
Abstract
Background:
Enhanced reduction of multinodular goiter (MNG) can be achieved by stimulation with recombinant human thyrotropin (rhTSH) before radioiodine (131I) therapy. The objective was to compare the long-term efficacy and safety of two low doses of modified release rhTSH (MRrhTSH) in combination with 131I therapy.
Methods:
In this phase II, single-blinded, placebo-controlled study, 95 patients (57.2±9.6 years old, 85% women, 83% Caucasians) with MNG (median size 96.0 mL; range 31.9–242.2 mL) were randomized to receive placebo (n=32), 0.01 mg MRrhTSH (n=30), or 0.03 mg MRrhTSH (n=33) 24 hours before a calculated 131I activity. Thyroid volume (TV) and smallest cross-sectional area of trachea (SCAT) were measured (by computed tomography scan) at baseline, six months, and 36 months. Thyroid function and quality of life (QoL) was evaluated at three-month and yearly intervals respectively.
Results:
At six months, TV reduction was enhanced in the 0.03 mg MRrhTSH group (32.9% vs. 23.1% in the placebo group; p=0.03) but not in the 0.01 mg MRrhTSH group. At 36 months, the mean percent TV reduction from baseline was 44±12.7% (SD) in the placebo group, 41±21.0% in the 0.01 mg MRrhTSH group, and 53±18.6% in the 0.03 mg MRrhTSH group, with no statistically significant differences among the groups, p=0.105. In the 0.03 mg MRrhTSH group, the subset of patients with basal 131I uptake <20% had a 24% greater TV reduction at 36 months than the corresponding subset of patients in the placebo group (p=0.01). At 36 months, the largest relative increase in SCAT was observed in the 0.03 mg MRrhTSH group (13.4±23.2%), but this was not statistically different from the increases observed in the placebo or the 0.01 mg MRrhTSH group (p=0.15). Goiter-related symptoms were reduced and QoL improved, without any enhanced benefit from using MRrhTSH. At three years, the prevalence of permanent hypothyroidism was 13%, 33%, and 45% in the placebo, 0.01 mg, and 0.03 mg MRrhTSH groups respectively. The overall safety profile of the study was favorable.
Conclusions:
When used as adjuvant to 131I, enhanced MNG reduction could not be demonstrated with MRrhTSH doses ≤0.03 mg, indicating that the lower threshold for efficacy is around this level.
Introduction
R
Despite the more pronounced TV reduction achieved at six months in the 0.03 mg MRrhTSH group, we were, like previous studies (10 –12), unable to demonstrate that increased TV reduction translated into improved goiter-related symptoms or quality of life (QoL), as compared to radioiodine alone. However, tools to make these symptom assessments are not highly sensitive, and it is important that the long-term impact of rhTSH (or MRrhTSH) stimulated 131I therapy continue to be evaluated. RhTSH is used off-label in this context, and it appears that enhanced TV reduction is achieved at the expense of an up to fivefold increase in the rate of permanent hypothyroidism when a large 0.3 mg dose of rhTSH is used (10). The destruction of thyroid tissue by radioiodine may be regarded as an alternative to thyroid surgery.
In the present study, we present long-term (36 months) follow-up data from our previous report (14), which was the first randomized, placebo-controlled, dose-selection study using MRrhTSH and 131I for the shrinkage of MNG.
Patients and Methods
Patients and study design
In this phase II, randomized, single-blinded, placebo-controlled, three-arm, parallel group, dose-selection study, sponsored by Genzyme, a Sanofi Company (Cambridge, MA), 95 patients were treated with 131I to evaluate the dose, safety, and efficacy of MRrhTSH in combination with 131I to reduce the size of MNG. The follow-up period of 36 months was divided into two parts. Results from the first six months following 131I therapy, referred to as the Core Study (CS), have previously been published (14). The present report describes the outcomes of the additional 30-month follow-up period (Extension Phase [EP]).
