
Abstract
Background:
We studied the frequency of thyrotropin (TSH) receptor mutations in hyperthyroid patients with diffuse goiter and negative TSH receptor antibodies (TRAb), and the clinical pictures of the hyperthyroid patients in the presence and absence of mutations.
Patients and Methods:
From 2003 through 2012, 89 hyperthyroid patients with diffuse goiter and negative TRAb based on a second- or third-generation assay underwent sequence analysis of the TSH receptor gene from peripheral leukocytes. The outcome of hyperthyroidism in patients with a TSH receptor mutation and their affected family members was compared with that in patients without any mutation after a 1–10-year follow-up.
Results:
Germline mutations of the TSH receptor occurred in 4 of the 89 patients (4.5%), including 3 definitive constitutively activating mutations (L512Q, E575K, and D617Y). The main difference in the clinical outcome of hyperthyroidism was that no patients with a TSH receptor mutation achieved euthyroidism throughout the follow-up, while 23.5% of patients without any mutation entered remission. The progression from subclinical to overt hyperthyroidism was not significantly different between patients with or without a mutation. Meanwhile, 10.3% of TRAb-negative patients without any TSH receptor mutation developed TRAb-positive Graves' hyperthyroidism during the follow-up.
Conclusions:
The prevalence of nonautoimmune hyperthyroidism with TSH receptor mutations is lower than that of latent Graves' disease in TRAb-negative patients with hyperthyroidism. However, all affected patients with a TSH receptor mutation showed persistent hyperthyroidism regardless of subclinical or overt hyperthyroidism throughout the follow-up.
Introduction
T
Among disease categories of hyperthyroidism that present with negative TRAb and diffuse goiter, nonautoimmune hyperthyroidism and a subset of toxic multinodular goiters with homogeneous distribution of the tracer on thyroid scintigraphy are known. Constitutively activating germline mutations of the TSH receptor (TSHR) gene have been identified as a molecular cause of nonautoimmune hyperthyroidism, while constitutively activating somatic mutations of the TSHR gene are detected in approximately half of toxic multinodular goiters. Serum TRAb levels gradually decrease in 80% of patients with Graves' disease during treatment with antithyroid drugs, and are often undetectable at the remission stage (3,4). In contrast, there are a small proportion of patients with Graves' disease in whom TRAb become positive after treatment with antithyroid drugs (5). Therefore, these patients with latent Graves' disease may also present with negative TRAb during their clinical courses.
In nonautoimmune hyperthyroidism, the severity of hyperthyroidism and goiter size are variable, even among family members harboring the same mutation. The absence of autoimmune parameters may be a major clue for identifying possible patients with nonautoimmune hyperthyroidism. However, the prevalence of germline mutations of the TSH receptor among hyperthyroid patients with negative TRAb and diffuse goiter is uncertain. Here, we first studied the frequency of germline mutations of the TSHR gene in patients described above. Then, the clinical pictures of hyperthyroidism were compared in patients with and without TSH receptor mutations.
Patients and Methods
Patients
From 2003 through 2012, in total 24,623 patients with hyperthyroidism were initially referred to Kuma Hospital. In subjects with subclinical or overt hyperthyroidism, we encountered 89 patients (13 men and 76 women; aged 40±12.5 years [median±quartile deviation]; 2–79 years [range]) who were unlikely to have Graves' disease or toxic multinodular goiter based on the clinical data shown in Table 1. The age of the patients at the diagnosis of hyperthyroidism was 34±11 years. Sequence analysis of the TSHR gene was carried out for these patients, after an interval of 2±2 years. When a germline mutation was detected in a patient, a family screening test for the mutation was carried out involving all available family members (n=15, aged 38±12.5 years; Fig. 1). The medical history, first-degree family history of hyperthyroidism, and presence of Graves' ophthalmopathy were recorded. The clinical courses of all affected patients with TSH receptor mutations and those of patients without any mutation were followed up.
