
Abstract

Radioactive iodine ablation (RIA) has been increasingly utilized as an adjuvant therapy for postoperative patients with differentiated thyroid cancer (DTC) over the last decades. However, the optimal 131I activity needed for successful ablation is still under investigation. The revised American Thyroid Association (ATA) guidelines recommend selective use of RIA therapy for low-risk DTC patients in a dose as low as 30 mCi (1100 MBq) of 131I (1). Here, we report a case of thyroid remnant ablation in a patient who only received a diagnostic dose (4.27 mCi; 158 MBq) of 131I for an imaging study under recombinant human thyrotropin (rhTSH; Thyrogen®) stimulation.
The patient is a 55-year-old female who underwent total thyroidectomy due to a 1.0 cm PTC in the left lobe with negative surgical margins and no evidence of capsular or lymphovascular invasion or extrathyroidal extension. She has a history of breast cancer, obesity, diabetes, hypertension, hypercholesterolemia, and severe three-vessel coronary artery disease. Nearly two months after thyroidectomy, she received an oral dose of 4.27 mCi (158 MBq) sodium 131I under rhTSH stimulation. Laboratory tests showed a TSH of 230.76 μIU/L, a thyroglobulin (Tg) of 3.4 ng/mL, and negative Tg antibodies (TgAb). The 24-hour 131I uptake over the thyroid bed was 4.35%. The first scintigraphy (Fig. 1A) showed a focus of intense 131I activity in the right central neck. The first SPECT/CT image (Fig. 1C) confirmed the presence of 131I-avid soft tissue (approximately 1.06 cm×0.80 cm×0.61 cm; calculated tissue volume of 0.517 cc) in the right thyroid bed, suggestive of a remnant. Twenty days later, without stimulation, laboratory tests showed a Tg of 6.0 ng/mL and negative TgAb. This case was discussed at our Multidiscipline Endocrine Conference, with recommendation for rhTSH-stimulated RAI therapy. Approximately three months after the first 131I scan, she returned for the planned RAI therapy under rhTSH stimulation. Laboratory tests showed a TSH of 186.67 μIU/mL, an undetectable Tg and negative TgAb. The 24-hour uptake over the thyroid bed was 2.24%. The second scintigraphy (Fig. 1B) showed resolution of the previous iodine accumulation in the right central neck. The second SPECT/CT (Fig. 1D) showed markedly reduced soft tissue (approximately 0.24 cm×0.16 cm×0.16 cm; calculated tissue volume of 0.006 cc) in the right thyroid bed. The measured urinary iodine concentration was 37 μg/L (normal 26–705 μg/L), indicating no iodine contamination. Because of these unexpected findings, the planned RAI therapy was not performed, and a decision was made to observe this patient. Over the last nine months, she has had three follow-up tests without stimulation; all showed undetectable Tg and negative TgAb levels.