A detailed description of inclusion and exclusion criteria has previously been reported (14). Key inclusion criteria were: a clinical diagnosis of MNG, 40–140 mL in size (by ultrasound (US) and palpation); age 35–80 years; serum free thyroxine (T4) index (fTI) and total triiodothyronine (T3) within the normal range, and serum TSH from undetectable to the upper limit of the normal range; and no suspicion of thyroid malignancy as determined by fine-needle aspiration biopsy. All patients had an indication for treatment based on either cosmetic and/or compressive complaints (85% of patients experienced symptoms of anterior neck compression). Key exclusion criteria were: previous partial or near total thyroidectomy and/or a history of 131I therapy.
One hundred forty-one patients were screened at 13 international study sites, and 95 patients were randomized to receive 131I therapy preceded by either placebo (n=32), 0.01 mg MRrhTSH (n=30), or 0.03 mg MRrhTSH (n=33). Investigators were unblinded toward the randomization scheme to facilitate study execution; only patients were blinded. All 95 patients completed the CS at six months. Four patients declined participation in the EP, and six patients later withdrew from the EP. Results are presented for the remaining 85 patients who completed the full study protocol. The protocol was reviewed and approved by each site's Institutional Review Board (IRB)/Independent Ethics Committee (IEC). Written informed consent was obtained from all patients. The study was designed, conducted, recorded, and reported in compliance with the principles of Good Clinical Practice (GCP) guidelines.
131I therapy and administration of MRrhTSH
Based on an (unstimulated) RAIU measurement and TV at baseline, the therapeutic 131I activity required to deliver a thyroid dose of 100 Gy in all of the three randomization groups was calculated using the following formula: Activity (MBq)=F×100 (Gy)×TV (mL)/residence time (hours). A single dose of 0.01 mg or 0.03 mg MRrhTSH or placebo was administered intramuscularly (IM) 24 hours before 131I therapy. Details regarding the RAIU measurements and the study compound (MRrhTSH) are reported in our previous publication (14).
TV estimation
TV was monitored by computed tomography (CT) scan of the neck and performed at baseline, six months, and 36 months following therapy. A CT scan was offered to patients who withdrew early from the EP. TV and the smallest cross-sectional area of the trachea (SCAT) were determined by an expert radiologist (blinded to treatment) using a standardized procedure at a central reading facility.
Outcome measures and follow-up
Efficacy
The primary outcome measures of the EP were the percent change in mean TV from baseline to 36 months in each of the three randomization arms and the differences in TV between the three groups. Secondary endpoints included the percent change in SCAT from baseline to 36 months and the differences in SCAT between the treatment groups. The thyroid disease-specific questionnaire ThyPRO (15) was used to evaluate the impact of the treatment on QoL. The change from baseline to 12, 24, and 36 months on the ThyPRO goiter-specific items was evaluated, and differences between treatment groups on the ThyPRO goiter-specific items were analyzed. Of the 17 goiter-specific questions (included in the ThyPRO), eight questions concerned physical symptoms. Further analysis of these eight physical goiter-specific questions was performed using a composite score methodology, in which a score was assigned for each response (0=“not at all”; 1=“a little”; 2=“some”; 3=“quite a bit”; 4=“very much”), totaled and converted for presentation on a scale from 0 to 100.
Safety
In the EP, thyroid function was monitored every three months until 36 months. Thyroid function tests (TFTs) included TSH, free T3 (fT3), free T4 (fT4), FTI, total T3 (TT3), and total T4 (TT4). Antibodies against the TSH receptor were measured at baseline and repeated at six months in subjects whose TFTs suggested hyperthyroidism. In addition, antibodies against MRrhTSH were measured at baseline and at 6 and 36 months. Patients were continuously monitored for adverse events (AEs), which were coded using the Medical Dictionary for Regulatory Activities (MedDRA) v10.0 or higher.