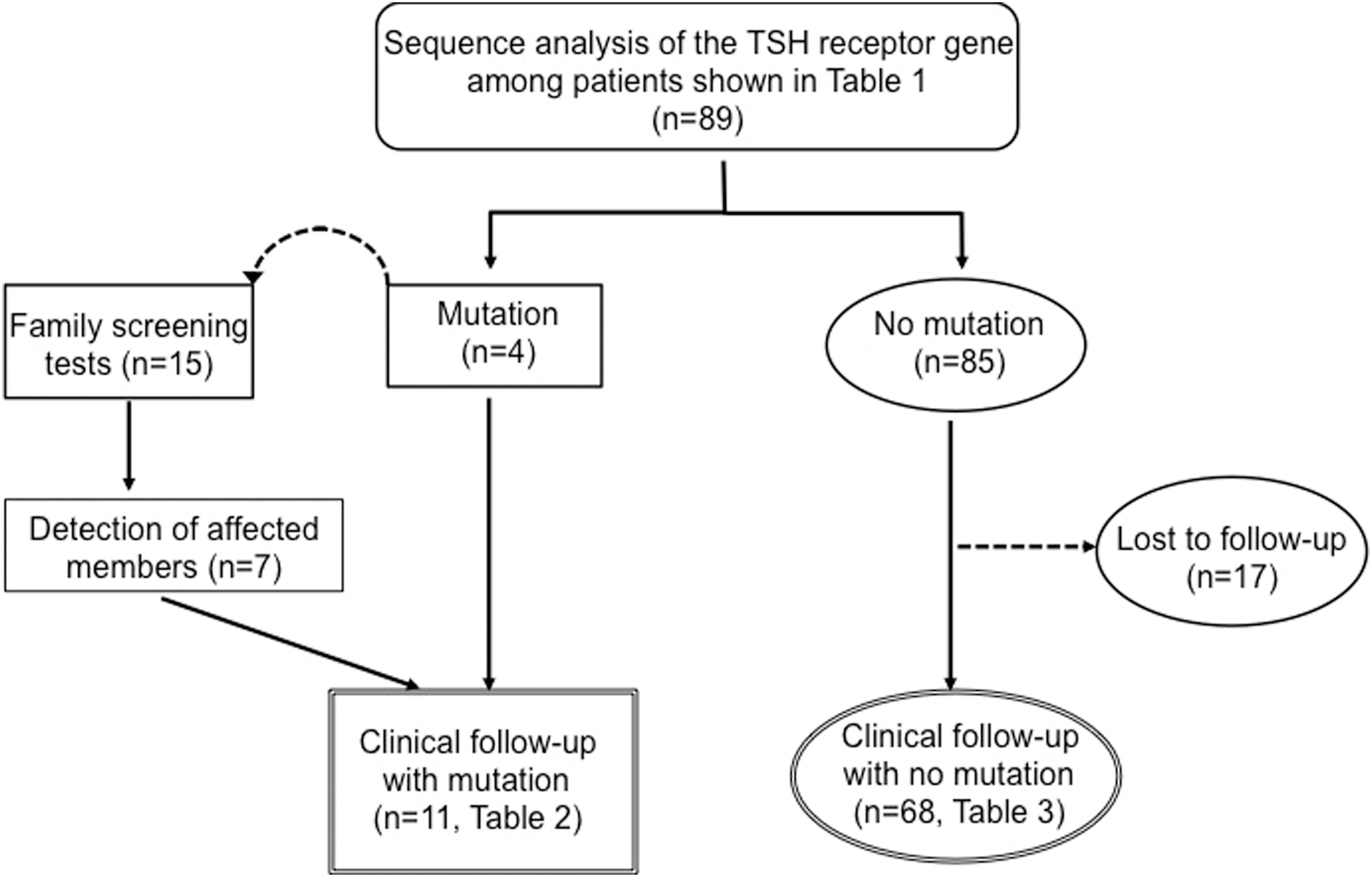
Flow chart of the study population. TSH, thyrotropin.
Persistent hyperthyroidism for more than 1 year.
No history of positive findings.
ATD, antithyroid drugs; NT, not tested; RAIU, thyroidal radioactive iodine uptake; TRAb, TSH receptor antibodies; TSH, thyrotropin; US, ultrasonographic findings of the thyroid gland.
