
Abstract
Background:
Immunoglobulin G4-related disease (IgG4-RD) is a new clinical entity that affects various organs with increased IgG4 positive plasmacytes and progressive fibrosis. While IgG4-RDs in association with Hashimoto's thyroiditis or Riedel's thyroiditis have been reported, the relationship between IgG4-RD and Graves' disease (GD) is yet unknown. To elucidate the relation of GD to IgG4-RD, serum IgG4 levels and their clinical implications in patients with GD were investigated.
Methods:
In this prospective study, serum IgG4 levels were measured in 109 patients with GD and classified into two groups according to the comprehensive diagnostic criteria of IgG4-RD previously established: (i) GD with elevated-IgG4 levels (≥135 mg/dL), and (ii) GD with nonelevated IgG4 (<135 mg/dL).
Results:
Seven out of 109 patients with GD (6.4%) had elevated serum IgG4 levels [mean±standard deviation (range): 175.0±44.5 (136–266) mg/dL] and elevated ratios of IgG4/IgG [12.7±4.5% (7.6%–21.2%)]. The remaining patients with GD had serum IgG4 levels and IgG4/IgG ratios of 39.6±27.6 (3–132) mg/dL and 3.2±2.2% (0.3%–11.5%), respectively. Ages in the elevated IgG4 group were significantly higher than those of the nonelevated IgG4 group: 54.7±6.2 versus 43.4±15.4 years, respectively. Ultrasound examinations revealed that the elevated IgG4 group had significantly increased hypoechogenic areas in the thyroid in comparison to the nonelevated IgG4 group (low echo scoring: 1.66±0.81 vs. 0.61±0.89, respectively). In the correlation analysis, TSAb (r s=0.385, n=42) titers were significantly correlated with serum IgG4 levels, while they were not significantly different between the two groups. In the elevated IgG4 group, symptoms were controllable with a small dose of antithyroidal drug (ATD; n=4), a combination treatment with ATD and L-T4 (n=1), or L-T4 administration only one year after the first visit (n=2).
Conclusions:
A small portion of GD patients harbored elevated serum IgG4 levels. They were older, had increased hypoechoic areas in the thyroid, and appeared to be responsive or prone to be hypothyroid after ATD treatment. Thus, the present study suggests the presence of a novel subtype of GD. Measuring serum IgG4 levels may help to distinguish this new entity and provide potential therapeutic options for GD.
Introduction
I
The relationship between IgG4-RD and thyroid diseases has been previously investigated. Li et al. described a novel type of IgG4 thyroiditis on the basis of its clinical and histopathological features (3). The authors found a close relationship between the fibrous variant of Hashimoto's thyroiditis (HT) and IgG4-RD. Riedel's thyroiditis (RT) has been proposed to be an organ manifestation of IgG4-RD (4,5). In cases of RT, elevated serum IgG4 levels and/or an increased number of IgG4-positive plasmacytes with dense fibrous tissue were observed in the thyroid gland, which would respond to steroid therapy, suggesting characteristics of IgG4-RD (4). In addition, Watanabe et al. reported that 19% of patients with IgG4-RD who had hypothyroidism showed an increased thyroid volume and TgAb and/or TPOAb positivity. The thyroid function of these patients normalized after prednisolone treatment. Furthermore, histology revealed IgG4-bearing plasma cells and loss of thyroid follicles, was the condition was thus termed IgG4-related thyroiditis (6). However, the relationship between IgG4-RD and GD remains unknown.
To elucidate the relationship between IgG4-RD and GD, serum IgG4 levels in 109 patients with GD were measured and compared according to clinical characteristics. Herein, we describe the clinical features of patients with GD and elevated serum IgG4 levels, and discuss diagnostic and therapeutic approaches.