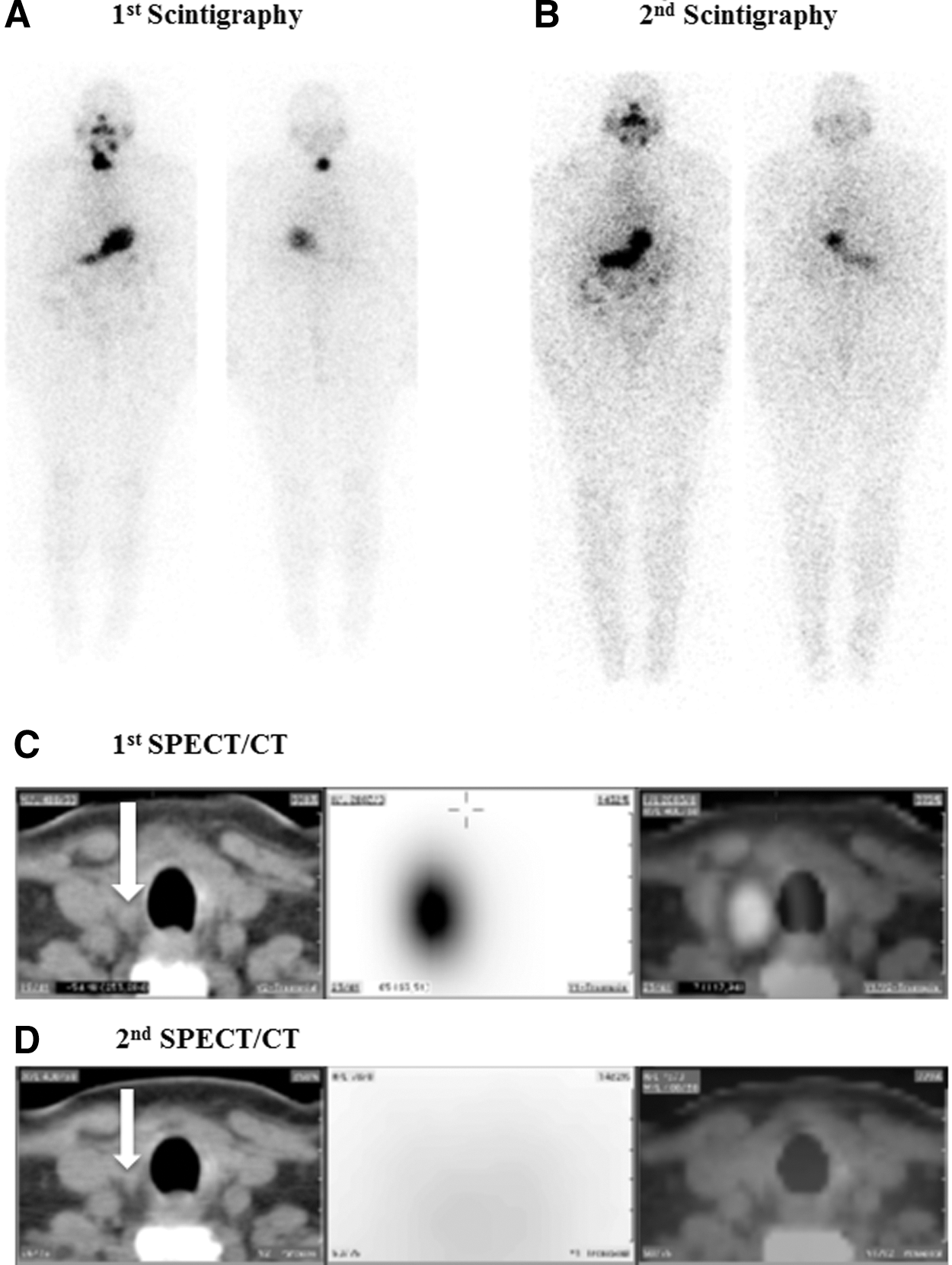
A focus of intense radioiodine uptake in the right central neck of this patient was demonstrated on the first scintigraphy
Despite the unexpected nature, data in this report meet criteria for a successful thyroid remnant ablation following administration of a diagnostic dose of 131I, including absent tracer accumulation on the second Thyrogen-stimulated 131I scintigraphy without evidence of iodine contamination, a decrease of the Tg levels to undetectable with or without stimulation, and a markedly reduced remnant tissue size on the SPECT/CT images. A literature search revealed that the lowest dose of 131I tested for thyroid remnant ablation was 15 mCi (555 MBq) with a 59.6% success rate (2). A systematic review of 18 published clinical studies showed that most of the investigators considered 30 mCi (1110 MBq) of 131I as the lowest effective dose for RAI therapy (3). To our knowledge, this is the first report describing successful thyroid remnant ablation with a diagnostic dose (4.27 mCi; 159 MBq) of 131I. Based on the size measurement on the first SPECT/CT (Fig. 1C), the estimated remnant volume was approximately 0.517 cc. In conjunction with 4.35% of 24-hour 131I uptake, the calculated radioactivity within the remnant is 32,900 rad (329 Gy). This is approximately 10% above the threshold of 30,000 rad (300 Gy) for successful RAI therapy of thyroid remnants proposed by Maxon et al. (4). In retrospect, the transient elevated Tg (6.0 ng/mL) in this patient 20 days after receiving a diagnostic dose of 131I may have resulted from the destruction of remnant cells.
The rationale of RAI therapy for postoperative DTC patients is at least twofold: ablation of thyroid remnants may facilitate the early detection of recurrence or metastasis of thyroid cancer based on serum Tg measurement and/or on follow-up 131I scans; and destruction of potential microscopic metastasis may reduce the rates of recurrence or metastasis. This case demonstrates that successful ablation of thyroid remnant could be achieved with a diagnostic dose of 131I under Thyrogen stimulation. Further clinical studies and a long-term follow-up are needed to define a subgroup of low-risk DTC patients who may benefit from RAI at such a low dose of 131I, while maintaining a low rate of recurrence or metastasis.
Footnotes
Acknowledgments
We are very grateful to the patient for her cooperation in multiple tests and follow-up. We also thank Drs. Michael Kaplan and Paresh Mahajan for their invaluable discussion and suggestions.
Author Disclosure Statement
The authors declare that no competing financial interests exist.