
Abstract
Background:
Indoleamine 2,3-dioxygenase (IDO) is overexpressed in many different types of tumor and is associated with activation of FOXP3+ regulatory T cells (Treg cells) and downregulation of cytotoxic cellular immunity in the tumor microenvironment. It has been suggested that IDO inhibitors can be utilized as an effective therapeutic agent against human cancers. However, the expression of IDO and its association with tumor-infiltrating lymphocytes (TILs) remain unclear in papillary thyroid microcarcinoma (PTMC).
Methods:
Immunohistochemical staining for IDO expression was performed on 124 PTMC samples. TIL subsets (CD3+, CD8+, and FOXP3+ T cells) were counted in serial sections. The relationships between the expression of IDO and infiltration of TIL subsets, as well as the relationships between these immunomodulating factors and clinicopathologic parameters of PTMCs, were analyzed.
Results:
There was a significant correlation between IDO expression and reduced CD3+ TIL and increased FOXP3+ TIL. IDO expression was found in 31% of PTMC and was associated with aggressive clinicopathologic features of the tumor such as extrathyroidal extension (ETE) and multifocality. High infiltration of FOXP3+ Treg cells in the tumor was associated with lymph node metastasis, ETE, and multifocality. Furthermore, high FOXP3/CD8+ ratio was associated with multifocality and lymph node metastasis, and high FOXP3+/CD3+ ratio was related to ETE and multifocality. In multivariate analyses, IDO expression was found to be an independent predictive factor for ETE and tumor multifocality.
Conclusions:
IDO expression and infiltration of FOXP3+ Treg cells were closely related to each other and were associated with aggressive features of PTMC, suggesting that disruption of antitumor immunity by IDO expression, and thus, infiltration of FOXP3+ Treg cells may contribute to tumor progression in PTMC.
Introduction
P
The immune system eliminates tumor cells and controls tumor growth by means of immunosurveillance (6), and the presence of lymphocytic infiltration has been reported to be associated with more favorable outcomes in PTC (7,8). Of the tumor-infiltrating lymphocytes (TILs), CD8+ cytotoxic T lymphocyte (CTL) is a crucial component of tumor-specific cellular adaptive immunity, and studies have demonstrated that CD8+TIL is associated with favorable outcomes in various cancers, including colorectal (9,10), ovarian (11), and breast cancers (12). Naïve CD4+ T cells play a major role in the immune response; they differentiate into four major lineages (Th1, Th2, Th17, and Treg cells) depending on the stimulation by cytokines and transcription factors (13). Regulatory T cells (Treg cells), which are identified as CD4+ CD25+ FOXP3+ T lymphocytes, are known to disturb antitumor immunity by suppressing the effector functions of various immune cells, and have been implicated in evading immunosurveillance against cancer cells (14). Thus, FOXP3+ Treg cells have been shown to be associated with adverse outcomes in various human cancers (15 –17). However, studies on the role of specific lymphocyte subsets have been rare in PTC. Only two recent studies have shown a correlation between FOXP3+ Treg cells and aggressive features of PTC (18,19).
Indoleamine 2,3-dioxygenase (IDO) is a heme-containing monomeric oxidoreductase that catalyzes the degradation of tryptophan to N-formyl-kynurenine, a toxic tryptophan catabolite (20). IDO is overexpressed in various tumor cells in response to cytokines such as interferon-γ, and is considered an immunosuppressive enzyme (21). Although the mechanism by which IDO influences tumor immune response is not completely unveiled, toxic tryptophan catabolites produced by IDO seem to be released by tumor cells and inhibit activation of CD8+ CTLs or NK cells, and promote the conversion of naive CD4+ T cells to Treg cells (21 –23). However, there have been no studies on IDO expression in PTMC, its effect on infiltration of TIL subsets, or its relationship with clinicopathologic features of PTMC.
In this study, therefore, we investigated the relationship between the expression of IDO and infiltration of T cell subsets in PTMCs and analyzed the relationship of these immunomodulating factors with clinicopathologic parameters of PTMCs.
