
Abstract
Background:
The aim of this study was to compare the detection of BRAFV600E by immunohistochemistry (IHC) using a mutation-specific antibody with molecular biology methods for evaluation of papillary thyroid carcinoma (PTC) patients.
Patients and methods:
This study concerned 198 consecutive conventional PTC patients, of which the majority were women (133/198; 67%), with a mean age of 56 years (range 19–79 years). BRAF mutation analysis was performed using DNA-based (direct sequencing, pyrosequencing, and SNaPshot) and IHC (VE1 antibody) methods. The sensitivity and specificity of IHC for BRAFV600E was compared with the molecular biology data.
Results:
A BRAF mutational result was obtained in 194 cases. A BRAFV600E mutation was detected in 153/194 (79%) cases of PTC when using at least one molecular method, and in 151/194 (78%) cases with IHC. No false positive results were noted using IHC to detect the BRAFV600E mutation. Besides this mutation, other rare BRAF mutations (BRAFV600K and BRAFK601E ), used as negative controls, were consistently negative with IHC. The sensitivity and specificity of IHC for the detection of this mutation were 98.7% and 100% respectively. The IHC test demonstrated excellent performance at a level equivalent to two DNA-based counterparts (pyrosequencing and SNaPshot). Failure to achieve a result was more frequent with the direct sequencing method than with the three other methods.
Conclusion:
IHC using the VE1 antibody is a specific and sensitive method for the detection of the BRAFV600E mutation in PTC. IHC may be an alternative to molecular biology approaches for the routine detection of this mutation in PTC patients.
Introduction
A
DNA-based assays are the standard methods for the detection of BRAF mutations in thyroid carcinomas (13). In routine clinical settings, these assays mostly include direct sequencing, pyrosequencing, SNaPshot, or Taqman technologies, although other more sensitive approaches are under investigation (13). More recently, immunohistochemistry (IHC) using a BRAFV600E specific antibody has been used for mutation detection in several types of neoplasias, including thyroid carcinomas (16 –23). However, assessment of the specificity and the sensitivity of this antibody in comparison to well-established molecular biology methods in a large cohort of PTC patients has not been performed to date.
The purpose of this study was to evaluate the value of an IHC approach for the detection of the BRAFV600E mutation in a consecutive series of 198 conventional PTC patients, and to determine the sensitivity and the specificity of the results in comparison to those obtained with three molecular biology methods (direct sequencing, pyrosequencing, and SNaPshot).
Patients and Methods
Patients and tissue samples
A total of 198 patients with PTC were enrolled in the study. Patients were surgically treated in the Department of Otorhinolaryngology (Pasteur Hospital, Nice, France) between 2004 and 2012. Written informed consent was obtained from all patients. Specimens of primary thyroid tumors were fixed (time of fixation, range 6–24 hours) in 10% formaldehyde for histological analysis and IHC. Adjacent tumor specimens were flash-frozen in liquid nitrogen and then stored at −80°C in the Human Tissue Biobank (Pasteur Hospital). A tissue section of the frozen specimen was systematically made and stained with hematoxylin and eosin (H&E) for histological control and for assessment of the percentage of tumor cells before DNA extraction. This study exclusively concerned the conventional PTC histological subtype including 160 macrocarcinomas and 38 microcarcinomas. A tumor was classified as conventional PTC if it showed >1% papillary formations and was composed of cells having the characteristic nuclear features of papillary carcinoma (24). All cases <10 mm in diameter were regarded as microcarcinoma. The epidemiological, clinical, and pathological features of this population are summarized in Table 1.
BRAF mutation analyses
Genomic DNA from frozen tissue samples was extracted using the MagNA Pure Compact Nucleic Acid Isolation Kit Large Volume (Roche Group, Inc., Tucson, AR) according to the manufacturer's instructions. To make sure that the extractions were successful and contained DNA, polymerase chain reaction (PCR) control reactions were performed using primers designed to amplify the human GAPDH gene.