Statistical methods
The sample size was estimated assuming a mean TV reduction of 25% and 40% at six months in the placebo (131I only) group and the 0.01 mg MRrhTSH group respectively. Using a two-sided t-test, this study required 29 patients per arm to have an 80% power for the detection of the group difference at a 0.05 significance level. Allowing for a 15% dropout, approximately 33 patients per arm were enrolled for the evaluation of the primary endpoint at six months. Statistical analyses were performed using SAS v9.1 (SAS Institute, Cary, NC). All pairwise comparisons were carried out with two-sided statistics at a significance level of 0.05. Summary statistics are presented as mean±standard deviation or median (range) for continuous data and as percentages for categorical data. Differences between each MRrhTSH group and the 131I only (placebo) group, with respect to the percent change from baseline in TV and in SCAT, were evaluated using analysis of covariance (ANCOVA) models with the treatment-group factor and the baseline value as a covariate. Potential interactions between the treatment-group factor and the covariate (e.g., TV, SCAT, and 131I uptake at baseline) on the treatment effects of MRrhTSH were also evaluated. Pearson's product–moment correlation coefficients were computed to explore the linear correlation between TV and SCAT at baseline. Kaplan–Meier product-limited estimators were employed to estimate the percentage of clinical events of interest with censored data during the course of the study. The log-rank chi-square test was also employed to assess the distribution equality across the treatment groups. Fisher's exact test was employed to assess the potential association between the study treatment and the occurrence of thyroid events (hyperthyroidism and hypothyroidism) following the study treatment.
Results
Baseline characteristics
Baseline variables, including the therapeutic 131I activities administered in each group, have been reported previously (14). There were no significant differences in any of the baseline post-randomization variables among the three treatment groups.
Thyroid volume
At 6 and 36 months, TV was significantly reduced compared to baseline in all treatment groups (Table 1). At six months, the percent reduction in TV was greater in the 0.03 mg MRrhTSH group (32.9±20.7%) compared to both placebo (23.1±8.8%) and the 0.01 mg MRrhTSH group (23.3±16.5%). The difference in TV reduction between the 0.03 mg MRrhTSH group and the placebo group at six months was statistically significant (p=0.033; Fig. 1).
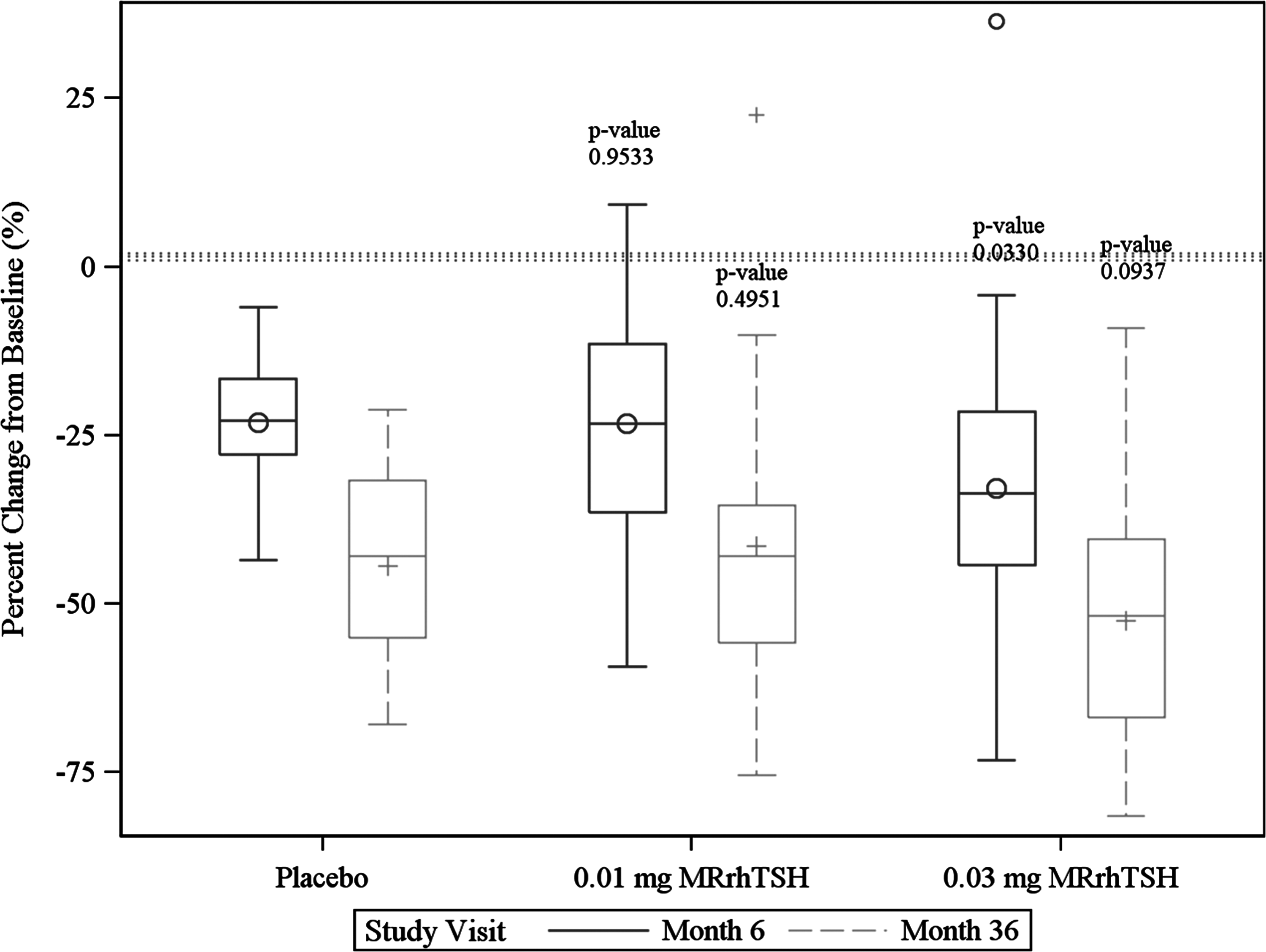
