
Abstract
Background:
While radioactive iodine (RAI) adjuvant therapy is commonly recommended for most papillary thyroid cancer patients presenting with large volume nodal involvement, it remains unclear if such therapy impacts the disease-specific recurrence rate and overall survival. In this study, we compared the risk of achieving a structural persistent response after low administered activity (100 mCi), intermediate administered activity (150 mCi), and high administered activity (>200 mCi) RAI adjuvant therapy in patients presenting with pathologic N1b disease.
Methods:
This was a retrospective review of 181 papillary thyroid cancer patients with N1b disease treated with total thyroidectomy, neck dissection, and RAI remnant ablation. Dose–response relationships were determined between the administered activity of 131I and the best response to initial therapy.
Results:
Out of the 181 patients, only 39% achieved no clinical evidence of disease (NED) after initial therapy. Young patients (Stage I) had a statistically nonsignificant trend toward higher rates of NED with increasing dose (34% low activity, 36% intermediate activity, 46% high activity), but there was no evidence of dose–response effect with regard to the likelihood of having a structural persistent response to initial therapy or the likelihood of having persistent biochemical evidence of disease. However, analysis of the older patients (Stage IVa) did reveal a trend toward statistically significant dose–response relationships with increasing administered activities being associated with lower rates of structural persistent response (46% low activity, 23% intermediate activity, 17% high dose). Unfortunately, the lower rate of structural persistent response only modestly increased the likelihood that patients would be NED but was instead associated with a higher proportion of patients being classified as having biochemical persistent disease at 12–18 months.
Conclusions:
It appears that administering more than 100 mCi of RAI as adjuvant therapy in N1b disease is unlikely to improve the initial response to therapy. This is especially true for the younger (Stage I) patients. It is plausible that administered activities of 150–260 mCi may be associated with an improved response to initial therapy in older patients (Stage IVa) who are probably at highest risk of having poor outcomes, but the potential benefit from RAI should be balanced against potential adverse effects in those patients.
Introduction
D
Because of the high risk of structural disease recurrence and concern for the possibility of distant metastases, most clinicians continue to recommend radioactive iodine (RAI) ablation/adjuvant therapy for patients presenting with large volume lymph node metastases, even though the data on clinical benefit are conflicting (5). Despite the fact that RAI ablation is usually recommended to these patients, there is little consensus with regard to the optimal administered activity of 131I that can be used to maximize the tumoricidal effect while minimizing side effects. Recommendations for these patients often range from 100 to 250 mCi (3700–9250 MBq) depending on the clinical situation, the treating physician, and patient preference. Even within our center, administered activities have varied widely across our disease management team.
Since many of the side effects of RAI are dose related, it is important to define the minimum administered activity that reliably achieves a therapeutic benefit. Administration of the smallest effective RAI administered activity would limit the potential risks for nausea, vomiting, ageusia (loss of taste), acute and/or chronic salivary gland dysfunction and associated mouth pain and dental caries, lacrimal duct obstruction, pulmonary fibrosis, alterations in gonadal function, and second primary malignancies (lymphoma, leukemia, breast, bladder, colon, salivary glands) (6 –8). Since the incidence of many of these side effects are higher with 250 mCi (9250 MBq) than with 100 mCi (3700 MBq) administered activities, it is critically important to determine if higher administered activities are required for optimal clinical outcomes.
Therefore, the goal of this retrospective study was to determine if the administered activity of 131I selected by the clinician had a significant impact on the clinical outcomes in papillary thyroid cancer patients presenting with clinical N1b disease. We hypothesized that the response to initial therapy would not be dose dependent over the relatively narrow range of administered activities typically recommended at our center (100–250 mCi, 3700–9250 MBq). The primary endpoint was the presence of persistent/recurrent structural disease as the best response to initial therapy in clinical N1b patients who received low activity (approximately 100 mCi), intermediate activity (approximately 150 mCi, 5550 MBq), or high activity adjuvant therapy (approximately 200 mCi, 7400 MBq).
