
Abstract
Background:
T-cell prolymphocytic leukemia (T-PLL) is rare, accounting for only 0.06% of all malignant lymphomas, and is classified as a T-cell mature lymphoma. The disease affects mainly elderly patients and is characterized by splenomegaly, lymphadenopathy, skin infiltration, and a high leukocyte count, but thyroid filtration has never been detected as far as we could determine. We report here a case of infiltration of the thyroid gland by T-PLL.
Patient findings:
An 89-year-old woman who had been treated for Hashimoto's thyroiditis for 20 years presented with a progressively enlarging thyroid mass accompanied by dyspnea and dysphasia. Atypical lymphocytes with irregular nuclei were observed in the peripheral blood. An open biopsy of the thyroid provided pathological evidence of T-PLL, and bone marrow examination showed infiltration by T-PLL. The diagnosis was therefore infiltration of the thyroid gland by T-PLL. Chemotherapy was initiated, but six months after termination, recurrence of neck swelling was observed. The patient was then treated with radiotherapy, but she died of a major stroke 15 months after onset.
Summary and conclusion:
This is the first report of T-PLL infiltration of the thyroid gland, reminding physicians to keep in mind a broad differential diagnosis when encountering a patient with diffuse thyroid lesions and abnormal lymphocytes in the peripheral blood.
Introduction
M
Primary thyroid T-cell lymphoma is extremely rare and is defined as a lymphomatous process involving the thyroid gland without contiguous spread or distant metastases from other areas of involvement at diagnosis. Only 12 cases of primary thyroid T-cell lymphomas are reported in the literature (2 –12). On the other hand, secondary thyroid infiltration of hematological malignancies was diagnosed in 3–7% of autopsied leukemia cases (13). Furthermore, two cases of acute myeloid leukemia and two of acute lymphocytic leukemia have been identified in living persons based on cytomorphological evidence (14 –16).
T-cell prolymphocytic leukemia (T-PLL) is also rarely observed, accounting for only 0.06% of all malignant lymphomas, and is classified as a T-cell mature lymphoma. The disease affects mainly elderly patients and is characterized by splenomegaly, lymphadenopathy, skin infiltration, and a high leukocyte count, but thyroid filtration has never been detected as far as we could determine.
We present an extremely rare case of infiltration of the thyroid gland by T-PLL. The patient was treated with conventional chemotherapy including cyclophosphamide, doxorubicin, vincristine, and prednisolone (CHOP); cladribin; and mitoxanetrone and with a total dose of 48 Gy irradiation, but died 15 months after diagnosis.
Patient
An 89-year-old woman who had been treated for Hashimoto's thyroiditis for 20 years presented with a 4-day history of a progressively enlarging thyroid mass accompanied by dyspnea and dysphasia. Her history included superventricular extrasystolies and an atrial ventricular block. A cardiac pacemaker to counter the atrial ventricular block had been implanted six years previously. Physical examination revealed diffuse thyroid enlargement with cervical lymphadenopathy (Fig. 1), and laryngeal endoscopy showed extreme swelling of the posterior pharyngeal wall as well as upper airway obstruction. A computed tomography scan showed a diffuse enlargement of the thyroid gland from the base of the skull to the upper mediastinum accompanied by lymphoadenopathy, and a low-density area in the right thyroid gland (Fig. 2). The computed tomography scan also showed multiple instances of mediastinal adenopathy in the chest but no abnormal findings in the abdomen.