We analyzed mutations in exon 15 of the BRAF gene by direct sequencing, pyrosequencing, and SNaPshot, as previously described (Supplementary Data, available online at
Preparation of tissue microarrays
H&E-stained sections of primary tumors were reviewed by five pathologists (M.I.I., S.L., E.L.-M., V.H., and P.H.), and tumor areas were marked on the slides. Representative carcinoma areas were selected for building tissue microarrays (TMAs), and arrays were designed as previously described (28). Three cores were selected for macrocarcinomas and two cores for microcarcinomas. In addition, five primary BRAFV600E -mutated melanomas (six tissue cores from biopsies performed on these patients) served as positive controls and were used for regulating mark spacing between core centers; cores were spaced at intervals of 1 mm in the x- and y-axes. Tissue cores of five primary BRAFV600K -mutated melanomas, five primary non-BRAF-mutated melanomas, and one BRAFK601E -mutated follicular variant of PTC served as negative controls. A 4 μm H&E-stained section was reviewed to confirm the presence of each tumor sample. A histospot was considered unsuitable for analysis if it was completely absent, contained no tumor tissue (sampling error), or contained too few tumor cells (<10%) for analysis (uninformative). For each patient, the mean score of a minimum two core biopsies was calculated.
Assessment of BRAFV600E mutation by IHC
The generation and validation of the BRAFV600E mutation-specific antibody (clone VE1) have been reported previously (20). IHC with the VE1 antibody was performed as described earlier (22,29). Briefly, 4 μm TMA sections were freshly cut and dried at 80°C for 15 minutes. VE1 IHC (1:10 diluted VE1 hybridoma supernatant) was performed on an automated immunostainer (Ventana BenchMark XT, Ventana Medical Systems, Tucson, AR) using standard reagents provided by Ventana and the OptiView DAB IHC Detection Kit (Ventana).
The intensity and cellular localization of the VE1 staining were independently analyzed by five pathologists (M.I., S.L., E.L., V.H., and P.H.) who were blinded to the molecular BRAF mutation data. Discrepancies were resolved using a multihead microscope. VE1 staining was scored based on signal intensity (0–3) and proportion (0–100%). Positively stained tumors were then stratified into three intensity categories: 1+, 2+, and 3+ (Supplementary Fig. S1). For statistics, histospots containing <10% of tumor cells were excluded from additional analyses. In parallel, in order to evaluate the topography and the intensity of the immunostaining of the positive-stained tumors observed on the TMAs, we selected 35 positive VE1 PTCs and performed IHC on whole paraffin sections using the same IHC protocol.
Statistical analysis
All cases were analyzed with the four different methods. To determine the specificity and sensitivity of each method, we compared the results of each method for each specimen, and when there was discordance, we used the consensus mutation to calculate each parameter as a reference test, as described (30). A consensus mutation was defined as that detected by at least one molecular method. The receiver operating characteristic (ROC) curve was used to estimate the cutoff value for VE1 immunostaining. A Kappa (κ) analysis was performed to evaluate the agreement between pyrosequencing, SNaPshot, and direct sequencing, and the consensus mutation, and to compare IHC data from whole-tissue sections and TMA histospots. Kaplan–Meier survival analysis and the log-rank test were used to evaluate the effect of BRAFV600E mutation on PTC recurrence. Recurrence was defined as the reappearance of disease after complete ablation of thyroid remnants as confirmed by cytological and/or histopathological examination or by the presence of definite 131I uptake outside of the thyroid bed on post-treatment whole body scan after administration of 5.55 GBq 131I (31).