Materials and Methods
Subjects
After obtaining Institutional Review Board approval, we reviewed the electronic medical records of 394 subjects with papillary thyroid carcinoma with lymph node involvement that were treated at the Memorial Sloan–Kettering Cancer Center between 1995 and 2012. Subjects were included if they met all of the following conditions : (i) papillary thyroid carcinoma (we excluded patients with follicular, Hürthle cell, poorly differentiated, medullary, or anaplastic thyroid carcinoma); (ii) total thyroidectomy and neck dissection with complete disease resection prior to RAI ablation; (iii) pathologically confirmed N1b disease; (iv) lack of gross extrathyroidal extension at initial surgery; (v) lack of evidence for distant metastatic thyroid cancer before and/or after ablation; (vi) on thyrotropin (TSH)-suppressive therapy for the duration of the study; (vii) one year or more of follow-up after RAI ablation, unless one of the clinical endpoints (recurrence, thyroid cancer-related death) was reached earlier; and (viii) appropriate follow-up with unstimulated thyroglobulin (Tg) and thyroglobulin antibodies (TgAb) and imaging (neck ultrasounds, computed tomography [CT]/magnetic resonance imaging [MRI], fluorodeoxyglucose positron emission tomography [FDG-PET] when available). We excluded patients with detectable TgAb. Seven patients with elevated neck uptake at the time of the ablation (≥6%) were excluded. In addition, six patients were excluded because they received RAI-administered activities of <100 mCi, and the 24-hour neck uptake was unknown. Only 12 patients did not receive RAI after complete resection of T1–3N1bM0 PTC and were excluded from the analysis. Thus, a total of 181 patients were selected for the study.
Histopathologic analysis
Tumors were classified according to the last World Health Organization criteria with the exception of tall cell variant (TCV-PTC) (9). Tumors were classified as TCV-PTC if they contained ≥50% tall cells. The latter cell type was defined as having a height at least twice its width with an oncocytic cytoplasm (10).
RAI adjuvant therapy
The decision to treat with RAI, the choice of the preparation method (recombinant human TSH [rhTSH] vs. thyroid hormone withdrawal [THW]) and the choice of RAI-administered activity were all at the discretion of the treating physician. All patients were asked to adhere to a low iodine diet for five to seven days prior to the planned RAI treatment.
Patient follow-up
Patients were followed every six months during the first year and then at 6–12 month intervals thereafter at the discretion of the treating physician. The frequency of follow-up visits was based on the estimated risk of recurrence for each individual patient and the clinical course of the disease.
Clinical endpoint
Each patient was risk stratified according to the seventh edition of the American Joint Committee in Cancer TNM (AJCC/TNM) staging system (Stage I, II, III, or IV) and the American Thyroid Association (ATA) risk of recurrence stratification system (low, intermediate, or high; Table 1) (11,12). Best clinical response to initial therapy was assessed based on clinical data obtained in the year of follow-up using a restratification model proposed and validated by our group. Specifically, patients were classified as having: (i) no clinical evidence of disease (NED) if they achieved an unstimulated Tg level <0.6 ng/dL and had a normal neck ultrasound and/or cross-sectional imaging (CT, MRI); (ii) indeterminate response if they achieved an unstimulated Tg level <0.6 ng/dL (undetectable) and had nonspecific findings by neck ultrasound and/or cross-sectional imaging; (iii) biochemical persistent disease if they had a detectable unstimulated Tg level and no findings or nonspecific findings on neck ultrasound or cross-sectional imaging; or (iv) structural persistent disease if they had suspicious findings by neck ultrasound or cross-sectional imaging or had abnormal uptake on follow-up diagnostic whole body scan when available (not thyroid bed uptake) with any unstimulated Tg level.
PTC, papillary thyroid cancer; RAI, radioactive iodine; Tg, thyroglobulin; US, ultrasound.
A subset of the 181 patients (105 patients) had their stimulated Tg level measured 12–18 months after RAI ablation. Best clinical response 12–18 months after RAI adjuvant therapy was classified as: (1) excellent response if they achieved an stimulated Tg level <1 ng/dL and had a normal neck ultrasound and/or cross-sectional imaging (CT, MRI); (ii) indeterminate response if they achieved an unstimulated Tg level between 1 and 10 ng/dL and had nonspecific findings by neck ultrasound and/or cross-sectional imaging; (iii) biochemical incomplete if they had a stimulated Tg level >10 ng/dL and no findings or nonspecific findings on neck ultrasound or cross-sectional imaging; or (iv) structural incomplete response if they had suspicious findings by neck ultrasound or cross-sectional imaging or had abnormal uptake on follow-up diagnostic whole body scan when available (not thyroid bed uptake) with any stimulated Tg level.