Patients and Methods
Patients
A total of 109 patients with GD at the Wakayama Medical University Hospital, Japan, from January 2011 to October 2012 were prospectively recruited to this study. The diagnosis of GD was based on the presence of hyperthyroidism, positive thyroid stimulating hormone receptor antibody/thyroid stimulating antibody (TRAb/TSAb), and/or increased 123I thyroid uptake. Patients with malignancies or pregnancy were excluded. None of the patients underwent surgery or radioiodine treatment. Patients were divided into two groups: those with elevated serum IgG4 levels (≥135 mg/dL) and those with nonelevated serum IgG4 levels (<135 mg/dL) according to the comprehensive diagnostic criteria of IgG4-RD, the currently established criteria (7). Masaki et al. proposed that another criterion for IgG4-RD consists of a ratio of IgG4/IgG of≥8.0% (8); this criterion was therefore also considered in our study. Patients were analyzed for age, sex, smoking, familial history of autoimmune thyroid disease (AITD), presence of Graves' ophthalmopathy (GO) on the basis of the clinical activity score (CAS) (9) and NOSPECS (10), serum IgG4 and IgG levels, thyroid function, thyroid autoantibodies, and ultrasound examination (Table 1). Patients were classified according to intractability in the control of hyperthyroidism: group 1 (intractable patients) who required a moderate or large dosage of antithyroidal drug (ATD) (thiamazole (MMI)≥10 mg/day; propylthiouracil (PTU) ≥150 mg/day) to control thyroid function; and group 2 (tractable patients) who could be treated with a small dosage no ATD (MMI ≤5 mg/day; PTU≤100 mg/day). Written informed consent was obtained from all patients, and the study protocol was approved by the Wakayama Medical University Hospital Ethics Committee.
p-Values were obtained using aFisher's exact test, or bMann–Whitney U-test, and p-values<0.05 were accepted as significant, shown in bold.
Thyroid size was measured as the sum of both lobes according to the following equation: anteroposterior×transversal diameters (mm2) at the maximum position.
Degree of low echogenicity in the thyroid gland was determined by ultrasonography as follows: Grade 0, diffuse high-amplitude echoes throughout the whole lobe of the thyroid; Grade 1, low-amplitude and ununiformed echoes in the whole or several regions of the thyroid; Grade 2, several sonolucent regions in the thyroid; and Grade 3, no apparent echoes or very low-amplitude echoes throughout the whole thyroid.
Increase of color Doppler flow in the thyroid gland was determined as follows: 0, none; 1, mild; 2, moderate; and 3, severe.
Since most TSH levels were undetectable, comparison of TSH levels in the two groups was not determined.
Data for TSH, TRAb, TgAb, and TPOAb were analyzed with log-transformed values.
Values of <0.003, <1.0, <5, <10, >30.0, >600, and >4000 were calculated as 0, 1.0, 5, 10, 30.0, 600, and 4000, respectively.
AITD, autoimmune thyroid disease; fT3, free triiodothyronine; fT4, free thyroxine; IgG, immunoglobulin G; IgG4, immunoglobulin G4; NA, not applicable; ND, not determined; SD, standard deviation; TgAb, thyroglobulin autoantibodies; TPOAb, thyroid peroxidase antibodies; TRAb, thyroid stimulating hormone receptor antibody; TSAb, thyroid stimulating antibody; TSH, thyrotropin.
Thyroid function tests and thyroid autoantibodies
Serum thyrotropin (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) levels were measured by chemiluminescent immunoassay (Abbott Diagnostics, Tokyo, Japan). Reference ranges were defined as follows: TSH 0.35–4.94 mIU/L; fT4 0.70–1.48 ng/dL; and fT3 1.71–3.71 pg/mL. TRAb was determined by enzyme-linked immunosorbent assay (Cosmic, Tokyo, Japan). Thyroglobulin autoantibodies (TgAb) and thyroid peroxidase antibodies (TPOAb) were measured with an electrochemiluminescent immunoassay (SRL, Tokyo, Japan). Normal values were defined as follows: TRAb <1 IU/L; TgAb <28 IU/mL; TPOAb <16 IU/mL. TSAb activities were determined using the Yamasa's TSAb bioassay kit (Yamasa Ltd., Choshi, Japan). Normal values for TSAb were defined as <180%.
Serum IgG4 and IgG levels
Serum IgG4 and IgG levels were measured by a nephelometric immunoassay (BML, Osaka, Japan). Reference ranges for IgG4 and IgG were defined as 4–108 mg/dL and 870–1700 mg/dL, respectively. Since comprehensive diagnostic criteria for IgG4-RD include a serum IgG4 level ≥135 mg/dL, we defined this as the cutoff level in this study.