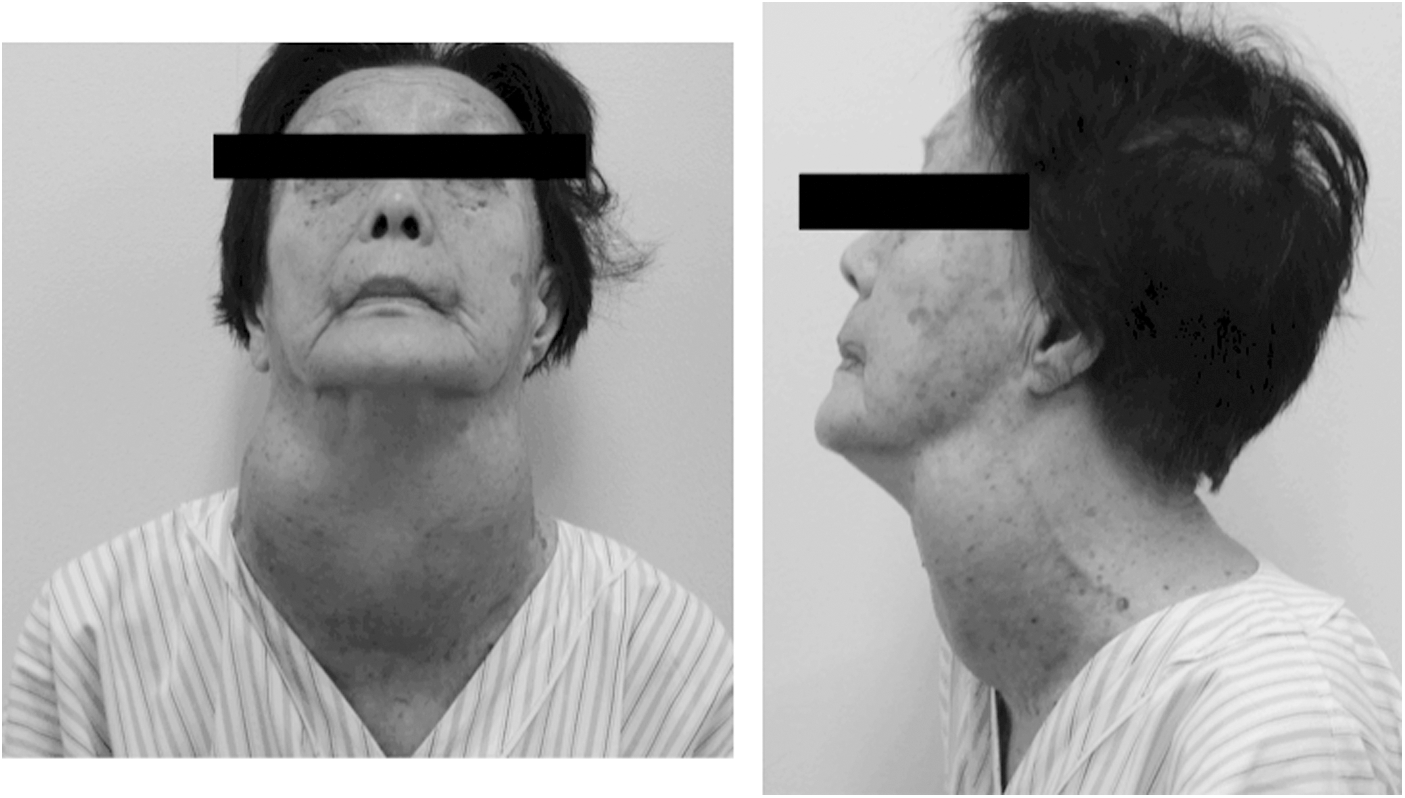
View of the neck at the first visit showing significant neck swelling.

Neck computed tomography scan image demonstrating diffuse enlargement of the thyroid gland from the base of the skull to the upper mediastinum, and a low-density area in the right thyroid gland. Arrows indicate the thyroid gland.
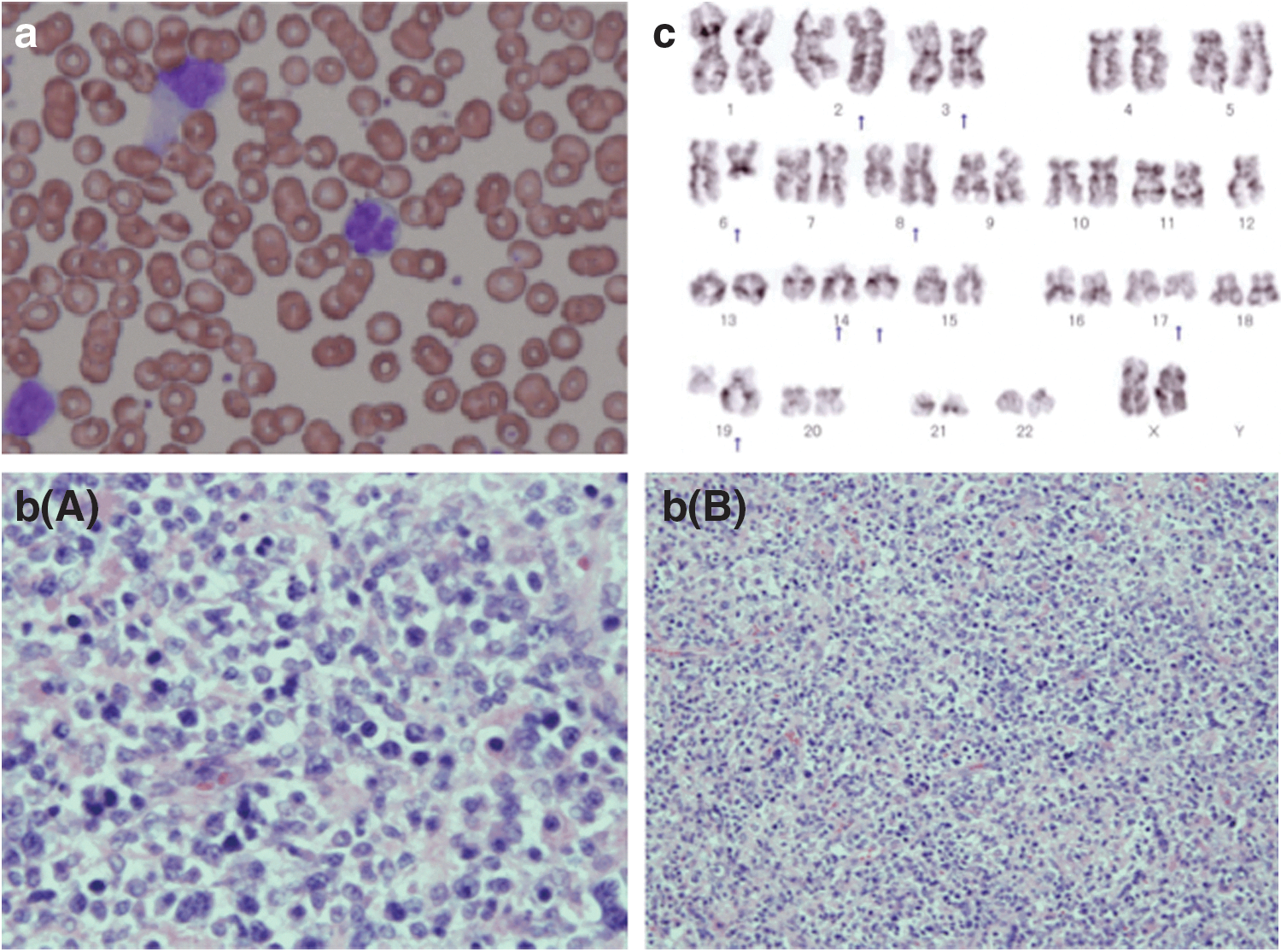
Laboratory data were as follows: white blood cells 24,700/μL (stab 0%, segs 16%, mono 3%, eosinophils 19%, lymphocytes 39%, abnormal lymphocytes 23%), red blood cells 3.57×106/μL, hemoglobin 10.5 g/dL, platelets 308×103/μL, C-reactive protein 0.30 mg/dL, lactate dehydrogenase 265 IU/L, erythrocyte sedimentation rate 86, and soluble interleukin-2 receptor 2840.4 U/mL. Atypical lymphocytes with irregular nuclei were observed in the peripheral blood. The atypical lymphocytes ranged in size from small to medium with a manifest nucleolus and a petal-like nucleus with constrictions. The cytoplasm was basophilic (Fig. 3). Neoplastic cells with mature helper T-cell markers (CD3, CD4, CD5, CD7, CD45RO, TCRαβ), but without B-cell markers (CD19, CD20), were detected by a fluorescence-activated cell sorting analysis of the peripheral blood. The patient presented with hypothyroidism (thyrotropin 11.39 mU/L, free triiodothyronine 2.16 pg/mL, free thyroxine 0.60 ng/dL, and thyroglobulin 31,000 ng/mL, with 0.0% of thyrotropin receptor antibody and 26.7 U/mL of thyroid peroxidase antibody).