Thyroid function analysis and thyroid volume
Concentrations of serum TSH, free triiodothyronine (FT3), and free thyroxine (FT4) were measured with a chemiluminescent immunoassay (Architect i2000; Abbot Japan, Tokyo, Japan). The reference ranges used for serum TSH, FT3, and FT4 were 0.30–5.00 μIU/mL, 1.70–3.70 pg/mL, and 0.70–1.60 ng/dL, respectively. Subclinical hyperthyroidism was diagnosed based on a suppressed TSH with normal FT4 and FT3 levels. Overt hyperthyroidism was diagnosed based on high FT4 and/or FT3 levels combined with a suppressed TSH. The thyroid function of patients receiving continuous administration of antithyroid drugs or who had already undergone ablative therapies such as radioactive iodine and thyroidectomy was also defined as overt hyperthyroidism. Serum TRAb were measured with a second-generation enzyme-linked immunoassay (RSR Ltd., Cardiff, United Kingdom) through July 2008 and with a third-generation electrochemiluminescent immunoassay (Roche Diagnostic, Mannheim, Germany) from August 2008 through December 2012. Serum TSAb were measured with a commercial bioassay kit (Yamasa Co., Chiba, Japan). The upper cutoff limits of values of the second-generation TRAb, third-generation TRAb, and TSAb are 15%, 1.9 IU/L, and 180%, respectively. Serum anti-thyroglobulin antibodies (TgAb) and anti-thyroid peroxidase antibodies (TPOAb) were measured with an electrochemiluminescent immunoassay (ECLusys Anti-Tg and ECLusys Anti-TPO; Roche Diagnostic). The upper cutoff limits of values of TgAb and TPOAb were 39.9 and 27.9 U/mL, respectively. The total thyroid volume was measured using ultrasonography, as reported previously (6).
DNA sequencing
Genomic DNA was extracted from peripheral leukocytes with GenTLE (Takara, Kyoto, Japan). Exons 9 and 10 of the TSHR gene encoding the entire intracellular and transmembrane regions and part of the proximal extracellular domain of the TSH receptor were amplified by the polymerase chain reaction (PCR) using High Fidelity PCR Master (Roche Diagnostic), as described previously (7). Direct sequencing of PCR products was performed using the Bigdye Terminator v1.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, CA) and an automatic ABI 3130 sequencer (Applied Biosystems). The present study was approved by the ethics committee of Kuma Hospital, and informed consent was obtained from the patients and their family members for the use of samples for research purposes.
Statistical analysis
Thyroid volumes were compared using the Mann–Whitney test. The first-degree family history of hyperthyroidism, presence of TgAb and/or TPOAb, stable state of subclinical hyperthyroidism, remission to euthyroidism, and therapeutic modalities were compared between the two groups with the χ 2-test. p<0.05 was accepted as indicating significance.
Results
Sequence analysis of the TSHR gene of the 89 patients led to the identification of 4 mutations in 4 patients (L512Q, E575K, D617Y, and L267F; Table 2). The four patients were heterozygous. The family screening test for each mutation identified two additional patients harboring E575K and five patients harboring D617Y (Figs. 1 and 2). Eleven patients with TSH receptor mutations presented with subclinical or overt hyperthyroidism, but the remaining family members without any TSH receptor mutation were euthyroid. The mutations of L512Q, E575K, and D617Y were confirmed as constitutively active forms by in vitro functional assays (6,8 –10). The proband with L512Q was a de novo case without the presence of a mutation in her parents (Fig. 2A), and had inadequate treatment for congenital hyperthyroidism, which caused bone abnormalities and mental retardation (8). Other probands with a TSH receptor mutation had a first-degree family history of hyperthyroidism (Fig. 2B–D). The in vitro activity of L267F was not tested. The proband's mother had a history of hyperthyroidism but had already died without detailed information. Clinical pictures of patients with TSH receptor mutation were evaluated over a 3–10-year follow-up (Table 2). In 6 patients with subclinical hyperthyroidism at the first examination, 5 patients maintained a stable state of subclinical hyperthyroidism without increasing goiter size, but 1 patient progressed to overt hyperthyroidism at the age of 25 years. Five patients with overt hyperthyroidism at the first examination were treated with continuous medication or thyroid ablation. No patients achieved euthyroidism without treatment throughout their clinical courses. TgAb and/or TPOAb were detected in 2 of 11 patients with a mutation (18.2%; Table 2).