Ultrasonographic evaluation
Ultrasonographic examinations were performed by conventional gray scale and color Doppler, and by 10 MHz linear transducer (Toshiba Medical, Osaka, Japan). Low echogenicity in the thyroid gland was classified into four categories and scored as previously described (11): Grade 0, diffuse high-amplitude echoes throughout the whole lobe of the thyroid; Grade 1, low-amplitude and nonuniform echoes in the whole or several regions of the thyroid; Grade 2, several sonolucent regions in the thyroid; and Grade 3, no apparent echoes or very low amplitude echoes throughout the whole thyroid. Increase of color Doppler flow in the thyroid gland was determined as follows: 0, none; 1, mild; 2, moderate; and 3, severe. Thyroid size was measured as the sum of both lobes according to the following calculation: anteroposterior×transversal diameters (mm2) at the maximum position.
Statistical analysis
Fisher's exact test was used to assess data in the two-dimensional contingency tables for comparison with sex, presence of GO, family history of AITD, and smoking. Mann–Whitney U-test or Kruskal–Wallis test were used to compare two or three individual groups, respectively. Two-tailed Spearman's rank correlation coefficient (r s) was determined to assess the correlation between two variables. Data for TSH, TRAb, TgAb, and TPOAb were analyzed with log-transformed values. p-Values <0.05 were accepted as statistically significant (SPSS v15, Chicago, IL). Data are expressed as mean±standard deviation (SD).
Results
Serum IgG4 and IgG levels in patients with GD
Overall, the serum IgG4 level in patients with GD was 48.3±44.0 mg/dL (range 3–266), and the ratio of IgG4/IgG was 3.8±3.4 mg/dL (range 0.3–21.2; Table 1). Seven (6.4%) of the 109 patients with GD had elevated serum IgG4 levels at 175.0±44.5 mg/dL (range 136–266) and elevated ratios of IgG4/IgG at 12.7±4.5% (range 7.6–21.2). The remaining patients with GD (93.6%) had serum IgG4 levels and IgG4/IgG ratios of 39.6±27.6 mg/dL (range 3–132) and 3.2±2.2% (range 0.3–11.5), respectively. Three cases of GD in patients with serum IgG4 levels <135 mg/dL had serum ratios of IgG4/IgG ≥8%. There was a significant difference in the ratios of IgG4/IgG between the two groups (p<0.001). However, no significant difference was observed in serum IgG levels between groups.
The elevated-IgG4 group consisted of one man and six women, while the nonelevated-IgG4 group included 14 men and 88 women. No significant difference was observed in sex distribution between groups.
The mean age of the elevated IgG4 group was significantly higher than that of the nonelevated IgG4 group: 54.7±6.2 years (range 49–68) versus 43.4±15.4 years (range 13–79), respectively (p=0.026). The number of patients with GO (CAS ≥1) who had a family history of AITD or who were smokers was not significantly different between the two groups (Table 1). Serum TSH, fT3, fT4, TRAb, TgAb, and TPOAb levels did not significantly differ between the elevated and nonelevated IgG4 groups (Table 1). Ultrasound examinations revealed that the elevated IgG4 group had significantly more hypoechogenic areas in the thyroid compared to the nonelevated IgG4 group [low echo scoring: 1.66±0.81 (range 1–3) vs. 0.61±0.89 (range 0–3)], respectively (p=0.005). No significant differences were observed in thyroid size or increase of color Doppler flow between the two groups. We also analyzed the patients based on the IgG4/IgG ratio (ratio ≥8%). The elevated IgG4/IgG ratio group had significantly increased hypoechogenic areas in the thyroid in comparison to the nonelevated IgG4 group (p=0.031), although the ages of the elevated IgG4/IgG ratio group were not significantly higher than those of the nonelevated IgG4/IgG ratio.