Percent change in thyroid volume from baseline at six months and 36 months by treatment group. The upper and lower fences of the boxplot indicate 1.5×IQR higher or lower than the upper and lower quartiles respectively. p-Values are derived from pairwise comparisons between each MRrhTSH group and the placebo group. IQR, interquartile range; MRrhTSH, modified-release recombinant human thyrotropin.
Mean thyroid volume (mL)±standard deviation is displayed.
p-Value, six months compared to baseline.
p-Value, 36 months compared to baseline.
MRrhTSH, modified-release recombinant human thyrotropin.
Among the 91 patients entering the EP, 82 patients completed the 36-month CT scan, and another four patients had an early termination CT scan (two patients at 21 and 28 months respectively in the placebo group; one patient at 31 months in the 0.01 mg MRrhTSH group, and one patient at 30 months in the 0.03 mg MRrhTSH group). Results at 36 months (n=82+4) refer to the last CT scan-related measurements made. The percentages of TV reduction achieved at six months in the nine subjects with CT scan dropout at 36 months is provided in Table 2. The mean percent TV reduction from baseline to 36 months was 44±12.7% in the placebo group, 41±21.0% in the 0.01 mg MRrhTSH group, and 53±18.6% in the 0.03 mg MRrhTSH group, with no overall statistically significant differences among the groups (F-value=2.11, p=0.105; Fig. 1).
CT scan dropout: no 36-month or early termination CT scan data; TV, thyroid volume.
The subset of patients with a basal 131I uptake <20% experienced greater TV shrinkage at 36 months in the 0.01 and 0.03 mg MRrhTSH groups, most evident in the 0.03 mg MRrhTSH group, where, at 36 months, patients with basal 131I uptake <20% achieved, on average, an estimated 24% greater TV reduction than the corresponding subset of patients in the placebo group (mean difference 23.9%; [CI 3.9%, 43.9%]; p=0.01).
SCAT
Mean SCAT did not differ among the three groups at baseline (14). In all groups combined (n=95), a negative correlation between baseline TV and baseline SCAT was observed (Pearson correlation ρ=−0.23, p=0.02; Fig. 2). At both 6 and 36 months, SCAT had increased significantly, compared to baseline, in all groups (data not shown). At 36 months, the largest relative increase in SCAT was observed in the 0.03 mg MRrhTSH group (13.4±23.2%), although not statistically different from the increases observed in the placebo group (9.2±22.1%) or the 0.01 mg MRrhTSH group (3.6±15.4%; F-value=1.96, p=0.15). At 36 months, the percent change in SCAT showed no correlation with the percent TV reduction (all patients combined, Pearson correlation ρ=−0.15, p=0.18).

Basal thyroid volume and smallest cross-sectional area of the trachea at baseline.