Materials and Methods
Case selection
A total of 339 consecutive cases of PTMC were collected from files of the Department of Pathology, Seoul National University Bundang Hospital (Seongnam, South Korea) between January 2007 and December 2007. Medical records, pathology reports, and hematoxylin and eosin (H&E)-stained slides were reviewed, and clinicopathologic data, including age, size of tumor, ETE, encapsulation, tumor multifocality, lymph node metastasis, and presence or absence of Hashimoto's or chronic lymphocytic thyroiditis, were obtained. Of the 339 PTMCs, 51 tumors (15.0%) exhibiting histologic findings of Hashimoto's or chronic lymphocytic thyroiditis, including oxyphilic change of follicular cells and extensive lymphocytic infiltration with germinal center formation within tumor and in peritumoral areas, were excluded, as it was difficult to discriminate the TILs from lymphocyte infiltrations associated with autoimmune thyroiditis. However, tumors that were clearly separate from the foci of background autoimmune thyroiditis were included. Moreover, incidentally found papillary microcarcinomas after surgery of other thyroid disease and small tumors with only one tumor block were excluded from the study. Finally, a total of 124 cases of PTMC were included in this study. The clinicopathologic characteristics are summarized in Table 1. In cases with multiple tumor foci, the largest tumor was regarded as the representative lesion. Tumors were considered to display ETE when the tumor cells extended into sizable blood vessels and nerves in the perithyroidal soft tissues or skeletal muscles, as previously reported (24). Lymph node dissection or sampling was performed in 114 cases. In the 10 cases where lymph node status was unknown, follow-up ultrasounds of the neck revealed no evidence of lymph node metastasis and were thus regarded free of lymph node metastasis. This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital, and informed consent was waived.
Tissue array methods
All tissue samples in the study had been fixed in 10% neutral-buffered formalin and embedded in paraffin. The original H&E-stained slides and corresponding clinicopathologic information were fully reviewed by two pathologists (H.S.R and S.Y.P), and the representative areas were marked for tissue array construction. The representative core tissue specimens (4 mm in diameter) were taken from individual paraffin blocks from the largest nodule in primary sites and rearranged in new tissue array blocks using a trephine apparatus (Superbiochips Laboratories, Seoul, South Korea). Non-neoplastic thyroid tissue was included in each of the array blocks.
Immunohistochemistry
Immunohistochemistry was performed on thin sections (4 μm) of tissue arrays, after staining optimization using positive and negative controls and serial dilution. As a positive control for IDO immunostaining, tissue sections of normal human placenta were used. For CD3, CD8, and FOXP3, non-neoplastic tonsil was used as a positive control. As a negative control, non-immune serum was substituted for the primary antibody. Tissue array slides were then immunohistochemically stained with four commercially available antibodies: IDO (Clone 10.1; 1:50 dilution; Millipore, Billerica, MA), CD3 (Clone SP7; 1:150 dilution; Thermo Scientific, Waltham, MA), CD8 (Clone C8; ready to use; Dako, Carpinteria, CA), and FOXP3 (Clone 236A/E7; 1:100 dilution; Abcam, Cambridge, United Kingdom). Briefly, sections from array blocks were submitted to routine immunohistochemical techniques, including deparaffinization and rehydration in graded ethanol. Antigen retrieval was performed by immersing the slides in citrate buffer (pH 6.0) or in Tris-EDTA buffer (pH 9.0) for 40 min in a steamer. Endogenous peroxidase activity was blocked with a 3% H2O2-methanol solution, and the slides were incubated in 10% normal goat serum for 30 min to prevent nonspecific staining. They were then incubated for 1 h at room temperature with appropriately diluted primary antibody. Thereafter, the sections were incubated with horseradish peroxidase-labeled polymer conjugated with secondary antibodies (Dako Envision detection kit; Dako) for 30 min. Diaminobenzidine was used as a chromogen, and the sections were counterstained with Mayer's hematoxylin.
Evaluation of immunohistochemistry
Immunohistochemical scoring of IDO was based on a semi-quantitative method according to the percentage of positive cells and the intensity of staining in tumor cells. The percentage of positive cells was scored as follows: 0, no staining or staining in <10% of the tumor cells; 1, staining in 10–25% of the cells; 2, staining in 26–50% of the cells; 3, staining in 51–75% of the cells; 4, staining in >75% of the cells. The staining intensity was scored as 0 (negative), 1 (weak), 2 (moderate), or 3 (strong). For statistical analysis, cases with ≥10% of positive tumor cells with any intensity were grouped as positive, as previously reported (25). Tissue sections containing tumor were scanned to ascertain areas with highest infiltration of CD3+, CD8+, and FOXP3+ lymphocytes. The number of CD3+, CD8+, and FOXP3+ T cells was determined by counting three hot spots, including intratumoral and peritumoral stromal areas in high-power fields (400×) using UTHSCSA Image Tool software v3.0, and average values of CD3+, CD8+, and FOXP3+ T cells per field, and the ratios of FOXP3+/CD8+, FOPX3+/CD3+, and CD8+/CD3+ T cells were calculated. For statistical analysis, patients were divided into CD3+, CD8+, or FOXP3+ lymphocyte high and low groups, and FOXP3+/CD8+, FOPX3+/CD3+, and CD8+/CD3+ ratio high and low groups using mean cell number of T cell subsets or mean ratio in total cases as cutoff point.