Serum test results were negative for human T-lymphotropic virus type-1, while Southern blotting revealed a clonal rearrangement of the T-cell receptor beta-chain gene in peripheral blood mononuclear cells.
An open biopsy of the thyroid gland showed diffuse infiltration of many small or medium-sized atypical lymphocytes (Fig. 3). Immunostaining of the thyroid tissue indicated that the lymphocytes were positive for CD3, CD4, CD5, and CD45RO, and negative for CD7, CD8, CD10, CD20, CD23, and CD79a. Results of a fluorescence-activated cell sorting analysis of a cell suspension from the thyroid tissue were similar to those of the peripheral blood mononuclear cells. Chromosome preparation of the thyroid tissue revealed abnormal karyotypes, 46, XX, add (2)(q21), del (3)(q?), del (6)(q?), add (8)(q24), −12, +add (14)(q24), add (14)(q32), del (17)(q?), and del (19)t(12;19) (q13;q31.1). Flow cytometry showed high levels of CD3, CD4, CD5, and 45RO (Fig. 3). Although deletion of 11q22–23, which would suggest an ATM locus abnormality and presence of inv(14)(q11;q32), was not detected, a complex of chromosomal abnormalities, including addition of 14q32, which can be typical of T-PLL, was found. The patient was pathologically and genetically diagnosed with T-PLL of the thyroid gland based on the World Health Organization classification. Bone marrow examination showed infiltration of malignant T cells, while histological examination and fluorescence-activated cell sorting analysis revealed bone marrow infiltration. These findings were similar to those of the thyroid tissue.