QoL
More than 50% of patients reported no baseline symptoms for 9 of the 17 goiter-specific questionnaire items. Considering only patients who did report symptoms at baseline, the majority reported an improvement in symptoms after treatment for almost all goiter-specific items and in all treatment groups. There were no apparent differences in symptom improvement in the 17 goiter-specific questions and overall QoL question among the treatment groups at 6 and 36 months.
At baseline, the mean composite scores of ThyPRO (consisting of the eight physical goiter-specific questions) were not substantially different across the three treatment groups (24.5±20.57, 29.0±19.30, and 21.4±15.55 in the placebo, 0.01 mg, and 0.03 mg MRrhTSH groups respectively; F-value=1.19, p=0.31; Fig. 3). There were no statistically significant differences in mean composite scores between treatment groups at six months (F-value=0.74, p=0.48) or 36 months (F-value=1.23, p=0.30).

Composite scores of eight physical goiter-specific questions in the ThyPRO questionnaire by treatment group at baseline, six months, and 36 months. The degree of physical goiter-related discomfort increases with increasing composite score. The upper and lower fences of the boxplot indicate 1.5×IQR higher or lower than the upper and lower quartiles respectively. ThyQoL, quality of life determined by thyroid-disease specific questionnaire.
Thyroid function
From 6 to 36 months, the prevalence of permanent hypothyroidism requiring levothyroxine replacement increased from 6%, 3%, and 24% to 13%, 33%, and 45% in the placebo, 0.01 mg, and 0.03 mg MRrhTSH groups respectively. Based on Kaplan–Meier estimation, the percentage of hypothyroid patients receiving levothyroxine was greater in the 0.01 mg and 0.03 mg MRrhTSH groups than the placebo group (p=0.001, log-rank chi-square test; Fig. 4). At six months, 11 patients (n=1 placebo, n=5 0.01 mg MRrhTSH, and n=5 0.03 mg MRrhTSH) had blood samples analyzed for TSH receptor antibodies, and all were negative. No patient was positive for TSH receptor antibodies during the EP. At six months, all patients had negative antibodies against MRrhTSH.
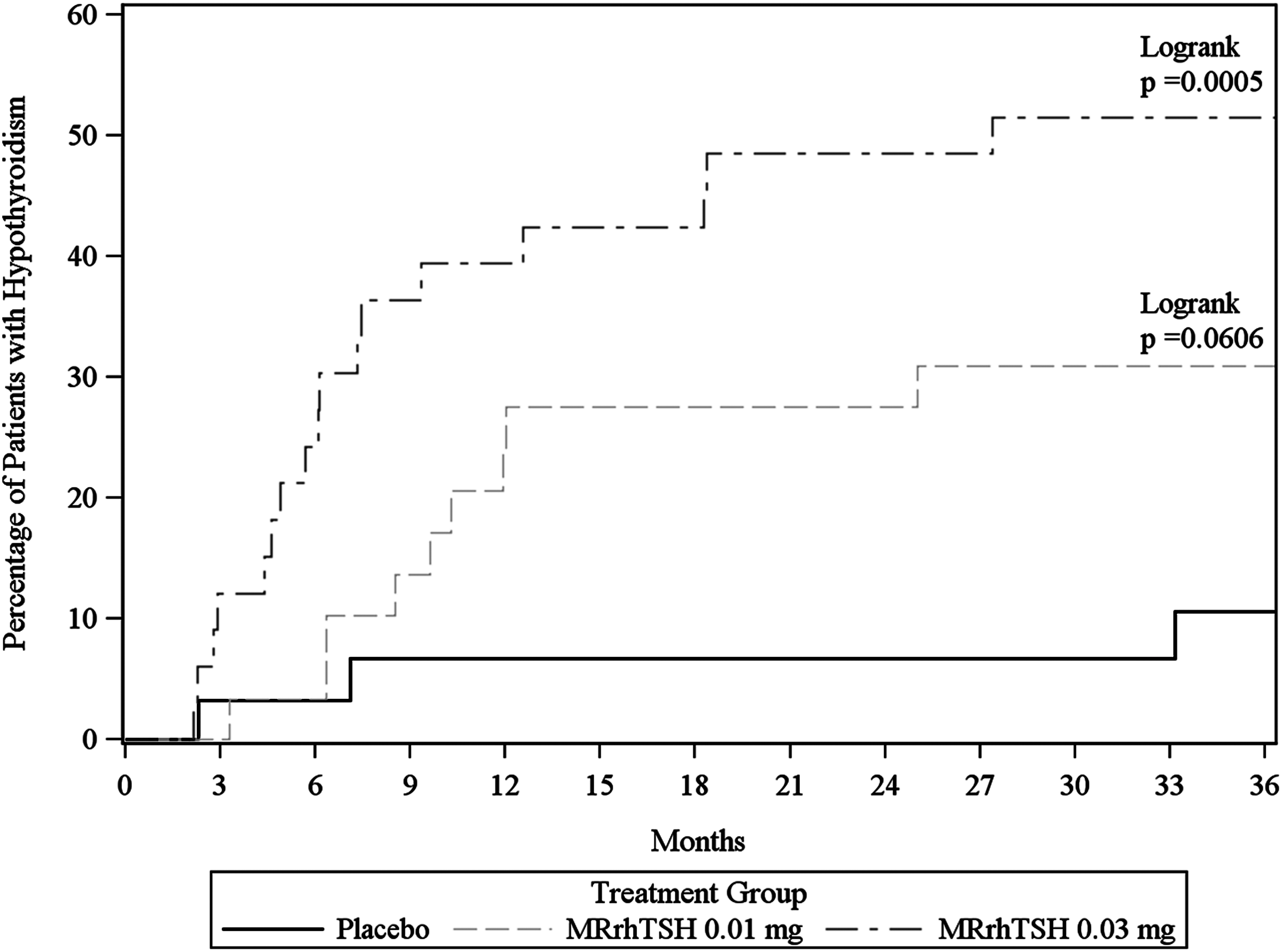
Kaplan–Meier curves for levothyroxine-treated hypothyroidism by treatment group. p-Values are derived from pairwise comparisons between each MRrhTSH group and the placebo group over the 36-month period.