The final clinical status at the time of last follow-up evaluation was recorded for each patient (no clinical evidence of disease, persistent disease, disease recurrence, indeterminate status). The Tg cutoffs used to assess the final clinical status were similar those used for initial response to therapy.
Laboratory studies
Between 1990 and 1997, various Tg assays were used with functional sensitivities of approximately 1 ng/mL. Starting in 1998, all Tg values were measured using the Dynotest-TgS immunoradiometric assay (Brahms, Inc., Berlin, Germany; functional sensitivity 0.6 ng/mL normalized to Certified Reference Material 457) (13). TgAb were measured using Siemens Immulite 2500 Chemistry Analyzer (Siemens Healthcare Diagnostics, Inc., Deerfield, IL). Patients with detectable TgAb were excluded.
Statistical methods
Continuous data are presented as means and standard deviations or median and ranges, as appropriate for each variable. Categorical comparisons were performed with the chi-square test, and continuous variables were compared using either Student's t-test or one way analysis of variance (ANOVA), as appropriate. Correlation analyses were performed using Pearson's linear correlation test. Analyses were performed using SPSS software v18.0.1 (SPSS, Inc., Chicago, IL). A p-value of ≤0.05 was considered statistically significant. The primary endpoint was the presence of persistent/recurrent structural disease as the best response to initial therapy in clinical N1b patients that received low activity adjuvant therapy (∼100 mCi, 3700 MBq), intermediate activity adjuvant therapy (∼150 mCi, 5550 MBq), or high activity adjuvant therapy (∼200 mCi, 7400 MBq).
In order to determine if there was a dose–response effect across the range of administered activities usually recommended for N1b disease at our center, we divided the patients into three groups based on the median administered activity of RAI with initial RAI therapy. The low activity adjuvant therapy cohort received a median dose of ∼100 mCi (n=45, median administered activity of 102 mCi [3774 MBq], range 75–139 mCi [2775–5143 MBq]), the intermediate activity adjuvant therapy cohort received a median of 150 mCi (n=102, median 150 mCi [5550 MBq], range 140–169 mCi [5180–6253 MBq]), and the high activity adjuvant therapy cohort received a median of ∼200 mCi (7400 MBq) (n=31, median 202 mCi [7474 MBq], range 170–468 mCi [6290–17,316 MBq]).
We analyzed the correlation between individual RAI-administered activities as a continuous variable and the best response to initial therapy outcomes using Spearman's rank correlation coefficient and the Jonckheere–Terpstra test.
Finally, we compared the likelihood of achieving structural persistent disease after RAI adjuvant therapy as opposed to NED if patients received: (i) low versus intermediate activity, (ii) intermediate versus high activity, and (iii) low versus high administered activity. The analysis was run for the whole cohort (n=181 patients), and then repeated for patients with stimulated Tg levels (n=105, data not shown). We then stratified the patients by TNM stage, vascular invasion, method of ablation, and sex, and repeated the analysis.
Results
Patient characteristics
The clinicopathological characteristics of the 181 patients included in this study are summarized in Table 2. We only included patients with papillary thyroid cancer with pathologic N1b disease without clinical evidence of distant metastasis at the time of thyroid cancer diagnosis. Most were young (median age 40 years, 61% TNM Stage I) women (62%) presenting with small primary tumors (median 1.7 cm; range 0–9 cm) with minimal extrathyroidal extension (ETE) (65% T3). Seventy-three percent of the primary tumors were classic variant, 14% were tall cell variant, and 7% were follicular variant PTCs. The median number of lateral neck nodes affected was five (range 1–32), and the median size was 2 cm (range 0.2–6.2 cm). If assessed, extranodal extension (ENE) was present in almost half of the affected nodes (45%). Consistent with the AJCC/TNM staging system, all patients were classified as being either Stage I (<45 years old at diagnosis with N1b disease) or Stage IVa (>45 years old at diagnosis with N1b disease).
SD, standard deviation; NED, no clinical evidence of disease.
