
Abstract
Background:
Prior to undergoing radioiodine therapy (RIT), patients regularly have concerns about isolation on the ward (mandatory for RIT for at least 48 hours in Germany due to radiation protection legislation) as well as fear of the presence of radioactive substances. In this study, these fears were investigated before and after RIT.
Methods:
A questionnaire was developed for completion both before and after radioiodine therapy. Questions included: (i) “Are you afraid of a therapy with radioactive substances?” (ii) “Do you have reservations about contact with radioactive substances?” and (iii) “Are you anxious about isolation?” Possible answers were made in a qualitative representation using a scale of 1–4 (4=full agreement, 3=mostly agreement, 2=partial agreement, and 1=no agreement). Further questions included, for example, sources of information used prior to therapy. A total of 209 patients treated by single or preplanned multiple RIT were surveyed over a period of 8 months (return 109). Analysis was done in subgroups according to age, education, disease, and number of RITs.
Results:
Question 1, “Are you afraid of a therapy with radioactive substances?” showed a similar statistically relevant decline in each subgroup (p<0.05), except for patients with multiple RIT (p=0.81). Asked about the handling of radioactive substances and their perception about the safety in this regard, the entire collective showed a highly statistically significant (p<0.01) decrease with little variability between the groups. The question concerning fear of isolation resulted in a significant decrease (p<0.05) in all subgroups, except for patients with multiple RIT (p=0.13). Analysis of sources of information before RIT showed that older patients preferred printed material and rarely used online resources, while younger patients used the internet more frequently, in addition to printed materials. Finally, most patients would undergo radioiodine therapy again (medical indication provided), with 54% fully agreeing and only 4% not agreeing.
Conclusions:
The survey demonstrates a reduction in concerns about nuclear radiation, use of unsealed radioactive materials, and isolation on the ward after RIT. Surprisingly, concerns rise again before a subsequent therapy.
Introduction
R
Nuclear medicine inpatient units are subject to specific radiation safety procedures and hygiene regulations. In addition to physical provisions, there are restrictions affecting the patient directly, such as the mandatory isolation in the ward (patients may not leave the ward for at least 48 hours) as well as restrictions on water consumption for personal hygiene. These arrangements, in particular the isolation, are often disturbing to patients, so that some even refuse to be treated at all. Over the decades, an increasing number of patient-centered improvements were made to nuclear medicine inpatient units. Wireless internet access, personal TV and the ability to use a bicycle ergometer intended to make the two- to five-day isolation on the ward as comfortable as possible are now the standard in many facilities.
A survey was conducted to evaluate patients' feelings about RIT and the associated circumstances and how this perception changes during the course of therapy. Other questions explored which sources of information the patients used before RIT (e.g., online resources, general practitioner's advice, or nuclear medicine physicians).
In recent years, a significant uncertainty and skepticism towards radioactivity has been noted in patients scheduled for RIT. Fear of radiation is the primary concern (3,4). In certain cases, the fear of radiation exposure even leads to refusal of RIT (5).
The aim of this study was to explore this radiation-related anxiety in a questionnaire, as well as differences—if any—between individual groups, such as patients with single versus multiple RITs or with different educational backgrounds. This is of interest because of the known differences in perception of ionizing radiation between experts and laypersons (6). The design of the questionnaire was based on existing standardized questionnaires used for quality management. In this case, data was collected taking into account fear of radiation as well as the particular situation in a nuclear medicine inpatient unit with its legal requirements (radiation protection and radiation hygiene). Likewise, the general well-being of the individual patient during the stay, side effects, and sources of information were to be recorded in the questionnaire.
Materials and Methods
Two questionnaires were designed (pretherapeutic and posttherapeutic); questions are shown in Table 1. The pretherapeutic questionnaire was handed out one week before admission to the hospital. Patients received the posttherapeutic questionnaire prior to their discharge from the ward. Data collection was anonymous. Answers were given as a quantitative representation with a scale of 1 to 4 (4=full agreement, 3=mostly agreement, 2=partial agreement, and 1=no agreement). Sociodemographic data such as age, gender, nationality, education, the number of previous radioiodine therapies, and the underlying disease (malignant / benign) were surveyed as well. The questionnaires were distributed to a total of 209 patients over a period of 8 months, beginning in April 2011. The evaluated collective of patients consisted of 109 returns [mean age of 57 years; 23 men and 86 women; 66 patients with the first RIT and 43 with more than one RIT (preplanned)]. Forty-seven patients were treated for malignant thyroid disease and 62 for benign thyroid disease. Educational background (years of school education only) was distributed as follows: 40 patients with 9 years, 29 patients with 10 years, and 40 patients with 13 years.