Safety
The overall safety profile of the study compound was favorable. No MRrhTSH-treated patients withdrew from the study due to an AE. Throughout the 36-month study duration, a total of 410 treatment emergent AEs were reported from 84 (88%) patients. Based on the Medical Dictionary for Regulatory Activities (MedDRA), AEs by system organ classes (SOCs) were similar among the three treatment groups. The highest frequency of AEs (67 events in 45/95 (47%) patients) occurred in the SOC of Endocrine Disorders. More patients in both of the MRrhTSH groups reported AEs consistent with hyperthyroidism (nine events in 8/30 (27%) in the 0.01 mg MRrhTSH group, and 12 events in 11/33 (33%) in the 0.03 mg MRrhTSH group), compared to the placebo group (two events in 2/32 (6%); p=0.04 and 0.01 respectively). All treatment-emergent AEs of endocrine disorders and frequent AEs reported by ≥10% patients during the study in any treatment group are summarized by preferred term in Table 3.
Discussion
In this large, multicenter, randomized, placebo-controlled, dose-selection study evaluating two low doses of MRrhTSH or placebo in combination with 131I therapy to reduce the size of MNG, no statistically significant overall enhancement of TV reduction was achieved with MRrhTSH. At the three-year follow-up, mean TV decreased by 53% in the 0.03 mg MRrhTSH group, compared to 44% and 41% in the placebo and 0.01 mg MRrhTSH groups respectively. The observed difference was not statistically significant at the three-year follow-up (note that this extension study may have been underpowered at 36 months), but the overall result was in line with the pattern observed at six months. The subset of patients with a baseline RAIU <20% achieved a greater reduction in goiter size with MRrhTSH stimulation. Although we did not measure the MRrhTSH-stimulated RAIU, previous studies (6) have shown that the increase in thyroid RAIU induced by rhTSH is inversely correlated to the initial uptake. The therapeutic 131I activities administered in this study were calculated based on the basal RAIU. It follows that the subset of patients with a low RAIU must have received a much higher absorbed thyroid radiation dose. These observations suggest that subjects with a low (i.e., <20%) RAIU could be ideal candidates for rhTSH or MRrhTSH stimulated 131I therapy.