All patients included in this study received RAI adjuvant therapy (Table 2). The choice of the administered RAI activities was left to the discretion of the treating physician. The median administered activity was 150 mCi (5550 MBq) with patients receiving activities as low as 75 mCi (2775 MBq) or as high as 468 mCi (17,316 MBq). The median 24 hour percent neck uptake was 0.5%. Patients were followed for a median of 3.6 years after RAI adjuvant therapy (range 0.5–18 years).
Clinical outcomes after RAI adjuvant therapy
As expected in patients with clinical N1b disease, only 39% had no clinical evidence of disease after initial therapy, while 15% had a biochemical persistent response, 30% had a structural persistent response, and 16% had an indeterminate response. In the 105 patients with measured stimulated Tg levels 6–18 months after RAI, 23% had an excellent response, 17% had a biochemical incomplete response, 33% had structural incomplete response, and 27% had an indeterminate response. At the time of final follow-up (following either continued observation or additional therapies), 42% were NED, 32% had persistent disease (biochemical and/or structural), 1% had recurrent disease, and 25% had indeterminate disease status (Table 2).
Comparison of clinicopathologic characteristics between dose cohorts
As shown in Table 3, patients receiving low activity adjuvant therapy were more likely to have a higher 24 hour percent uptake (p=0.046) and had longer follow-up (p=0.005) than those who received intermediate activities. Patients who received high activity adjuvant therapy were more likely to be males (p=0.016), less likely to be prepared with rhTSH (p=0.001), and had longer follow-up (p<0.001) compared with those who received intermediate activities. When comparing patients who received low activity to those who received high activity RAI adjuvant therapy, those with higher activities were more likely to be older (p=0.012), male (p=0.018), with microscopic vascular invasion (p=0.014; Table 3). No statistical differences across the activity cohorts were seen with respect to histology (classic PTC vs. nonclassic PTC), the presence of ETE, the number of involved N1b nodes, the size of the involved N1b nodes, or presence of ENE on the diagnostic whole body scan prior to adjuvant therapy.
Data are presented as n (%) or mean±SD. Activity levels: low, median 102 mCi (75–139 mCi); intermediate, median 150 mCi (140–169 mCi); high, median 202 mCi (170–468 mCi).
c-PTC, classical PTC; TCV-PTC, tall cell variant of PTC; FV-PTC, follicular variant of PTC; ETE, extrathyroidal extension; ENE, extranodal extension; rhTSH, recombinant human thyrotropin; THW, thyroid hormone withdrawal.
Best response to initial therapy based on dose cohort
When analyzed across the full cohort, a nonstatistically significant trend toward a higher rate of NED (36% low activity, 39% intermediate activity, and 45% high activity) and a lower rate of structural persistent responses (31% low activity, 32% intermediate activity, and 23% high activity) was noted with escalating RAI-administered activities. When analyzed as a continuous variable, no statistically significant correlation was found between clinical response and RAI-administered activities (Spearman coefficient −0.03, n=181 patients). Using the Jonckheere–Terpstra test, the p-value for testing if continuous RAI-administered activity is associated with clinical outcome is 0.71 (Fig. 1, Table 4).