Results
The DNA extracted from the 198 frozen samples was screened for a BRAFV600E mutation using pyrosequencing, SNaPshot, and direct sequencing methods. The diagnostic accuracy of each test in terms of sensitivity and specificity is presented in Table 2. One hundred ninety-four samples had a mutational result with at least one DNA-based analysis. A BRAFV600E mutation was found in 153/194 cases (79%) with pyrosequencing, in 147/194 cases (76%) with SNaPshot, and in 142/194 cases (73%) with direct sequencing (Fig. 1). No BRAF mutation other than V600E was found in PTC cases. By using these three methods, the genotype results were concordant in 183/194 cases (94%). Finally, a BRAFV600E mutation was detected in 79% (153/194) of PTC cases when using at least one DNA-based method.
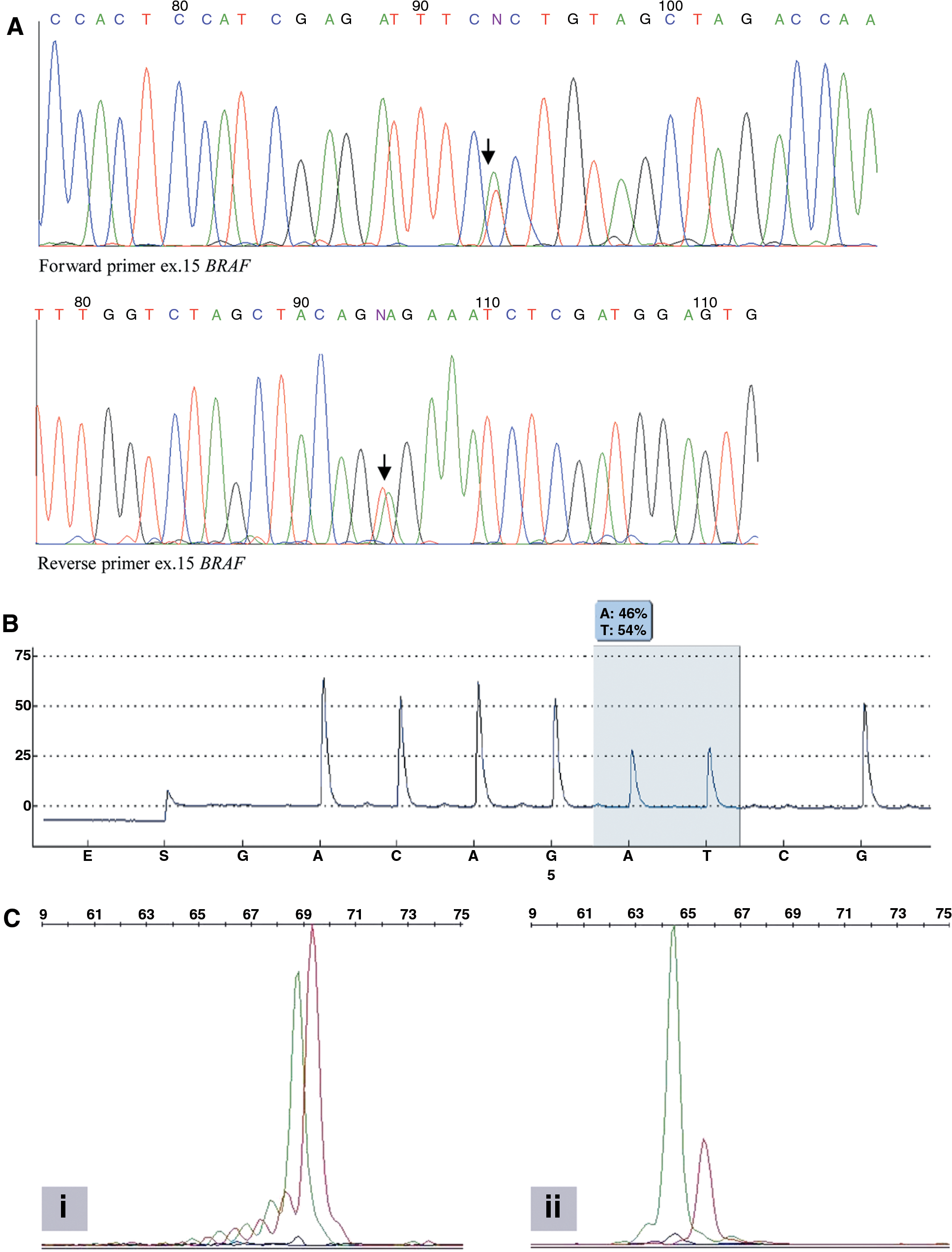
Representative BRAFV600E
analyses of a mutated papillary thyroid carcinoma (PTC) by direct sequencing
The detection of other rare BRAF mutations with the DNA-based techniques determines lower sensitivity for IHC among the 198 analyzed patients.