The present study used a new formulation of rhTSH that has been termed MRrhTSH. The new formulation is nonaqueous and is more viscous than marketed rhTSH, which contains necessary salts in the dry pellet and is routinely reconstituted for use in thyroid cancer patients using sterile water. After IM injection in humans, the pharmacokinetic profiles of rhTSH and MRrhTSH differ, and MRrhTSH causes a statistically significant slower rise in serum T3 levels than aqueous rhTSH (unpublished Phase 1 study [THYR-012-05] results, data on file, Genzyme).
The TV reductions in this current Phase 2 study were modest compared to studies using 131I alone (TV reduction 50–60% at three to five years) (16,17) and in a few long-term studies evaluating rhTSH. Fast et al. (18) demonstrated an absolute TV reduction of 56% and 70% at six years using placebo and a far greater dose of 0.3 mg rhTSH respectively. Cardia et al. (19) reported reductions of 57% and 73% at four years using placebo and an even higher dose of 0.45 mg rhTSH respectively. Giusti et al. (20) observed reductions of 44% and 60% at four years following placebo and two successive daily doses of 0.1 mg rhTSH respectively. However, these larger doses of rhTSH led to transient thyrotoxicosis in some patients.
In all groups, 131I therapy resulted in a marked decrease in goiter-related symptoms and improvement in QoL, irrespective of MRrhTSH use. The difficulty in demonstrating a superior outcome in the 0.03 mg MRrhTSH group may be because many patients enrolled in this study were relatively asymptomatic. Furthermore, QoL data are prone to rather large random variation, necessitating large sample sizes in order for small to moderate effect sizes to be identified. It is important to recognize that the failure to demonstrate improvement in QoL when stimulating with MRrhTSH does not necessarily disqualify its use in this context. Although enhanced TV reduction may not be required to relieve goiter-related symptoms in the majority of patients, there remains the long-term risk of goiter recurrence. It is reassuring that a recently published randomized controlled study was able to demonstrate that the amplification of TV reduction obtained at one year, when stimulating with a large dose of 0.3 mg rhTSH, was maintained at six years of follow-up (18). This resulted in a reduced need for additional therapy, and there was improvement in overall patient satisfaction (18).
In this large study of MNG patients, we demonstrate, for the first time, that SCAT was negatively correlated to initial TV. Owing to variation in the impact of goiter size, goiter location, and the rate of goiter growth on tracheal anatomy, such a relationship has been difficult to demonstrate in previous studies, even in patients with very large goiters (21,22). Although SCAT increased after therapy in all subgroups, we were not able to demonstrate that this was positively correlated to TV reduction. The absence of such a correlation was likely because subjects enrolled in this study had little impairment of SCAT at baseline. Previous studies have demonstrated that rhTSH-stimulated 131I therapy facilitates tracheal decompression, suggesting that subjects with large compressive goiters are candidates for such therapy if surgery is contraindicated (22).
Our study indicates that the lower threshold level for efficacy (enhanced TV reduction) is around 0.03 mg of MRrhTSH. This observation is in contrast to two small comparative studies evaluating rhTSH doses between 0.005 and 0.1 mg. In the observational, controlled study by Cubas et al., stimulation with placebo, 0.005 mg, and 0.1 mg rhTSH before a fixed dose of 131I activity resulted in 15%, 39%, and 37% TV reduction at the two-year follow-up respectively (23). The results in that study should be interpreted with caution, since there were only nine subjects in each arm, the 0.005 mg rhTSH group had a very low baseline RAIU (i.e., 14.2%), and some patients had received methimazole prior to enrolment. In the small randomized controlled study by Albino et al., stimulation with placebo, 0.01 mg, and 0.1 mg rhTSH before a fixed dose of 131I resulted in 19%, 37%, and 37% TV reduction at the one-year follow-up respectively (13).