Slides were concurrently evaluated by two pathologists (H.S.R and S.Y.P) who were blinded to clinicopathologic features of the tumor. If there was a discrepancy in the interpretation, evaluation was repeated until a consensus was obtained.
Detection of BRAF mutation
Genomic DNA was extracted from the paraffin-embedded tissues. Briefly, the tumor areas were marked using 4 micron-thick H&E stained sections as a guide. Then, the marked areas were matched with de-waxed but unstained 20 μm-thick sections. The tumor areas were dissected from the unstained slides and transferred into Eppendorf tubes. After the dissection, the blocks were cut into 4 μm sections for H&E staining to confirm the tumor continuity. All samples were then deparaffined with pure water for 10 min at 70°C, and centrifuged at 10,000 g for 10 min. Pellets were treated with 20 μL of instagene matrix (Bio-Rad, Hercules, CA). The samples were incubated at 56°C for 30 min, then 100°C for 10 min, and centrifuged at 10,000 g for 10 min to collect DNA. A 5 μL aliquot of each sample was used for polymerase chain reaction (PCR) amplification.
Each PCR mixture contained the forward and reverse primers (20 pmol each), 25 mmol each of deoxynucleotide triphosphate, 50 mmol MgCl2, and 10× PCR buffer, 5 U Immolase DNA polymerase (Bioline, Taunton, MA), and 10 μL genomic DNA in a total volume of 55 μL. The PCR products were electrophoresed in a 2% agarose gel to confirm successful amplification of the PCR product. The biotinylated PCR product (20 μL) was attached to streptavidin-Sepharose™ High Performance (GE Helthcare, Uppsala, Sweden) according to the standard protocol by incubating them together at room temperature for 10 min (with shaking) in binding buffer. The streptavidin-Sepharose beads were captured using a PyroMark Q24 mdx Vacuum Workstation (Qiagen GmbH, Sweden) with a 24 vacuum probe. This tool was also used for incubation (10 sec) of the biotin-streptavidin complex in 70% EtOH before washing in annealing buffer. Subsequently, the samples were hybridized to 10 pmol of the sequencing primers in annealing buffer at 85°C for 2 min, and this was followed by cooling to room temperature. The PCR primers and sequencing primer sequences were as follows: exon 15 (T1799A) forward, 5′-biotin CTT CAT AAT GCT TGC TCT GAT AGG-3′; exon 15 (T1799A) reverse, 5′-GGC CAA AAA TTT AAT CAG TGG AA-3′; and sequencing reverse, 5′-CCA CTC CAT CGA GAT T-3′. Pyrosequencing was performed using a PyroMark Gold Q24 Reagents (Qiagene GmbH) and PyroMark Q24 mdx the system (Qiagene GmbH), and this was confirmed by visual analysis.
Statistical analysis
Statistical analysis was performed using SPSS v16.0 (SPSS, Inc., Chicago, IL). Spearman's correlation test was used to evaluate the correlations between the expression of IDO and infiltration of FOXP3+, CD3+, and CD8+ TIL. The chi-square test or Fisher's exact test was used to evaluate the association between the clinicopathologic parameters, the expression of IDO, the level of CD3+, CD8+, and FOXP3+ TIL, and the ratio of FOXP3+/CD8+, FOPX3+/CD3+, and CD8+/CD3+ T cells. The number of CD3+, CD8+, and FOXP3+ TIL was also compared by Mann–Whitney U-test according to clinicopathologic parameters. To detect independent predictive factors for aggressive features of PTMC, including ETE, tumor multifocality, and lymph node metastasis, multivariate binary logistic regression analyses were performed. The covariates, which were statistically significant in the univariate analyses, were included in the multivariate analysis. Odds ratios (OR) and their 95% confidence intervals (CI) were estimated for each factor. p-Values of <0.05 were considered statistically significant.