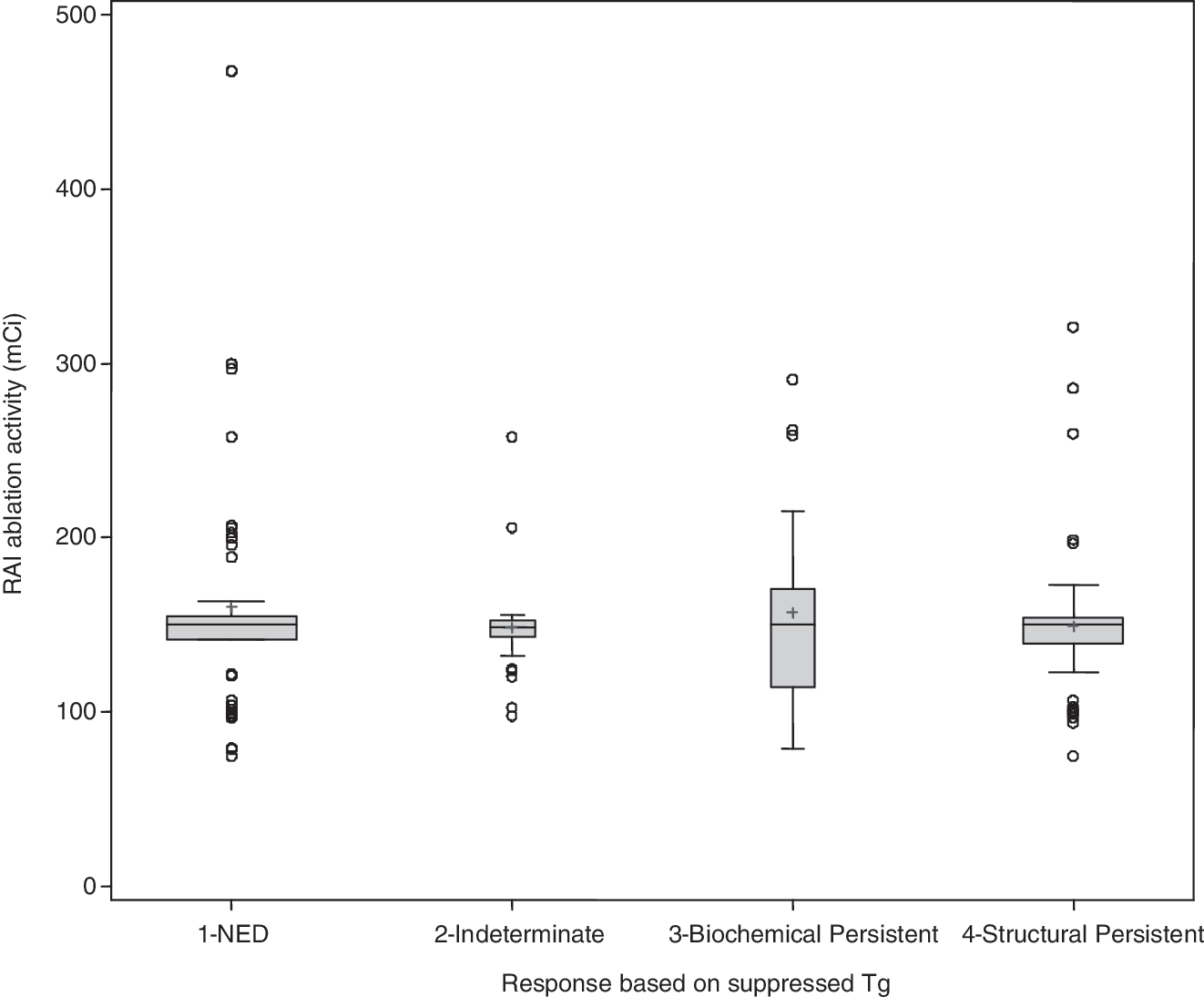
Continuous radioactive iodine (RAI)–administered activities in the four clinical response groups. Between groups, comparisons were made using Spearman's rank correlation coefficient. No correlation was found between RAI-administered activity as a continuous variable and response (Spearman's coefficient −0.03, p=0.71, n=181 patients).
IQR, interquartile range.
Because metastatic disease in young patients tends to be more RAI avid (14), we next analyzed the dose–response relationships with all groups of RAI-administered activities separately in younger patients (AJCC Stage I, younger than 45 years of age at diagnosis) and older patients (AJCC Stage IVa, older than 45 years of age at diagnosis). Similar to the full cohort, young patients had no evidence of dose–response effect with regard to the likelihood of having a structural persistent response to initial therapy (25% low activity [median 102 mCi, range 75–132 mCi], 38% intermediate activity [median 150 mCi (5550 MBq), range 142–164 mCi (5254–6068 MBq)], 31% high activity [median 200 mCi (7400 MBq), range 171–300 mCi (6327–11,100 MBq)]; Fig. 2). It appeared that low activity adjuvant therapy achieved very similar clinical outcomes to intermediate or high activity adjuvant therapy.

The chance of achieving a structural persistent response with escalating RAI-administered activities in the younger (Stage I; low activity: median 102 mCi, range 75–132 mCi; intermediate activity: median 150 mCi, range 142–164 mCi; high activity: median 200 mCi, range 171–300 mCi) vs. older patients (Stage IV; low activity: median 102 mCi, range 94–139 mCi; intermediate activity: median 150 mCi, range 142–163 mCi; high activity: median 260 mCi, range 198–468 mCi).