Clinical features of patients with elevated IgG4
The clinical characteristics of the seven GD patients with elevated IgG4 are summarized in Table 2. Of these, six patients had an IgG4/IgG ratio of ≥8%, and five had GO (patients 1, 2, 3, 4, and 6). Patient 4 had diplopia; patients 1, 3, and 4 had mild proptosis (17–20 mm); patients 2 and 4 had swollen extraocular muscles and increased orbital fat; patient 6 showed palpebral swelling. TRAb levels were elevated in all seven cases. In patient 3, who spontaneously became hypothyroid in the follow-up of Graves' hyperthyroid patients treated with a maintenance dose (5–15 mg) of methimazole for more than 10 years, TRAb levels were rapidly and remarkably increased in spite of negative TSAb activity, suggesting the presence of blocking-type TRAb. Nonetheless, this patient showed persistent thyroid enlargement with broad hypoechoic areas in both lobes (Fig. 1). The TRAb activity of patient 6 was initially 35.1% as determined by a 1st generation TRAb assay (normal value <10%) when she was thyrotoxic (fT4 4.2 ng/dL). TgAb and/or TPOAb levels were elevated in most cases except for patient 2. In the elevated IgG4 group, patients were treated with a small dose of ATD (patients 1, 2, 4, and 5), MMI and combined L-T4 (patient 7), or L-T4 alone (patients 3 and 6) one year after ATD treatment (Table 2). None of the patients had pretibial myxedema.
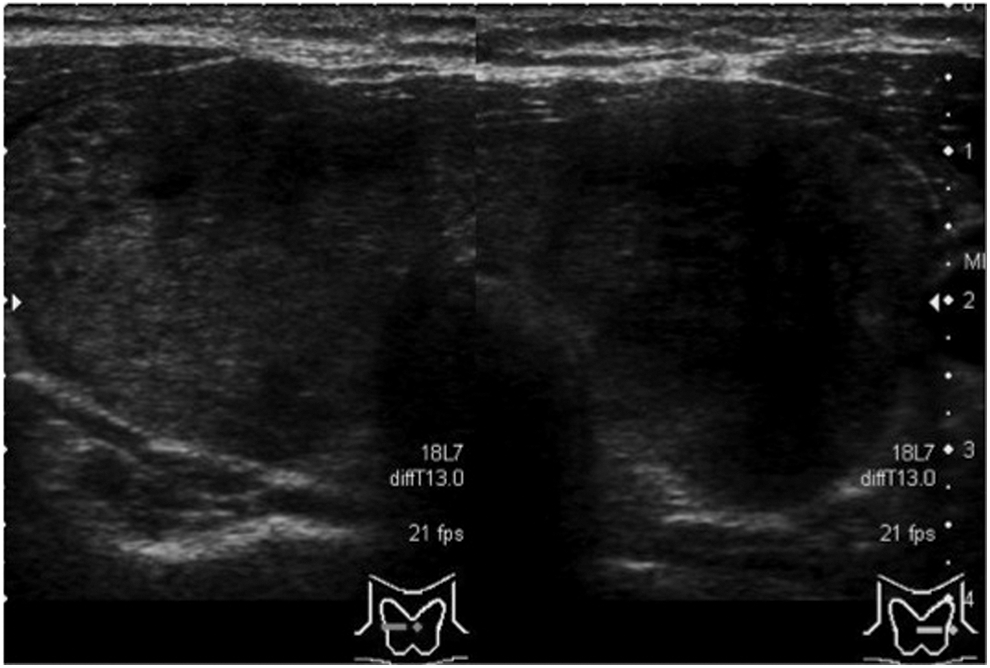
An ultrasonographic image of patient 3. Note that hypoechoic areas are seen throughout both lobes of the thyroid gland.
NOSPECS and CAS are the severity and activity classifications, respectively, of Graves' ophthalmopathy. Exophthalmoses in the right and left eyes measured with the Hertel exophthalmometer are represented as (R, mm) and (L, mm), respectively. In the orbital MRI, the presence of extraocular muscles enlargement and the increase of orbital fat are indicated.
ATD, antithyroid drugs; MMI, thiamazole; ND, not determined; PTU, propylthiouracil; US, ultrasound.
Correlation between serum IgG4 and IgG levels and ratios and other clinical parameters
The TSAb titer correlated significantly with both serum IgG4 levels (r s=0.385, p=0.012, n=42) and IgG4/IgG ratios (r s=0.346, p=0.027, n=41). In addition, in patients with untreated hyperthyroidism (n=42), TSAb titers also significantly correlated with both serum IgG4 levels (r s=0.519, p=0.039, n=16) and IgG4/IgG ratios (r s=0.568, p=0.022, n=16). The TPOAb titer correlated significantly with serum IgG levels (r s=0.2495, p=0.037, n=70), but not with IgG4 levels or IgG4/IgG ratios. No significant correlation of serum IgG4, IgG levels, and the ratios of IgG4/IgG were observed with age, ultrasound findings (thyroid size, low echogenicity, Doppler flow), thyroid hormone levels (fT3, fT4), or TgAb titer. IgG4 levels or IgG4/IgG ratios were not correlated with IgG levels either.