Results
Immunohistochemical expression of IDO and T cell subsets in PTMC
IDO expression was found in the cytoplasm of tumor cells. Eighty-six cases were scored as 0 (69.4%), 21 cases as 1 (16.9%), 11 cases as 2 (8.8%), four cases as 3 (3.3%), and two cases as 4 (1.6%) in terms of proportion of positive tumor cells. Thus, increased expression of IDO was detected in 38 (30.6%) cases of PTMC (Fig. 1A and B). CD3+, CD8+, and FOXP3+ T cells were detected within cancer cell nests, as well as in the peritumoral stroma (Fig. 1C–H). The mean number of tumor-infiltrating CD3+ and CD8+ T cells was 35.3 (range 1.0–399.5) and 13.4 (range 0–80.0). The mean number of tumor-infiltrating FOXP3+ Treg cells was 10.9 per a high power field (range 0–37.5). Using the mean number of TIL subsets as a cutoff point, tumors were classified as CD3+, CD8+, or FOXP3+ lymphocyte high or low groups, and high infiltration of CD3+, CD8+, and FOXP3+ T cells was found in 67 (54.0%), 40 (32.2%), and 47 (37.9%) cases of PTMC respectively.
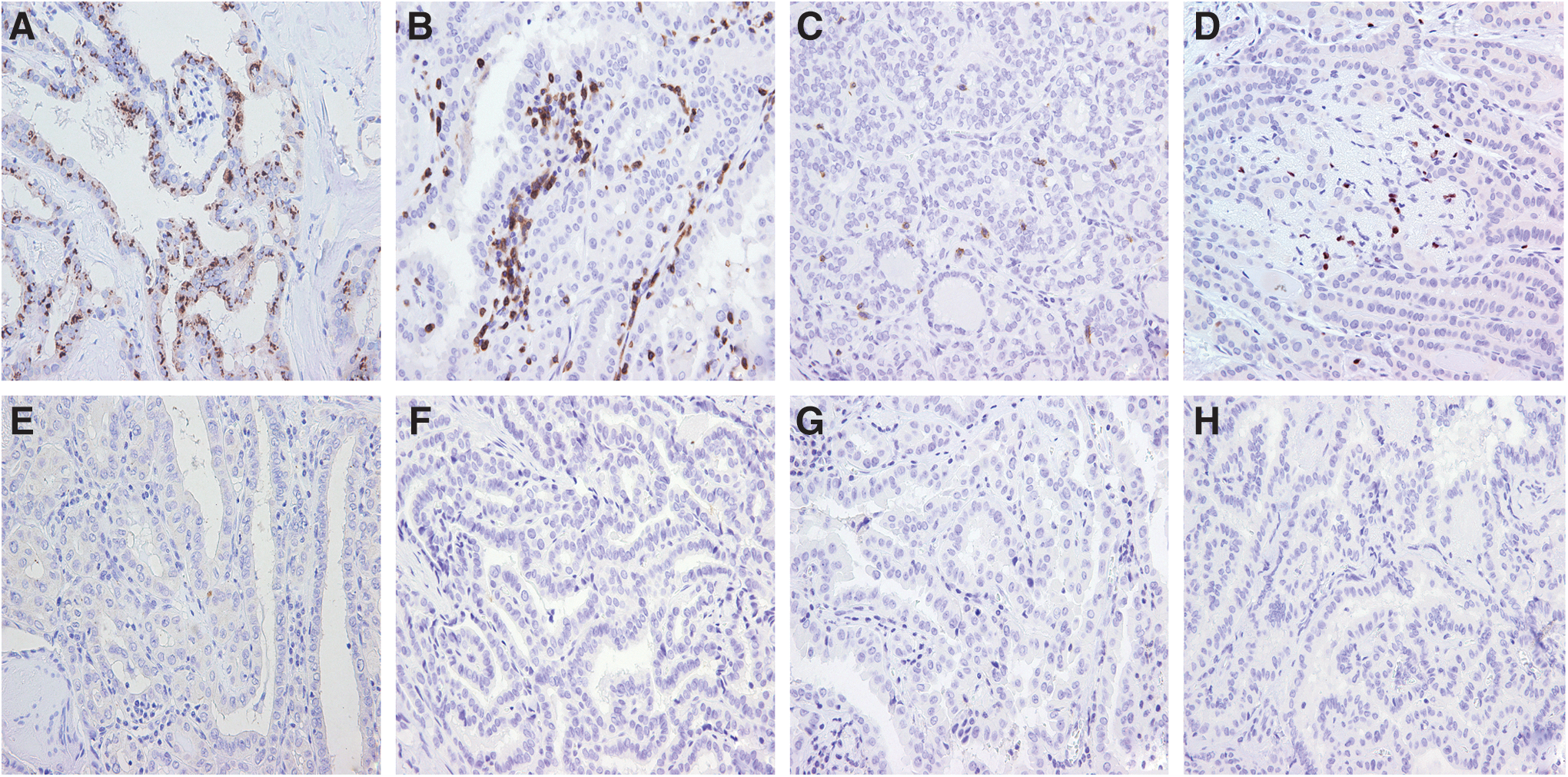
Representative examples of indoleamine 2,3-dioxygenase (IDO) expression and infiltration of CD3+, CD8+, and FOXP3+ tumor infiltrating lymphocytes (TIL) in papillary thyroid microcarcinoma. Whereas some tumors reveal high expression of IDO and high infiltration of CD3+, CD8+, and FOXP3+ TIL
Correlation of IDO expression and infiltration of T cell subsets
To evaluate the effect of IDO expression in PTMC on the infiltration of TILs, we investigated the relationship between IDO and T cell subsets. The expression of IDO and infiltration of FOXP3+ Treg cells had a clear positive correlation with each other (ρ=0.562, p<0.001). On the contrary, expression of IDO and infiltration of CD3+ T cells showed a negative correlation (ρ=−0.229, p=0.010). IDO expression and CD8+ CTL infiltration revealed no correlation. Infiltration of FOXP3+ Treg cells had an inverse correlation with the presence of CD8+ TIL (ρ=−0.184, p=0.041) and CD3+ TIL (ρ=−0.213, p=0.017). CD8+ CTL infiltration was positively correlated with CD3+ T cell infiltration (ρ=0.429, p<0.001).
Association of IDO expression and infiltration of T cell subsets with clinicopathologic features of the tumor
To characterize the cases with increased expression of IDO and increased infiltration of T cell subsets, we analyzed the relationship between the expression of the markers and various clinicopathologic features of the PTMC related to aggressive behavior. IDO expression was significantly associated with ETE (p<0.001) and multifocality (p<0.001; Table 2). High infiltration of FOXP3+ Treg cells was associated with ETE (p=0.002), multifocality (p<0.001), and lymph node metastasis (p=0.021; Table 3). Furthermore, infiltration of FOXP3+ Treg cells was higher in the cases with lymph node metastasis more than three (p=0.002), and tended to be high in those with lateral metastasis (p=0.154). Using the Mann–Whitney U-test, we also found that the number of FOXP3+Treg cell infiltrate was higher in cases with ETE, multifocality, or nodal metastasis than in those without such features (p=0.007, p=0.002, and p<0.001 respectively; Fig. 2). However, CD3+ and CD8+ TIL did not correlate with clinicopathologic features of PTMC, with the exception of the negative correlation of CD3+ TIL and tumor multifocality (Table 3).