However, chi-square analysis of the difference of treatment responses amongst all RAI-administered groups in the older patients (Stage IVa) did reveal a significant trend in dose–response relationships with increasing administered activities (p<0.03, compared to p=0.42 for young [Stage I] and p=0.17 for entire cohort). Specifically, we noted lower rates of structural persistent response with increasing RAI-administered activities in the older patients (46% low activity [median 102 mCi (3774 MBq), range 94–139 mCi (3478–5143 MBq)]), 23% intermediate activity [median 150 mCi (3770 MBq), range 142–163 mCi (5254–6031 MBq)]), 17% high activity [median 260 mCi (9620 MBq), range 198–468 mCi (7326–17316 MBq)]; Fig. 2). Unfortunately, the lower rate of structural persistent response only modestly increased the likelihood that patients would be NED but was instead associated with a higher proportion of patients being classified as having biochemical persistent disease (0% low dose, 8% intermediate dose, 33% high dose). Therefore, it appears that higher adjuvant therapy activities administered in Stage IVa patients have only a modest effect on the likelihood of achieving NED at initial therapy, but rather moves the type of persistent disease from structural persistent disease to biochemical evidence of disease without structural correlate. Interestingly, except for being older at diagnosis and being male, the clinicopathological features of Stage I and Stage IV patients were remarkably similar (Table 5). No differences were detected between these two groups with regard to histology, presence of ETE, presence of vascular invasion, size or number of involved lymph nodes, the presence of ENE, the method of preparation, percent uptake in the neck on diagnostic RAI scan, or follow-up time. While the mean RAI-administered activities were statistically different in younger patients compared to older patients, the overall median RAI-administered activities at ablation were similar. Furthermore, no dose–response relationships were evident when analyzed based on sex, histology, presence of ETE, or vascular invasion (data not shown).
Discussion
In the current study, a third of the papillary thyroid cancer patients presenting with pathological N1b disease had a structural incomplete response 12–18 months after total thyroidectomy and RAI adjuvant therapy. These results are compatible with prior studies demonstrating worse outcomes in these patients compared to those of intrathyroidal papillary thyroid cancer or nodal disease limited to the central compartments (N1a) (2,3,5). More importantly, the risk for persistent/recurrent thyroid cancer 12–18 months after initial therapy was not altered by varying RAI-administered activities in the study population.
The optimal RAI activity needed to achieve the best objective RAI response and to minimize RAI-specific adverse effects is not known. Historically, most physicians treat thyroid cancer patients presenting with lateral nodal metastasis with 150 mCi (5550 MBq) of RAI (15). The choice of the RAI adjuvant activity is highly variable among physicians in a common medical center and between various institutions. In our center, that activity ranged between 75 mCi (2775 MBq) and 468 mCi (17,316 MBq), with most such patients receiving close to 150 mCi after surgical resection. Interestingly, the choice of the RAI activity was not greatly influenced by the patients' clinical characteristics. Other than older age at diagnosis, we could not find a clear reasoning as to why some patients received a lower RAI activity and others a higher one. While we were more likely to give escalating RAI activities to patients with increased overall number of involved nodes (N1a+N1b), neither the number nor the size of prognosis-altering N1b nodes affected the choice of the activity. The study enrollment was restricted to papillary thyroid cancer patients presenting with N1b disease, thus limiting the effects of histology-driven variation in RAI avidity on clinical response after RAI.
In our cohort, we could not demonstrate a decreased risk of achieving a structural persistent response when RAI adjuvant therapies exceeding 100 mCi (3700 MBq) were used. This was especially true for the Stage I patients. Young patients with lateral lymph node metastasis have an intermediate risk for recurrence but are at low risk for disease-specific mortality. These younger patients faired equally well/badly with higher RAI-administered activities (≥150 mCi) compared to lower RAI activities (median 102 mCi, 3774 MBq), suggesting a lack of dose response to RAI. It is possible that RAI does not alter disease-specific outcome in these Stage I patients. We did not have a control group of similar patients who did not receive RAI to confirm that hypothesis.