Considering that TV reduction is positively correlated with the absorbed thyroid dose (Gy) (10,11,16,21,24), which is directly proportional to the RAIU, a straightforward explanation of the lack of efficacy in the group receiving 0.01 mg MRrhTSH could be that 0.01 mg had less impact on the RAIU than did 0.03 mg. The average baseline RAIU was similar in our three groups. Thus, this hypothetical difference in drug-induced RAIU would have resulted in a higher absorbed thyroid radiation dose in the 0.03 mg MRrhTSH group, although the RAIU post-MRrhTSH stimulation was not measured. Well-designed, randomized, comparative studies evaluating the dose–response curve (in terms of increasing RAIU) are lacking, although a few previous studies support the view that the effect declines below 0.03 mg. In the study by Albino et al., the increase in RAIU was much higher (absolute increase 25%) in the 0.1 mg rhTSH group compared to the 0.01 mg rhTSH group (absolute increase 7%) (13). Likewise, Nieuwlaat et al. observed that 0.03 mg rhTSH resulted in a more pronounced increase in RAIU (relative increase 145%) compared to 0.01 mg (relative increase 87%) (8). Overall, the current evidence points to a positive dose–response curve in the range between 0.01 and 0.03 mg, whereas it is relatively flat above 0.03 mg (25 –27). Although considered equipotent, the impact of MRrhTSH and rhTSH on thyroid RAIU has been compared head to head in only nine healthy subjects in an earlier study (THYR-012-05); at a dose of 0.1 mg IM, both drugs more than doubled the 24 hour 123I uptake compared to baseline, showing an increase of about 125% (data on file, Genzyme).
Although it is likely that the lack of efficacy in the 0.01 mg MRrhTSH group was the result of an insufficient increase in the RAIU, it is important to recognize that other factors may have contributed to the overall results of the present study. A large, randomized, placebo-controlled study has suggested that rhTSH preconditions the nodular goiter/thyrocyte beyond the increase in the RAIU, in which case the dose of rhTSH could be an independent determinant of TV reduction (28). This hypothesis remains to be evaluated in randomized controlled studies. Disqualifying all but one previous comparative study, the absorbed thyroid dose must be controlled if the aim is to evaluate any independent effect of the dose of rhTSH on TV reduction. So far, this design has only been evaluated in a small, observational, nonrandomized study, demonstrating, at one year, a slightly greater TV reduction following 0.03 mg (41%) compared to 0.01 mg (35%) of rhTSH in combination with 100 Gy (8).
MRrhTSH was designed to attenuate the major side effect of rhTSH stimulation, a rapid dose-dependent increase in circulating thyroid hormones (10,29,30). Although hyperthyroidism, in the early phase following 131I therapy, was more frequent in both MRrhTSH groups than in patients who had received placebo, the overall safety profile of the study was excellent. This result should be seen in the context that in the relevant dose range (0.01–0.1 mg), rhTSH does result in a small rise in circulating thyroid hormones and is generally not associated with major side effects (13,25,28,31). Furthermore, 131I therapy itself results in an excess thyroid hormone release caused by radiation damage to the thyroid follicular cells (4,32). By 36 months, permanent hypothyroidism occurred more frequently in the 0.03 mg MRrhTSH group, presumably reflecting more pronounced thyroid tissue destruction.
In conclusion, the negative result of our study demonstrates a lower threshold for efficacy, since at least MRrhTSH doses <0.03 mg have no effect on goiter reduction when combined with 131I therapy. Finally, the dose of MRrhTSH required to enhance the thyroid RAIU sufficiently before 131I therapy is likely to depend on thyroid function, the basal RAIU, and iodine intake, among other factors (33).
Footnotes
Acknowledgment
This study was a Genzyme-sponsored trial.
Author Disclosure Statement
S.F., A. Pinchera, M.V., J.L.W., D.A.H., W.H., I.R., H.N.S., M.G.C., L.A., L.E.B., R.C., C.D., E.P.L., C.M., and H.G. have nothing to disclose. L.H. is a consultant and advisory board member and has provided expert witness for Genzyme. F.P. is an advisory board member and a recipient of fees for talks from Genzyme. A.M.L. has received research funding from Genzyme and is supported in part by NIH 5K23HD068552. C.R. and A.D. are recipients of fees from Genzyme for talks. T.W. has received unrestricted research grants from Genzyme. J.M. and A. Purvis are employees and shareholders of Genzyme.