Results shown as percentage of respondents (rounded). Scale for responses: 4, full agreement; 3, mostly agreement; 2 partial agreement; 1 no agreement.
RIT, radioiodine therapy.
Statistical analysis was performed using Wilcoxon matched pairs test with Hodges-Lehmann estimator (significance level p=0.05) to determine changes between pre- and posttherapeutic responses and Fisher-Freeman-Halton exact test to compare different groups.
Results
The quantitative evaluation of all patients surveyed on the question “Are you afraid of a therapy with radioactive substances?” before and after radioiodine therapy is shown in Table 2, showing a similar statistically relevant decline in each subgroup (gender, education, benign or malignant disease, number of RITs; p<0.05), except for patients with multiple RITs (p=0.81).
Median response values; scale: 4, full agreement; 3, mostly agreement; 2, partial agreement; 1, no agreement.
Changes estimated by Hodges-Lehmann estimator (HLE). *Not significant (p>0.05).
Asked about the handling of radioactive substances and their perception of safety in this regard, the entire collective showed a highly statistically significant (p<0.01) decrease of concern with little variability between the groups (Table 2). There was no statistically significant difference between patients with the first RIT or multiple RITs (p=0.93; Fig. 1).
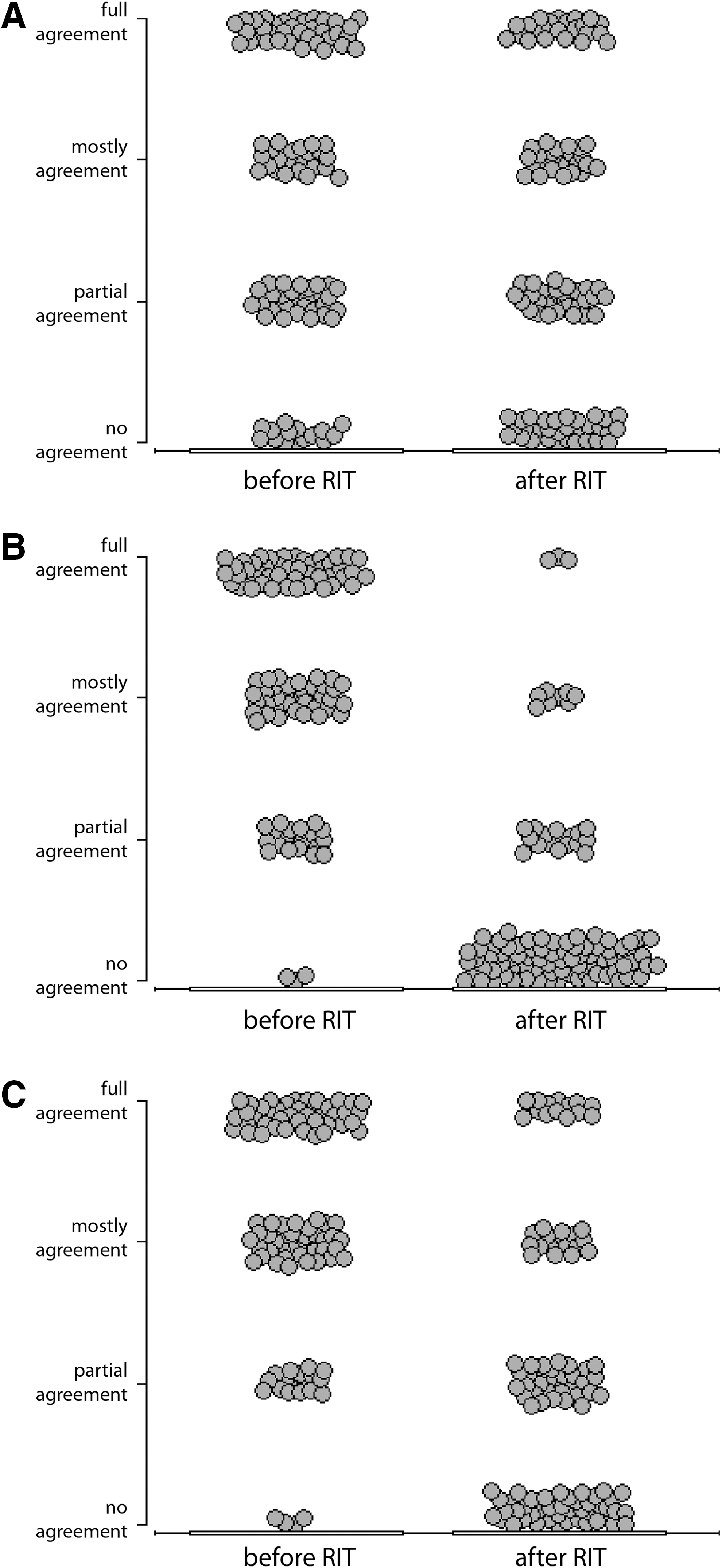
Responses to questions 1–3 before and after radioiodine therapy. (
The question concerning fear of isolation resulted in a significant decrease (p<0.05) in all subgroups (Table 2), except for patients with multiple RIT (p=0.13). Most patients (70%) had no major problems with boredom, possibly due to the availability of television, internet access, and other amenities.