Comparisons of clinical profiles between patients with intractable and tractable GD
Since patients with elevated serum IgG4 appeared to be responsive to ATD or prone to be hypothyroid, patients with GD were divided into two subgroups: group 1 (intractable patients, n=39) and group 2 (tractable patients, n=18). Although not significant, serum IgG4 [70.5±75.1 mg/dL (range 4–266)] and the ratio of IgG4/IgG [5.8±6.1 mg/dL (range 0.4–21.2)] in group 2 tended to be slightly higher than those in group 1 [IgG4 levels 47.2±29.6 mg/dL (range 3–132); IgG4/IgG ratios 3.7±2.4 (0.3–11.5)]. In contrast, serum IgG levels were almost identical within the two groups [group 1 1284.6±237.8 (782–1735); group 2 1219.6±308.9 (774–2928)).
We also classified patients by CAS: patients with CAS=0 (n=80), patients with CAS=1 or 2 (n=17), and patients with CAS ≥3 (n=12). Serum IgG4, IgG levels, and the ratio of IgG4/IgG were not significantly different between the three groups. We also examined orbital magnetic resonance imaging (MRI) scans and NOSPECS in patients with GD, but no clear associations between serum IgG4 levels with findings of orbital MRI or NOSPECS (9) were observed (data not shown).
Next, correlations between serum IgG4, IgG levels, or ratios of IgG4/IgG and other clinical parameters were separately examined in two groups. No obvious correlations were observed in group 1. In group 2, low echoic scores were significantly positively correlated with serum IgG levels (r s=0.851, p=0.001, n=12) but not IgG4. TPOAb titer was significantly correlated with both serum IgG4 levels (r s=0.576, p=0.031, n=14) and IgG levels (r s=0.637, p=0.019, n=13), but not with IgG4/IgG ratios.
Discussion
In the current study, a novel subgroup of patients with GD and elevated serum IgG4 level was identified (6.4% of overall GD patients; Table 1). Yamamoto et al. reported that in healthy controls (n=21), the average serum IgG4 level was 43±31 mg/dL and the ratio of IgG4/IgG was 2.9±1.8% (12). On the basis of these values, in this report, patients with GD demonstrated a higher serum IgG4 level and IgG4/IgG ratios than healthy controls. Moreover, 6.4% of patients had elevated serum IgG4 levels (≥135 mg/dL), which meets the comprehensive diagnostic criteria of IgG4-RD.
The elevated IgG4 group did not demonstrate any male predominance (Table 1). This finding is neither consistent with previous reports on IgG4 thyroidits (3), nor with those on IgG4-RD (2). The average age of patients in the elevated IgG4 group was significantly higher than that in the nonelevated IgG4 group, which is similar to that observed in IgG4-RD (2). In contrast, IgG4 thyroiditis is associated with a younger age (3), although the prevalence of HT increases with age (13). Since serum IgG4 levels do not increase with age (14) and ages were not found to be correlated with IgG4 levels, unknown factors other than aging may contribute to the elevation in IgG4 levels.
TgAb elevation is associated not only with IgG4 thyroiditis (3), but also with IgG4-related thyroiditis (6). In the present study, serum TgAb levels tended to be higher, albeit not significantly, in the elevated IgG4 group than in the nonelevated IgG4 group (Table 1). Given that IgG4 is a dominant subtype of TgAb in patients with GD (15 –17), TgAb may be at least partly a source of IgG4 in patients 1, 3, and 5–7 with TgAb elevation (Table 2). The presence of TPOAb is also associated with GD. In fact, a significant positive correlation between TPOAb and IgG4 or IgG levels in tractable patients.