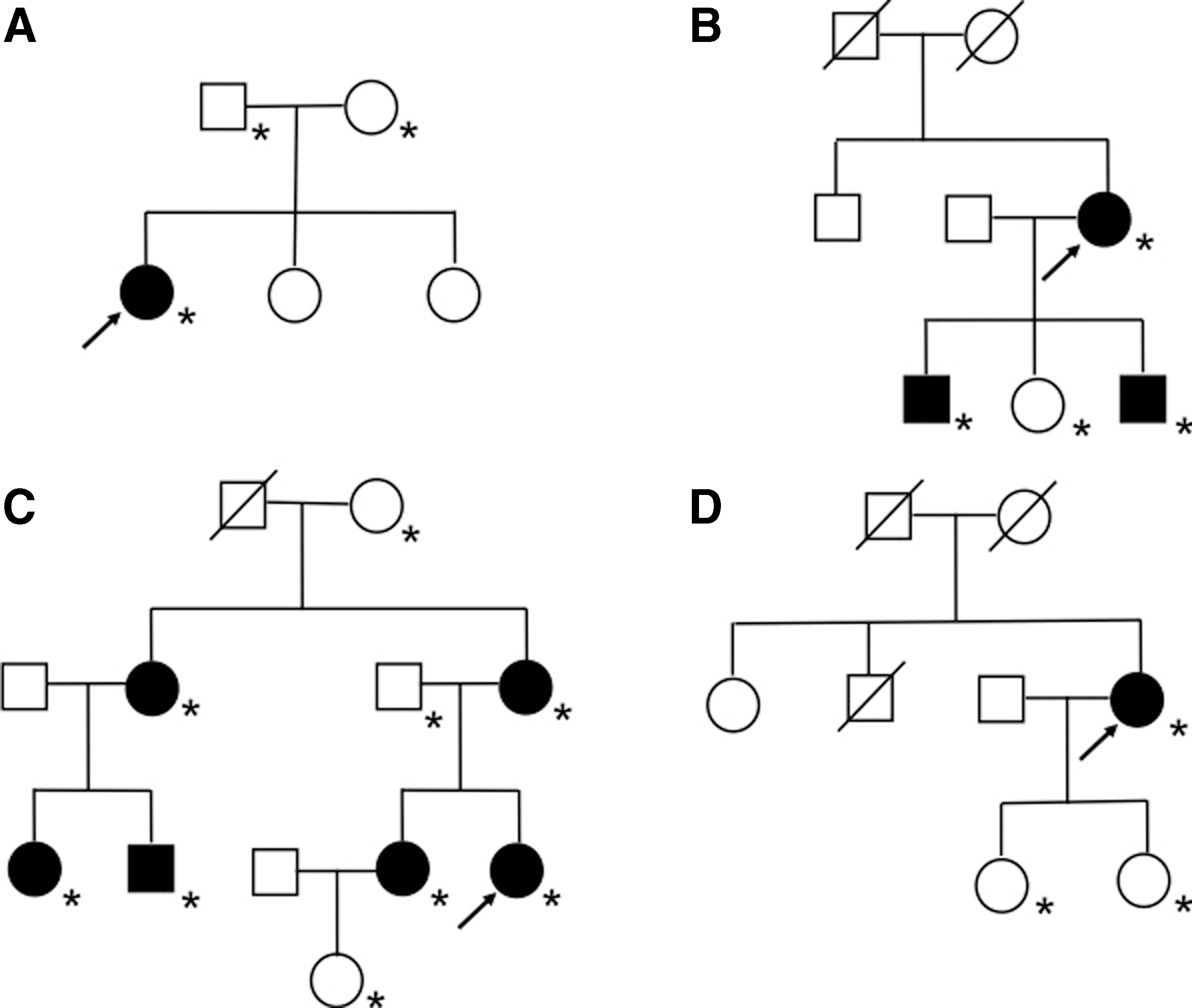
The family pedigrees of patients with TSH receptor mutations.