To analyze the sources of information before RIT (Table 1, pretherapeutic questions 6 and 7), patients were split into subgroups by age (over/under 50 years). It was shown that older patients preferred printed material and rarely used online resources. As expected, younger patients used the internet more frequently; however, use of printed materials was also common.
The remaining questions were only asked either pre or post therapy and dealt with information provided before therapy as well as the patients' experiences in the nuclear medicine therapy ward. This included, for example, the survey of the limitations due to radiation protection, the resulting hygiene restrictions such as the limited amount of water in the shower, and the strict smoking ban. Results are shown in Table 1. Smokers did not show significantly higher anxiety related to isolation pre therapy than nonsmokers; posttherapeutically, smokers did not consider the smoking ban worse than other radiation protection measures or the limitations to personal hygiene.
The final questions assessed whether the patients would undergo radioiodine therapy again (medical indication provided), with 54% fully agreeing and only 4% not agreeing. Similar results—58% fully agreeing and only 2% not agreeing—were obtained when asked about recommendation of a radioiodine treatment to others (Table 1).
Discussion
Initial reservations of the population concerning the handling of radioactive materials (7) and therapy with these, which are already described in the literature, show a clear and statistically significant decline after radioiodine therapy. This includes fear of contamination and “the invisible threat” posed by the handling of these substances, as previously described by Freudenberg et al. after qualitative interviews with RIT patients (8). The largest decline was seen in the question about the handling of radioactive substances. An explanation for this large decline might be the diligent handling of the radiation protection measures on the ward, as well as the direct experience that the therapeutic dose is calculated individually for each patient (3,5,6,8 –11). Daily measurements of the residual activity in the thyroid and whole body most likely also reassure the patient.
An interesting comparison can be made to a study by Stegie et al. from the 1970s, which described that the skepticism toward radiation increased with the level of education (12). This was not found in the present results: significant differences were observed only between highest and lowest levels of education, with more educated patients showing less skepticism.
Concerning fear of isolation on the ward, there was an overall decrease of the initial anxiety. Patients with the first radioiodine therapy did not differ significantly (p=0.38) from those with multiple radioiodine therapies, with a similar initial value (Fig. 1). This shows that re-treatment with a resulting second isolation is still perceived as uncomfortable by the patient. It is also interesting that the general fear of radioactivity experienced by patients undergoing a second or multiple therapies is similar to the value experienced by first-time patients. The two groups did not differ significantly (p=0.87) (Fig. 1). On the contrary, patients with multiple RIT showed significantly (p=0.01) higher fear of handling radioactive substances before therapy. This is consistent with the results of Freudenberg et al., whose qualitative interviews conducted two years after radioiodine therapy showed that the described views on radioactivity were nearly identical to the views before radioiodine therapy was performed (8). The present results show that in as little as three months, which is the period between first and second RIT in some patients with malignant thyroid disease, the fear of dealing with radioactive substances increased again. Acceptance of the restrictions due to radiation protection, such as the smoking ban and the limitation of water consumption, was surprisingly good.
As a source of information, the internet was used mostly by younger patients (<50 years). The brochures and information sheets handed out were generally regarded as very important in all age groups. This is in agreement with a study by D'haese et al., who showed that fear of radiation therapy is significantly reduced by handing out information sheets (13). Nevertheless, the individual information provided by the nuclear medicine physician remains essential for the patient, particularly when considering the special circumstances of treatment with radioactivity and a lack of knowledge on the subject in the population.
In summary, patients are generally satisfied and do not feel the restrictions to be overly disturbing. This is particularly emphasized by the result that the majority would agree to undergo RIT again as well as recommend RIT to others.
Footnotes
Author Disclosure Statement
No competing financial interests exist.