The TSH receptor (TSH-R) is a crucial antigen for GD (13). Weetman et al. reported that the IgG subclass in TRAb is restricted to IgG1 (18). In contrast, Latrofa et al. reported that TRAb were affinity enriched on recombinant TSHR antigen before IgG subclass analysis (19). Of three sera samples processed, one contained IgG1 only, one IgG1+IgG4, and one only IgG4. Since they studied sera selected for very high TRAb levels, this finding suggests that long-term antigen stimulation may increase TRAb concentrations and eventually lead to subclass switching from IgG1 to IgG4. M22, a stimulating monoclonal anti-TSH-R antibody (TRAb), is found to be IgG1 (20). Although IgG subclasses in TRAb were not investigated in our study, a positive correlation between IgG4 or the ratio of IgG4/IgG and TSAb was observed in overall patients with GD. Patient 2 showed strong TSAb activity in spite of negative TgAb or TPOAb, suggesting that TSAb is at least partly present in the IgG4 fraction. Patient 3, who rapidly changed to hypothyroidism and possessed persistent thyroid enlargement (Fig. 1), is quite similar to recent cases reported independently by Nishihara et al. and Kawashima et al. (21,22). Thus, both in stimulating and blocking TRAbs, IgG4-positive plasma cells may be involved in the pathogenesis of GD.
The exchange of IgG half-molecules among IgG4 results in bispecific characteristics (23). Notably, McLachlan et al. showed that in patients with GO and elevated TRAb, an IgG4 shift toward TgAb was observed (24). We speculate that IgG4 could have a bispecific nature and consist of TgAb and TRAb. Considering that the levels of TgAb and TPOAb, as well as TRAb, are elevated in GD (13), these autoantibodies may be related to bispecific IgG4 molecules. Another biological relevance of this exchange of half-molecules in IgG4 is that it generates antibodies that inhibit formation of large immune complexes and immune inflammation by IgGs of other subclasses (23). For example, Guo et al. reported that the IgG1 but not the IgG4 subfraction of TPOAb is associated with antibody-dependent cytotoxicity (25).
In the present study, ultrasound examination revealed that the elevated IgG4 group had significantly more hypoechoic areas than the nonelevated IgG4 group (Table 1), as similarly observed in IgG4 thyroiditis (3). Moreover, low echo scoring was positively correlated with serum IgG4 levels. Since hypoechoic areas reflect lymphocyte infiltration and fibrosis in the thyroid gland (10), this area may be related to lymphoplasmacytes that produce IgG4 in the thyroid. In the elevated IgG4 group, disease was controlled with low doses of ATD or treatment with ATD and/or L-T4 one year following the first visit (Table 2). In cases of HT, the degree of hypoechoic areas correlated with the prevalence of hypothyroidism, resulting from fibrosis (26). Thus, the clinical course of patients with IgG4 elevation may be related to fibrosis on the basis of ultrasonographic findings, which resemble the alterations found in HT. In this context, the relationship between IgG4 and Hashitoxicosis (27,28), which has concurrent features of GD and HT, should be studied in the future.
There are several limitations of our study. First, there was a lack of pathologic studies performed in the patients. Second, the patients showed an absence of manifestations of other organs in IgG4-RD. Third, the number of patients with elevated IgG4 is rather small. For this reason, there is some concern for either a type I error (false positive) or a type II error (false negative). Finally, information on alterations in serum IgG4 levels during treatment and clinical course was not collected. As a future study, longitudinal follow-up studies to examine pathophysiological relations and therapeutic outcomes are warranted.
In conclusion, the current study proposes a novel subgroup of patients with GD who show elevated serum IgG4 levels. In comparison to the majority of patients with GD, these patients were older, had more hypoechoic areas, and may be responsive to ATD or prone to be hypothyroid after ATD treatment. IgG4-RD generally shows positive response to steroid therapy. In patients with GD and elevated serum IgG4 levels, steroid therapy should be considered to avoid adverse effects of ATD, radioiodine treatment, or surgical intervention. Thus, measurement of serum IgG4 levels may help to distinguish this new entity and may offer diagnostic and potential therapeutic options for GD. Further investigations on the relationship between GD and IgG4-RD using a larger patient population and longer observation times are warranted.
Footnotes
Acknowledgments
We are thankful to Takamasa Minaga, Yuko Matsumoto, Kana Hayakawa, Tomomi Funahashi, Shinsuke Uraki, Syogo Ueda, Seigo Kurisu, Takahiro Hayakawa, Kaori Miyata, Takeshi Shimada, Tatsuya Ishibashi, Tomoyuki Takagi, Takayuki Nakagawa, and the members of The First Department of Medicine for collecting and analyzing data. This work was supported by the Research Program of Intractable Diseases provided by the Ministry of Health, Labor, and Welfare of Japan.
Author Disclosure Statement
No competing financial interests exist.