Mutation affects several members of the same family.
Proband.
Age, age at diagnosis; F, female; KI, potassium iodide; M, male; RI, radioactive iodine therapy; TgAB, anti-thyroglobulin antibodies; TPOAb, anti-thyroid peroxidase antibodies.
In 85 patients without any TSH receptor mutation, clinical follow-up data on 68 patients were available for more than 1 year (median 4.0 years; Fig. 1). TgAb and/or TPOAb were detected in 17 of the 68 patients (25.0%). Throughout their clinical courses, 7 of the 68 TRAb-negative patients (10.3%) developed TRAb-positive Graves' hyperthyroidism. Thereafter, 2 of the 7 patients entered remission within 3 years of antithyroid drug therapy (Table 3). Among 61 patients with persistently negative TRAb, 39 patients (63.9%) were subclinical hyperthyroid or euthyroid. Of 34 patients with subclinical hyperthyroidism at the first examination, 22 (64.7%) patients maintained a stable state of subclinical hyperthyroidism, while 6 patients (17.6%) received medication or underwent ablative therapy, and 6 patients (17.6%) entered remission. Fifty-four of the 61 patients with persistently negative TRAb were tested by the TSAb assay and then 5 patients (9.3%) showed weakly positive TSAb. Among them, four patients entered remission and one patient underwent total thyroidectomy. Subsequently, histopathological examination of this thyroid specimen showed follicular swelling, papillary projection, vacuolated colloid, and lymphocytic infiltration in the stroma, which were compatible with Graves' disease. Histopathological findings of thyroid specimens from six other patients negative for both TRAb and TSAb (Table 3) showed multiple adenomatous nodules but no lymphocytic infiltration in the thyroid gland.
The brackets indicate numbers of patients.
In our study, all subjects were over 19 years old, excluding 2 patients (2 and 6 years old) without any TSH receptor mutation (Fig. 3A). Hyperthyroidism in first-degree family members was detected in 3 of 4 probands with a TSH receptor mutation (75.0%), while it was detected in 26 of 85 patients without any mutation (30.6%; χ 2=3.43, p=0.06). The thyroid volume at the first examination was not significantly different between patients with and without a TSH receptor mutation (Fig. 3B). Therapeutic modalities with no treatment, medication, and ablative therapy for hyperthyroidism were not significantly different between these two groups (Tables 2 and 3; χ 2=2.65, p=0.27). No patients presented with Graves' ophthalmopathy.