One course of CHOP resulted in temporary reduction of the thyroid mass, but after one week, the thyroid mass started to grow more rapidly than before. Therefore, the patient was treated with 5 cycles of cladribine 2.5 mg/m2 and prednisolone 1 mg/kg on days 1–5. After three cycles, chemotherapy was combined with mitoxanetrone 3 mg/m2 on day 1 for added potency (Fig. 4). Subsequently, the chemotherapy was discontinued because of frequent angina chest pain and vertigo associated with vertebrobasilar insufficiency. The chemotherapy reduced the size of the enlarged thyroid mass and neck lymph nodes, and resulted in disappearance of the atypical lymphocytes. However, six months after the end of chemotherapy, recurrence of neck swelling was observed, so the patient was treated with radiotherapy (48 Gy, 24 fractions), which resulted in a partial response. After 2 months of radiotherapy, however, recurrence was observed, and the patient died of a major stroke 15 months after diagnosis of infiltration of the thyroid gland by T-PLL.

Course of chemotherapy and resultant reductions in white blood cells and atypical lymphocytes. CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisolone.
Discussion
Leukemias derived from mature lymphocytes are known as chronic lymphoid leukemias. These mature, or chronic, lymphoproliferative disorders can be divided into B-cell- and T-cell-derived disorders (17), the former being over four times more common than the latter. T-PLL is an uncommon variant of chronic lymphocytic leukemia and recognized by the new World Health Organization classification as a malignant lymphoma. T-PLL frequently involves skin, spleen, and marrow, but thyroid infiltration and lymph node involvement have not been reported.
Primary thyroid malignant lymphomas account for 1–2.5% of malignant lymphomas, less than 2.5% of non-Hodgkin's lymphomas, and 2–5% of thyroid cancers (2). Histologically, most thyroid malignant lymphomas are mucosa-associated lymphoid tissue lymphomas and diffuse large B-cell lymphomas.
To the best of our knowledge, 12 cases of T-cell-origin thyroid malignant lymphomas have been reported (2 –12), but no instances of thyroid malignant lymphoma associated with T-PLL have been documented.
The patient presented here had a history of rapid thyroid mass enlargement accompanied by hoarseness and dysphagia, a presentation that is similar to the majority of patients with primary thyroid T-cell lymphomas or anaplastic thyroid cancers. The laboratory data of the peripheral blood led us to suspect the presence of a malignant thyroid lymphoma, so we performed a thyroid biopsy, which resulted in the diagnosis of T-PLL. Since bone marrow infiltration was detected at the patient's first visit, our final diagnosis was infiltration of the thyroid gland by T-PLL. However, no skin invasion or splenomegaly, characteristic of T-PLL, was found.
Cladoribine (2-chlorodeoxyadenosine or 2-CdA) is a prodrug and its intracellular phosphorylation is necessary for exerting its cytostatic effect by inhibiting deamination by adenosine deaminase (18). In contrast to other antineoplastic drugs, 2-CdA is cytotoxic to both proliferating and quiescent cells (19,20). Purine nucleotide analogs are highly effective for chronic lymphoid leukemias and low-grade B- and T-cell non-Hodgkin's lymphomas, including Waldenström's macroglobulinemia and hairy cell leukemia. Several reports have confirmed that PLL can be effectively treated with purine nucleotide analogs such as 2-CdA. For our patient, first-line treatment with CHOP was not effective and the thyroid gland swelled more than before the treatment, so we decided to use 2-CdA, which suppressed tumor progression for at least 6 months.
Myelosuppression and infection are reportedly the most common adverse effects of 2-CdA, with neutropenia of grade 3 or more, anemia, thrombocytopenia, and infection observed in 17%, 3%, 5%, and 12%, respectively, of patients treated with 2-CdA. However, none of these patients experienced nausea; vomiting; alopenia; or renal, hepatic, cardiac, pulmonary, or neurological toxicity (21). For this reason, 2-CdA could be administered without adverse effects to our patient despite her advanced age.
Infiltration of the thyroid gland by a T-cell lymphoma is a very rare type of disease, and its prognostic implications have not yet been clarified. T-cell lymphomas are generally associated with a worse prognosis than B-cell lymphomas, and T-PLL is very aggressive and frequently refractory to conventional chemotherapy regimens, resulting in a median survival of between 6½ and 7½ months. However, it has been reported that the median survival of patients treated with 2-CdA is 14 months (22). Since our patient survived 15 months, 2-CdA can be considered to improve prognosis compared with CHOP.
To the best of our knowledge, this is the first report of infiltration of the thyroid gland by T-PLL, reminding physicians to keep in mind a broad differential diagnosis when encountering a patient with diffuse thyroid lesions and abnormal lymphocytes in the peripheral blood.
Footnotes
Author Disclosure Statement
No competing financial interests exist.