On the other hand, older patients presenting with lateral neck disease at time of thyroid cancer diagnosis are classified as Stage IVa by TNM classification. They are both at an increased risk for thyroid cancer recurrence and disease-specific mortality. In this study, older papillary thyroid cancer patients with nodal metastasis had a trend for a better response with escalating RAI administered activities. Specifically, the risk for achieving a structurally persistent response significantly decreased from 46% with a median 102 mCi (3774 MBq) RAI activity to 23% with a median 150 mCi (5550 MBq) dose and 17% with a median 260 mCi (9620 MBq) activity (p<0.03). As would be expected, this was associated with an increased preponderance for biochemical persistent response but a similar chance for cure one year after RAI therapy. If followed longitudinally, some of the patients in the biochemical persistent response group at one year are expected to revert to an excellent response, as Tg levels are expected to decrease spontaneously to undetectable.
It is possible that the older patients had better dose–response trends than the younger patients because the older patients received larger RAI-administered activity than the younger patients (high activity group median 202 mCi [7474 MBq] in the young and 260 mCi [9620 MBq] in older patients). The varying responses between younger and older patients may be due to unperceived selection bias inherent of retrospective designed studies. Also, while the trend for better response with escalating RAI-administered activity was statistically significant in older patients when all groups of RAI responses were compared to all groups of RAI-administered activities, the association between any two groups of RAI responses and any two combinations of RAI-administered activity was not significant [e.g., NED vs. structural persistent response against (i) low vs. intermediate activity (p=0.259), (ii) intermediate vs. high activity (p=0.663), and (iii) low vs. high activity (p=0.193)]. This may be attributed to the small number of patients studied in each subgroup and lack of power to detect a significant dose–response association. Future, well-designed, randomized clinical trials are needed to determine better the role of RAI therapy in these patients.
We recognize that RAI-administered activity is a poor surrogate marker for lesional RAI absorbed activity, which is the true determinant of therapy success. Lesional RAI absorbed activity is influenced by patient factors such as kidney function, blood volume, height, and weight in addition to tumoral NIS expression. In the absence of lesional dosimetry, correlating clinical response to RAI therapy with blood radiation activity would have been more convincing than correlating clinical response with 131I-administered activity (16). However, in our database, the number of patients with dosimetry (n=13) was too small to make any meaningful conclusions as to the relationship between blood RAI activity and clinical outcome after RAI. These markers should be used in future randomized trials studies to correlate clinical response with minimal effective RAI-administered activity.
In the absence of clear evidence for benefit from higher activities of RAI therapy, we advocate restricting RAI-administered activities in young papillary thyroid cancer patients with pathologically confirmed large volume lateral lymph node involvement to 100 mCi (3700 MBq). It is possible that older patients with large-volume N1b disease may benefit from higher RAI-administered activity (possibly activities >260 mCi [9620 MBq]). However, caution should be exercised with the use RAI activities >150 mCi (5550 MBq) without dosimetry calculation in older patients, especially those with chronic renal insufficiency, as the risk for bone marrow toxicity increases (17).
Multikinase inhibitor therapies have been recently used to augment RAI avidity and objective response to RAI in metastatic thyroid cancer (18). However, they have not been previously used in conjunction with RAI for the adjuvant therapy of patients presenting with lateral nodal involvement. It is very plausible that short-term pretreatment with kinase inhibitor therapies may augment RAI avidity in remnant tissues after surgery and thus enhance RAI efficacy of low to intermediate RAI activities (100–150 mCi, 3700–5550 MBq). This is expected to improve clinical response after RAI in the older PTC patients with nodal metastasis while limiting the potential RAI-specific adverse effects encountered with higher RAI-administered activities. This will be the subject of future prospective randomized trials.
In conclusion, it appears that administering more than 100 mCi (3700 MBq) of RAI as adjuvant therapy in N1b disease is unlikely to improve the initial response to therapy in younger papillary thyroid cancer patients (Stage I) presenting with lateral node involvement. In older patients (Stage IVa), it is plausible that administered activities of 150–260 mCi (5550–9620 MBq) may result in less persistent structural disease and higher rates of persistent Tg in the absence of structurally identifiable disease without a significant improvement in NED. Therefore, the potential benefit from higher RAI activities should be balanced against potential adverse effects in that subgroup of patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist for M.M.S., R.K.G., or R.A.G. R.M.T. is a consultant for Genzyme.