IHC, immunohistochemistry.
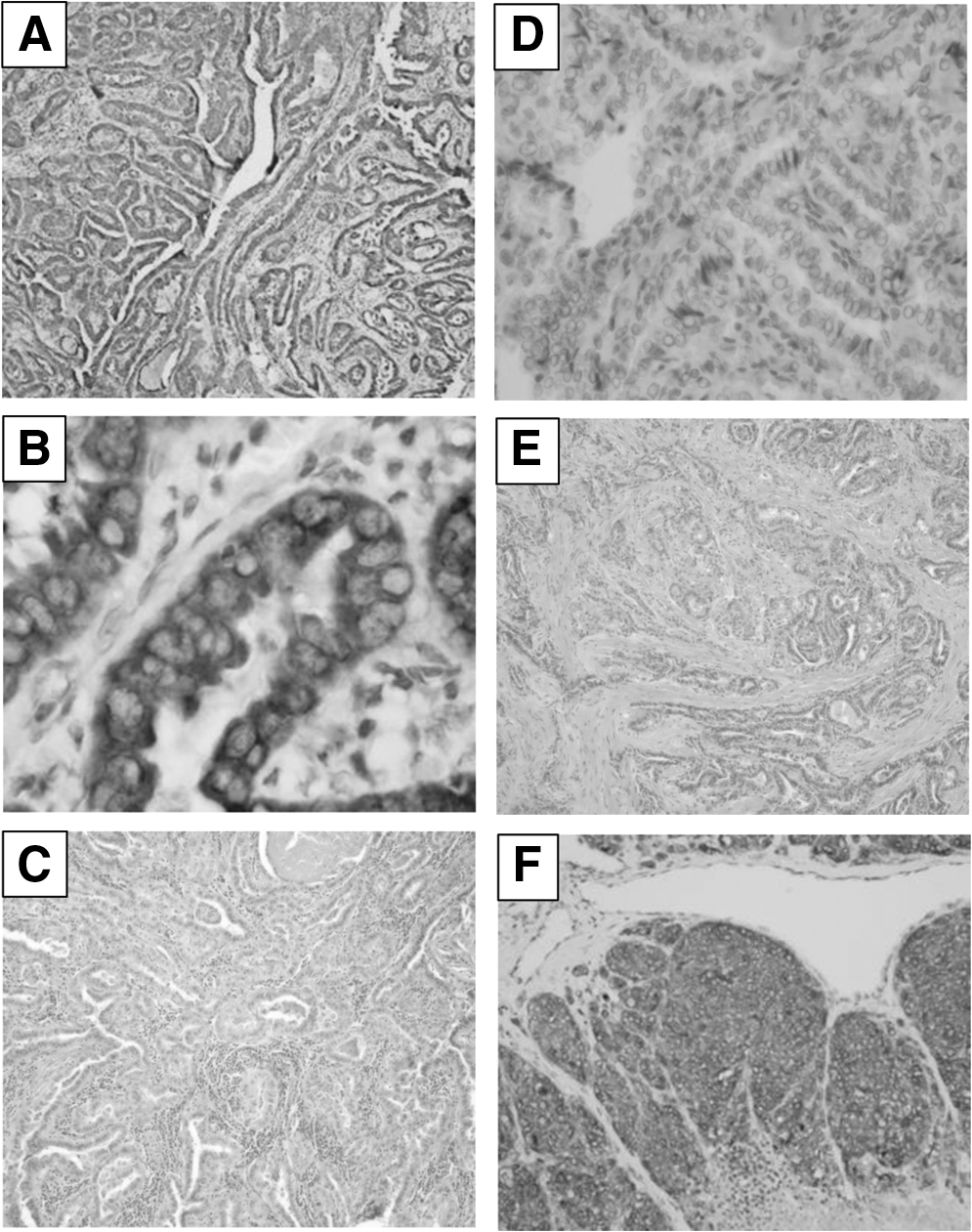
According to the ROC curve (AUC=0.993; Supplementary Fig. S2), a tumor was considered positive for the BRAFV600E mutation as determined by the VE1 immunostaining when a distinct, strong, and homogenous signal (score 3+) was observed in the cytoplasm of all carcinoma cells (Fig. 2). Positive immunolabeling for the BRAFV600E mutation detected by IHC on TMAs was noted in 78% (151/194) of all cases with molecular analysis (Fig. 2). The BRAFV600E expression levels observed on the TMA spots faithfully reflected the staining intensity of the protein on whole-tissue sections from corresponding tumor blocks (κ=0.92), with no variation between TMA cores (Supplementary Fig. S1). All five observers who interpreted the IHC both on TMA spots and whole-tissue sections showed perfect agreement (κ=0.99). No variation in VE1 immunostaining was observed between the leading/invasive edge versus the center of the tumor or with the allele peak height on DNA-based assays. No statistical difference in the frequency of V600E BRAF protein expression was seen between macrocarcinomas and microcarcinomas with positive molecular analysis (124/158 vs. 27/36 respectively; p=0.889, Fisher's exact test). We also observed six wild-type tumor samples that stained weakly or moderately (scores 1+ or 2+) on IHC (Supplementary Fig. S1), whereas none of the wild-type cases detected by a molecular method showed positive immunostaining (Fig. 2). None of the control tissue samples (including melanoma and follicular variant of PTC) having a BRAFV600K or a BRAFK601E mutation were positively immunostained (not shown), whereas melanoma samples harboring a BRAFV600E mutation, used as positive controls, were strongly immunostained (Fig. 2). The comparison of the four methods showed that failure to achieve a result was more frequent with direct sequencing than with the three other methods, including IHC.