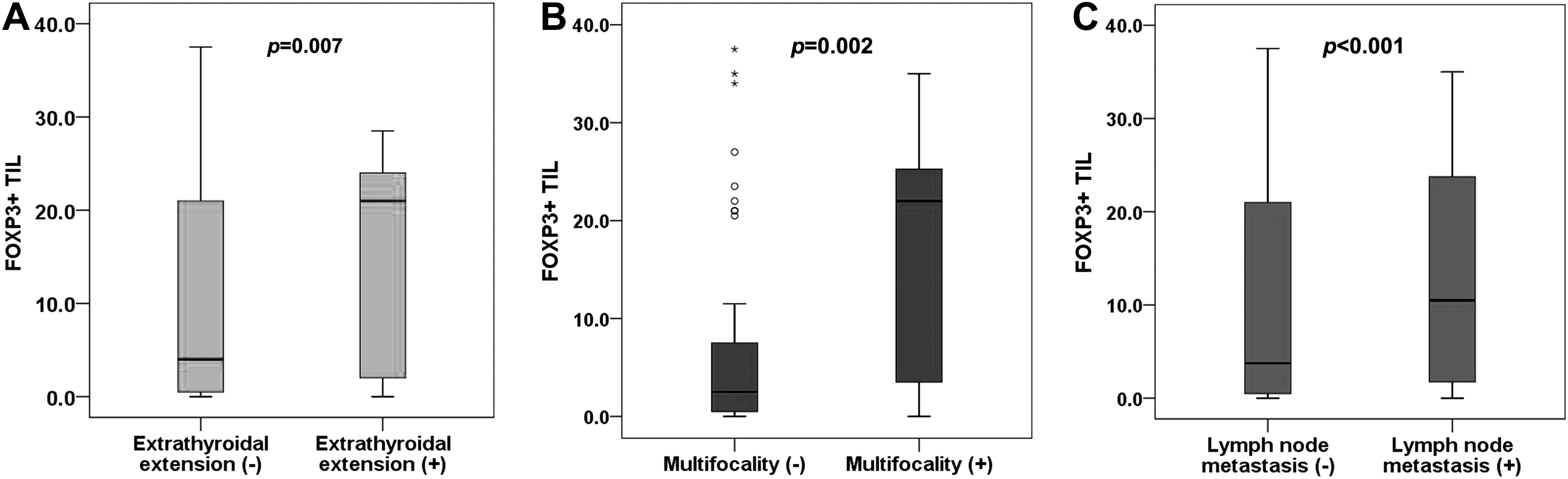
Box plots of the number of FOXP3+ tumor-infiltrating lymphocytes in relation to extrathyroidal extension, multifocality, and nodal metastasis. The group displaying extrathyroidal extension
Numbers in parenthesis indicate column percentage.
BRAF V600E mutational status is available in 100 cases.
IDO, indoleamine 2,3-dioxygenase.
Numbers in parenthesis indicate column percentage.
BRAF V600E mutational status is available in 100 cases.
As the infiltration of T cell subsets was correlated with each other, we also analyzed the relationship between the ratios of T cell subsets (FOXP3+/CD8+, FOXP3+/CD3+, and CD8+/CD3+) and clinicopathologic features of PTMC. High FOXP3/CD8+ ratio was associated with multifocality (p=0.001) and lymph node metastasis (p=0.002), and high FOXP3+/CD3+ ratio was related to ETE (p=0.030) and multifocality (p<0.001). A high CD8+/CD3+ ratio showed a relationship with small tumor size (p=0.032; Table 4).
Numbers in parentheses indicate column percentage.
FOXP3+/CD8+ ratio is not calculated in four cases because there is no infiltration of CD8+ T cells.
BRAF V600E mutational status is available in 100 cases.
As a next step, IDO expression and high FOXP3+ Treg cell infiltration together with significant clinicopathologic parameters were subjected to multivariate logistic regression analyses to find independent predictive factors for aggressive features of PTMC. In multivariate analysis including IDO expression, high FOXP3+ Treg cell infiltration, and tumor multifocality, only IDO expression (OR 4.592; 95% CI, 1.433–14.713; p=0.010) was found to be an independent predictive factor for ETE. And in the multivariate analysis encompassing IDO expression, high FOXP3+ Treg cell infiltration and ETE, IDO expression (OR, 27.880; 95% CI, 5.665−137.206; p<0.001) and high FOXP3+ Treg cell infiltration (OR, 5.564; 95% CI, 1.907–16.234; p=0.002) were revealed as independent predictive factors for tumor multifocality. However, for lymph node metastasis, only high FOXP3+ T cell infiltration showed a positive relationship in this study, and thus multivariate analysis was not performed.
Discussion
A relationship between IDO and antitumor immunity has been proposed in recent studies (22,23). IDO released from tumor cells seems to be related to the suppression of cytotoxic function of T lymphocytes against tumor cells (26). Thus, IDO has been suggested as a potential target for antitumor therapy in previous studies (27,28). In the present study, increased IDO expression in PTMC of the thyroid was associated with more aggressive clinicopathologic features, including tumor extension to perithyroidal soft tissues and multifocality, as an independent predictive factor. Some recent studies have reported that IDO expression in tumor cells correlated with increased risk of lymph node metastasis in other malignancies (25,29,30). Inaba et al. (31) also reported that peritoneal dissemination was significantly increased among ovarian cancer cells that express IDO in animal studies. However, there are also some reports that have shown no significant association between IDO expression and clinical variables of the tumors (32,33). Nevertheless, a significant adverse role of IDO expression on prognosis has been consistently identified in various studies (29,32,34,35).