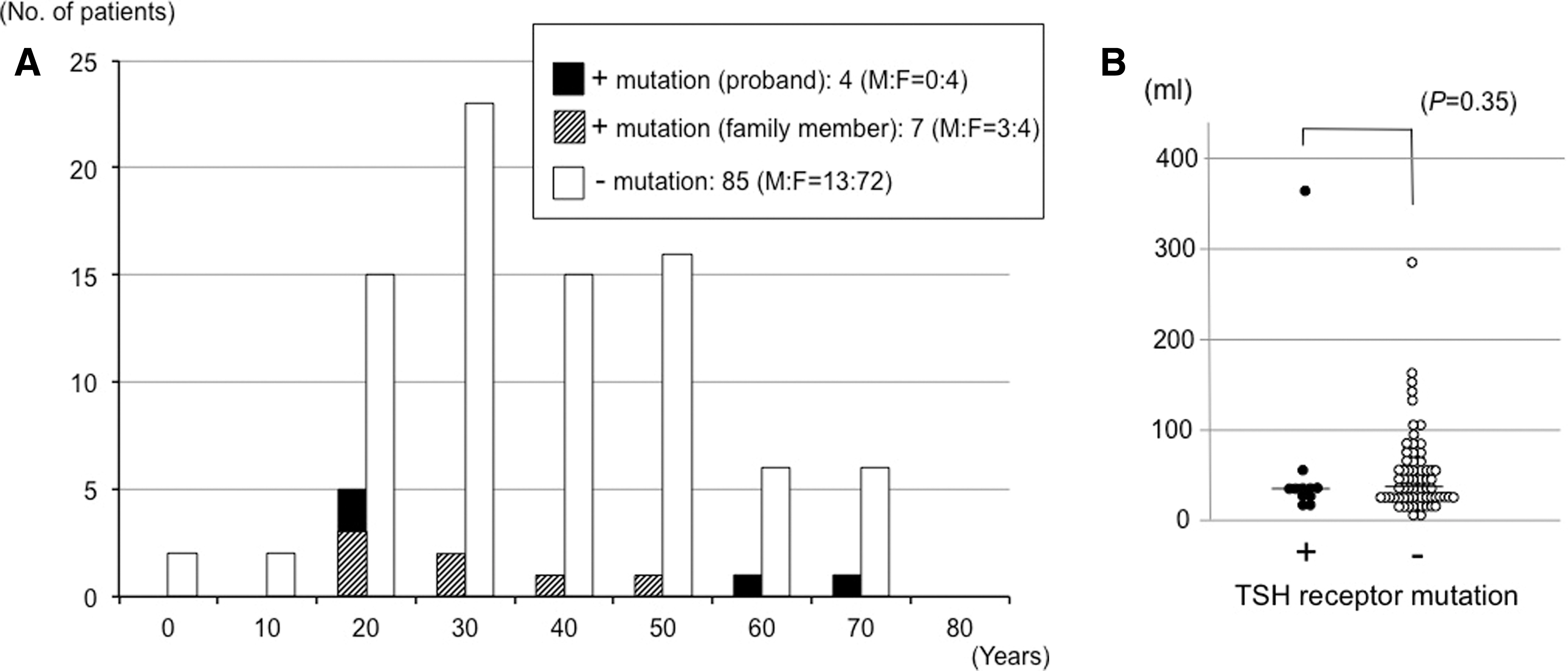
Comparison of the clinical characteristics of patients with or without TSH receptor mutations. Seven patients with a TSH receptor mutation identified in the separate family study were added to the initial 89 patients.
Discussion
The presence of TSH receptor mutations is the primary cause of nonautoimmune hyperthyroidism. In this study, the prevalence of a TSH receptor mutation was 4.5% in 89 hyperthyroid patients who were unlikely to have Graves' disease or toxic multinodular goiter based on the clinical data shown in Table 1. Previous studies concerning nonautoimmune hyperthyroidism were mostly case reports, but the prevalence among patients with hyperthyroidism has been less extensively studied. To our knowledge, only a country-wide screening in Denmark showed that the prevalence of nonautoimmune hyperthyroidism with constitutively activating germline mutations of the TSHR gene was 0.8% in 121 patients with juvenile-onset hyperthyroidism, which corresponds to 5.8% in 17 patients with juvenile-onset hyperthyroidism who do not have thyroid autoantibodies, including TSAb, TgAb, and TPOAb (11). In our study, subjects over 19 years old, excluding 2 patients (Fig. 2A), seem to be an appropriate population because hereditary nonautoimmune hyperthyroidism develops most frequently during adolescence or later (12). Sequence analysis of the TSHR gene in this population gave us a chance to identify not only typical patients with hereditary nonautoimmune hyperthyroidism, but also one patient with unnoticed sporadic nonautoimmune hyperthyroidism. Even in the presence of TgAb and/or TPOAb, nonautoimmune hyperthyroidism can be differentiated from autoimmune thyroid diseases, including painless thyroiditis and the so-called Hashitoxicosis, based on the levels of radioactive iodine uptake and clinical follow-up of the thyroid function. The presence of TgAb and/or TPOAb in patients is not required to exclude the diagnosis of nonautoimmune hyperthyroidism (13 –15). Indeed, 18.2% of the patients with a TSH receptor mutation were concomitantly positive for TgAb and/or TPOAb; the positive rate was not significantly different from patients without any mutation (χ 2=0.24, p=0.62).