Furthermore, we explored the relationship between the BRAF mutational status and the outcome of PTC patients. Patients were followed up for a median of 4.5 years (range 0.8–8.6 years) after thyroidectomy. Follow-up data were available for 178 patients, and all had a positive BRAF genotype. During this time, 12 (7%) patients showed locoregional recurrence. Among the 12 specimens (primary T2 stage, n=3; T3 stage, n=5; and T4 stage, n=4) with locoregional recurrence, 8 (67%) harbored the BRAFV600E mutation. However, the presence of the BRAFV600E mutation was not associated with tumor recurrence, as demonstrated by the univariate Kaplan–Meier curve analysis (Supplementary Fig. 3, p=0.165).
Discussion
This study, performed on a large series of 198 conventional PTC patients, shows that IHC using the VE1 clone was a specific and sensitive method to detect the BRAFV600E mutation. Several studies have previously evaluated the performance of the VE1 antibody in PTC cases (Table 3) (19,20,32 –35). However, an important limitation in the majority of these studies was the use of direct sequencing as the standard reference for BRAF genotyping. Such settings were bound to yield a relatively high number of false positive results with VE1 when compared to direct sequencing. Thus, in our study, we avoided a low quality gold standard method (i.e., direct sequencing) to assess the performance of the VE1 antibody by taking advantage of the comparison with highly sensitive DNA-based methods. The comparative analysis of the IHC approach with molecular biology methods for BRAFV600E detection demonstrated that IHC performed very well and at a level equivalent to the pyrosequencing and SNaPshot methods, but was more sensitive than the direct sequencing method. Moreover, the use of an IHC approach on TMA allowed us to perform an analysis of a large number of PTC cases. Although one recently published study employed the same approach using TMA, the immunostaining was first validated on whole sections with high agreement for immunostaining between TMA cores and the corresponding whole sections. One limitation related to the design of our study is the lack of PTC variants other than conventional type that have a lower prevalence of BRAF mutations such as follicular variant (3,33,35). This is likely to inflate estimates of the VE1 antibody sensitivity and specificity in low-prevalence subtypes. However, several studies have previously reported a strong relationship between VE1 immunostaining and the subtypes of PTC or other types of thyroid carcinoma (33,35).
