosus and psoriasis (34,35). Moreover, MxA has been widely studied in serum from patients with multiple sclerosis, mainly as a measure for bioactivity of IFN treatment (36,37).
We found that CD8+ T cells were mainly present at the chronic stage of GD, which is consistent with the findings of a previous study by Skowronek et al. (38). IHC revealed a high percentage of CD8+ T cells compared with CD4+ T cells in the thyroid tissue of euthyroid children with GD. We did not observe CD8+ T cells at the early stage of GD, suggesting that these cells primarily play a role in disease progression and chronicity. The biological significance of CD8+ T cells in the response to persistent viral infection is unclear (10,39,40). Primary infection with a virus can stimulate a vigorous cytotoxic T-cell response. The role of the antigen-specific component versus the bystander component of a primary T-cell response remains controversial (39,41). We found no correlation between the presence of EVs and the number of CD8+ T cells.
A different approach was adopted by Volpe et al. (42), who showed that there were fewer lymphocytes in the thyroid tissue of patients treated with antithyroid drugs. Whether this is a result of treatment or the natural course of the disease is unclear; the mechanism(s) underlying the immunosuppressive effects of antithyroid drugs remains controversial (26,27). It is almost impossible to study samples from patients with chronic GD that were not exposed to antithyroid drugs.
Because steroids have a potent anti-inflammatory effect, we compared patients who had been treated with those who had not. However, there were no significant differences in the number of immune cells infiltrating the thyroid tissue. Hence, we cannot exclude an effect of steroids, as the phenotype of GD varies to a large degree and the cell distribution may not reflect the severity of the disease in the group treated with steroids. The distribution of infiltrating cells in the newly diagnosed group could not predict remission. A previous clinical study failed to identify markers that predicted remission (43).
Thus, the most important finding of the present study was the upregulation of MxA expression in the early stage of the disease, which may reflect an antiviral response. Considering its potent pro-inflammatory effects, IFN-α is likely to contribute to the inflammatory changes observed in the thyroid tissue samples. However, although viruses may be the initial trigger that causes the breakdown of tolerance to self-antigens, they may have already been cleared from the tissues at the time of sampling.
In conclusion, we suggest that CD4+ T cells are involved at the early stage of GD, whereas CD8+ T cells play a role in the chronic phase. An inflammatory cell distribution similar to the one found in HT (however, higher in number in HT) demonstrates that GD and HT share even more common features. The presence of PDCs and the enhanced expression of MxA at the early stage of the disease suggest that PDCs may produce type I IFNs at the lesion, thereby contributing to immunological changes. Thus, the immune response associated with GD may be triggered by viral infection, although further studies will be needed to confirm this.
Footnotes
Acknowledgments
K.D.-J. was the primary investigator involved in this study. The authors would like to thank the staff at the Hormone Laboratory Research Section at Oslo University Hospital, Aker, and the Department of Pathology at Oslo University Hospital-Rikshospitalet, particularly biomedical laboratory scientists Douglas Pauly, Jan Schwarze, and Hogne Røed Nielsen, for their help with the immunohistochemistry. We also thank all the study participants.
Author Disclosure Statement
H.H. is a minor shareholder (<5%) in Vactech Ltd., which develops picornavirus vaccines. None of the other authors have any potential conflicts of interest to declare.