In spite of the variable severity of hyperthyroidism among patients with nonautoimmune hyperthyroidism, data from previous reports show that affected adult patients develop almost always overt hyperthyroidism and receive continuous antithyroid drug therapy or ablative therapy (12). Indeed, a 20-year-old patient in this study was finally diagnosed with sporadic nonautoimmune hyperthyroidism with an L512Q mutation following inadequate treatment for congenital hyperthyroidism (8). Immediate diagnosis and initiation of ablative therapy without delay is indispensable to avoid irreversible complications (16 –23). TSH receptor mutations in sporadic cases, including our case, typically have a more severe clinical presentation and much stronger activating effect than those in hereditary cases, which has also been shown by in vitro studies (24). In contrast, 5 of 10 adult patients with hereditary nonautoimmune hyperthyroidism maintained a stable state of subclinical hyperthyroidism without treatment for more than 8 years, which may be dependent on the relatively small increase in constitutive activity of TSH receptor mutations (E575K and D617Y) and other environmental modifiers, including iodine intake (6,7,10). These affected patients with persistently subclinical hyperthyroidism showed no symptoms of hyperthyroidism or complications of cardiovascular diseases such as atrial fibrillation. In our study, more than 60% of patients with subclinical hyperthyroidism did not develop overt hyperthyroidism with either the presence or absence of a TSH receptor mutation (χ 2=0.81, p=0.37). Therefore, these patients with mild hyperthyroidism cannot be accurately classified without molecular analysis of the TSHR gene. No information about in vitro activity of L267F has been obtained yet. L267 is located in the amino-terminal hinge region of TSH receptor ectodomain, where both mechanisms of hormone binding and intramolecular signal transduction toward the serpentine domain are assumed, and naturally occurring pathogenic activating mutations have been reported (25,26).
At the first examination, there were no significant differences in clinical data between patients with and without a TSH receptor mutation. When compared with the thyroid function during follow-up, 23.5% of patients without any TSH receptor mutation entered remission (Table 3), but no patients with a mutation achieved euthyroidism throughout the follow-up (Table 2; χ 2=3.25, p=0.07). Although significance was not noted, persistent hyperthyroidism rather than hormonal levels at the onset may lead to characteristic features in nonautoimmune hyperthyroidism. While a diagnosis of Graves' disease depends on the presence of TRAb, approximately 10% of initially TRAb-negative patients without any TSH receptor mutation turned out to be TRAb positive during the follow-up (Table 3), and 9.3% of patients with persistently negative TRAb were weakly positive for TSAb in our study. The sensitivity of TRAb to diagnose Graves' disease is high but not 100%, especially at its early stage with mild hyperthyroidism or near remission during antithyroid drug treatment (3 –5,27). When considering all patients with positive TRAb or TSAb during the follow-up, or who entered remission without treatment, at least 22 of the 68 patients (32%) without any TSH receptor mutation are considered to have had latent Graves' disease at the first examination. On the basis of periodic follow-up combined with several examinations in persistent TRAb-negative patients, however, the exact etiology of hyperthyroidism remains undefined in more than half of the patients. There is a considerable interindividual variation of the set point of TSH in healthy subjects, which is determined by genetic and environmental factors. Accordingly, a suppressed TSH with normal FT4 and FT3 levels may not always be identical with subclinical hyperthyroidism.
In summary, we focused on patients with subclinical or overt hyperthyroidism with diffuse goiter and negative TRAb in the second- or third-generation assay. In this condition, the prevalence of germline mutations of the TSHR gene is 4.5%. All patients with a TSH receptor mutation were adults at the time of genetic testing and showed persistent hyperthyroidism regardless of the presence of subclinical or overt hyperthyroidism. To address the long-term care of hyperthyroid patients and their affected family members, we should evaluate TSH receptor mutations in persistently TRAb-negative patients with hyperthyroidism, not only in children, but also in adults.
Footnotes
Acknowledgments
We are grateful to Drs. Yuji Nagayama and Basil Rapoport for their excellent in vitro studies to elucidate the constitutive activity concerning D617Y and E575K mutations, respectively, cited herein, as well as to Kuma Hospital staff for their invaluable contribution.
Author Disclosure Statement
The authors declare that no competing financial interests exist.