FFPE, formalin-fixed paraffin embedded; NOS, not otherwise specified; PTC, papillary thyroid carcinoma.
Some solid tumors harboring other rarer BRAF mutations (i.e., the BRAFK601E and the BRAFV600K mutations) were consistently negative using the VE1 clone, as were the tumors without the BRAFV600E mutation (36 –38). With regard to the different clinical significance of these latter mutations, it is important to note that the VE1 antibody will not detect BRAF mutations other than V600E (39).
Interestingly, the positive (score 3+) immunostained tumors showed a diffuse and strong staining occurring throughout the tumor area. Moreover, we found no correlation between the expression of the BRAFV600E -mutated protein and the allele peak height on DNA-based assays, suggesting an “on-off” method of detection not suitable for quantitative purposes. Moreover, we also observed six cases that stained weakly or moderately (scores 1+ or 2+) on IHC, but these tumors had a wild-type BRAF genotype. As previously suggested, ambiguous, focal, or moderate immunostaining may cause uncertainty in the diagnostic setting (33,35). Therefore, the staining score should be validated in house. In such cases, additional genetic analysis may be required to clarify the BRAF status (24,35). Finally, no variation in staining intensity was observed between the leading/invasive edge versus the center of the tumor, as previously reported in PTC harboring a BRAFV600E mutation (32).
Although our results concerning the correlation between the BRAF status and patient outcomes were not consistent given the limited follow-up time, BRAF mutations were present in a higher proportion of recurrent tumors. Although several studies have reported that the presence of a BRAF mutation in PTC may be associated with poor clinicopathologic features, radioiodine resistance, and a higher risk for disease recurrence and shorter survival, the real impact of the BRAF mutation on the outcome of PTC patients still remains a controversial issue (9,12,40,41).
The advent of molecular therapeutics targeting some genomic alterations in solid tumors requires detection of gene mutations and rearrangements in tissues and cells. In this regard, the management of biological resources by the surgical pathology laboratories must be optimal both for the pre-analytical and analytical phases. IHC using the anti-BRAFV600E antibody can be potentially associated with false negative results in the case of a weak control of the pre-analytical steps with hypo- or hyperfixation of the biological specimen in formaldehyde.
In a few patients with thyroid cancer, the detection of the BRAFV600E mutation leads to the administration of specific inhibitor molecules targeting this mutation. In clinical daily practice, the detection of this mutation is performed by molecular biology technologies from extracted DNA obtained from thyroid FNA or from formalin-fixed paraffin-embedded tissue sections and more rarely from frozen specimens. In this context, the detection of a BRAF mutation is mostly performed in a molecular biology laboratory and not in the surgical pathology laboratory. However, surgical pathologists can take advantage of a growing list of available mutation-specific antibodies, including the VE1 BRAFV600E -specific antibody, to use IHC as an efficient screening tool for the detection of druggable genomic alterations, and thus to enhance the competitiveness relative to the molecular biology approaches (42).