Although there exist conflicting data regarding the clinical implications of FOXP3+ Treg cells (36,37), the adverse role of FOXP3+ Treg cells in clinical outcomes is generally being accepted (15 –17). Previous studies demonstrated that an increased number of FOXP3+ Treg cells was associated with a higher rate of lymph node metastasis and advanced disease stage in PTC (18,19). We also found that high infiltration of FOXP3+ Treg cells was significantly associated with increased lymph node metastasis, ETE, and tumor multifocality. Furthermore, high infiltration of FOXP3+ Treg cells was associated with a large number of lymph node metastasis. Equally worth noting is the fact that the infiltration of FOXP3+ Treg cells was inversely correlated with the infiltration of CD8+ CTL, which is a crucial component of antitumor immunity, and a high FOXP3/CD8+ ratio was associated with tumor multifocality and lymph node metastasis. Taken together, FOXP3+ Treg cells seem to be associated with tumor progression and aggressive behavior of PTMC. However, Cunha et al. (38) reported that FOXP3+ lymphocytic infiltration was associated with less aggressive features of PTC, such as small tumor size and absence of extrathyroidal invasion. This finding, which conflicts with the results from our study, may be related to the difference in the selection of fields for counting of TIL (unselected spot vs. hot spot), and inclusion or exclusion of cases with Hashimoto's or chronic lymphocytic thyroiditis.
Interaction between tumor-associated IDO expression and T cells appears to be important in inhibiting the activity of NK and cytotoxic T cells and in promoting conversion of naive CD4+ T cells into FOXP3+ Treg cells (21 –23). Our study revealed that IDO expression correlates with a significant increase in FOXP3+ Treg cells and reduction in CD3+ T cells in PTMC. In accordance with our results, previous studies have shown that the expression of IDO correlates with reduced infiltration of CD3+ T cells and increased infiltration of FOXP3+ T cells in other malignancies (35,39,40). However, one study has shown conflicting results on the relationship between IDO expression and infiltration of FOXP3+ Treg cells (41). Although IDO expression proved to be a predictive marker for shorter survival in vulvar cancer, the authors failed to show a significant relationship between IDO expression and FOXP3+ Treg cells. Thus, the role of IDO on the accumulation of Treg cells and reduction of T cells, especially CTL, in tumors should be demonstrated in further studies.
Our study has some limitations regarding the clinical significance of IDO expression and FOXP3+ Treg cells in PTMC, since the data contain no information concerning their relationship with the patients' clinical outcomes. The cases included in this study were relatively recent in onset, and there were no recurrences or metastases during the five-year follow-up, as most PTMCs show indolent clinical courses. Thus, it was impossible to correlate the expression of IDO or the infiltration of FOXP3+ Treg cells with clinical parameters of the tumor, including recurrence or metastasis. Furthermore, although multivariate analyses were conducted to identify independent predictive factors for aggressive features of PTMC, variables included in the analyses were limited to IDO expression, FOXP3+ Treg cell infiltration, and a few clinicopathologic variables, and multivariate analysis was not conducted for lymph node metastasis. Therefore, a large-scale study is needed to confirm the role of IDO expression and FOXP3+ Treg cell infiltration as predictive factors for aggressive PTMC. Moreover, in the present study, 44 cases of PTMC with background Hashimoto's or chronic lymphocytic thyroiditis were included. Although we selected representative samples for tissue array analysis with the PTMC lesion clearly separate from the background Hashimoto's thyroiditis in order to distinguish TILs from lymphocyte infiltrations associated with autoimmune thyroiditis, there may be a limitation in the distinction of the two entities. A further large study dividing patients according to the presence of background autoimmune thyroiditis is necessary.
In summary, we have shown the expression of IDO in PTMC, its association with more aggressive clinicopathologic features, and the relationship of IDO with FOXP3+ Treg cells. These findings suggest that disruption of antitumor immunity by IDO expression and thus infiltration of FOXP3+ Treg cells may contribute to disease progression in PTMC, and that suppression of IDO expression may offer a venue for the development of more effective therapeutic agents against aggressive PTMC.
Footnotes
Author Disclosure Statement
All authors have no conflicts of interest.