The strengths and the advantages of detection of the BRAFV600E mutation using IHC can be commented on briefly. One of the main interests is to obtain simultaneously the BRAFV600E status and the morphological features corresponding to the mutated cells and to ensure that the presence or the absence of this mutation is strictly linked to the carcinoma cells. The fact that detection of the mutation can be done by the observation of a tissue section also reduces the possibility of sampling errors and thus increases traceability. False negative results can be obtained according to the sensitivity of the molecular biology method (such as with the direct sequencing method) and according to the percentage of mutated tumoral cells in the specimen submitted to DNA extraction. A false positive result obtained with the molecular biology methods is mainly due to contamination between different samples. Using IHC, this false positive result should be considerably limited and eliminated by using a negative immunostaining control simultaneously. Moreover, only an intense and diffuse cytoplasmic immunostaining in carcinoma cells (score=3), without nuclear staining should be considered to give a positive result. IHC gives a quicker result than other molecular biology technologies and thus reduces the turnaround time between the physician's request and the result. This would be of particular interest in urgent cases that require targeted therapy against an aggressive thyroid carcinoma harboring the BRAFV600E mutation (14). Moreover, one potential advantage of VE1 IHC over DNA-based assays is the possibility of testing decalcified specimens.
Still, the question remains about the clinical scenario in which BRAF testing by IHC would be of clinical benefit. The preoperative identification of BRAF positivity on FNA may guide initial surgical management (43). For instance, some authors have proposed BRAF testing of suspicious thyroid nodules ≥1 cm and lymph nodes, and a total thyroidectomy as the initial surgical approach for a BRAF-positive tumor (43,44). With regard to cytology analyses that do not providing a definitive diagnosis, such as those in the atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) category, this may avoid repeating FNAs and eliminate the need for two-step surgery, that is, diagnostic lobectomy followed by completion thyroidectomy (44). The role of BRAF testing in PTC that is already metastatic to the lymph nodes has not been clearly defined. Moreover, in current clinical practice, the performance of central neck dissection in patients with PTC varies. A recent study suggested that once selected, this procedure may be needed to a greater extent to reduce disease recurrence. According to the authors, this extent may be defined by the combined use of preoperative BRAF mutation testing with conventional risk factors of PTC (45).
Finally, cost should be taken into consideration, since an IHC method is more cost-effective than other molecular biology methods. For instance, in our institution, the total cost ratio between IHC and a molecular biology technique is in the order of 1:3.4. Taken together, these points highlight that the IHC approach can be a good alternative to the molecular biology approach for BRAFV600E detection in PTC patients. However, this approach has to be done in surgical pathology laboratories with dedicated expertise and quality-control procedures established for accredited laboratories.
Interestingly, this study demonstrates that the different BRAFV600E -mutated PTC samples were diffusively and strongly immunostained with the VE1 antibody in all the carcinoma cells. Both whole sections and TMA sections of the mutated tumors were strongly immunostained in their carcinoma cell components. Previous studies have discussed the fact that BRAFV600E could or could not be a clonal event in PTC (46,47). Even if the data obtained in the present study need to be confirmed in a larger series, the IHC results underline that the studied PTC homogenously expressed the BRAFV600E mutation. These findings confirm previous reports demonstrating the concordance in BRAFV600E mutation status between different metastatic sites within the same patient using genotyping (40). Therefore, BRAFV600E tumor homogeneity rather than heterogeneity may have important therapeutic implications (48).
The present work was performed in one laboratory and must be validated in other surgical pathology laboratories and in other large cohorts of PTC patients in order to demonstrate high reproducibility of the results. The interobserver analysis made by the pathologists in this study showed perfect concordance. This is in accordance with a recent multicenter study performed with the VE1 antibody but used on melanoma specimens, which showed a high concordance of the results of a blinded analysis by different surgical pathologists from different institutions (49).
In conclusion, we show that IHC is a valuable tool to detect the BRAFV600E -mutated protein in PTC patients. Whilst DNA-based assays are still the standard method for detection of the BRAFV600E mutation in thyroid carcinomas, they require specialized equipment. We believe that IHC is a promising screening modality showing excellent sensitivity and specificity for the detection of BRAFV600E -mutated PTC. In this context, IHC should be considered as a valid alternative to the molecular biology methods for the detection of this mutation, particularly as it is able to provide a quick result in daily clinical practice.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.