
Abstract
Background:
A higher body mass index (BMI) is associated with more advanced stages of thyroid cancer. Screening obese patients for thyroid cancer has been proposed but has yet to be examined for cost-effectiveness. The objective of this study was to assess the cost-effectiveness of ultrasound (US) screening of obese patients for thyroid cancer.
Methods:
A decision-tree model compared cost savings for the following: (i) base case scenario of an obese patient with thyroid nodule found by palpation, (ii) universal US screening of all obese patients, and (iii) risk-based US screening in obese patients. Risk-based screening consisted of patients who had at least one of four major identified risk factors for thyroid cancer (family history of thyroid cancer, radiation exposure, Hashimoto's thyroiditis, and/or elevated thyrotropin). Patients with nodules underwent established treatment and management guidelines. The model accounted for recurrence, complications, and long-term treatment/follow-up for five years. Outcome probabilities were identified from a literature review. Costs were estimated using a third-party payer perspective. Sensitivity analyses were performed to examine the impact of risk factor prevalence and US cost on the model.
Results:
The resulted costs per patient were $210.73 in the base case scenario, $434.10 in the universal US screening arm, and $166.72 in the risk-based screening arm. Risk-based screening remained cost-effective until more than 14% of obese patients had risk factors and with a wide variation of US costs ($0–$1113).
Conclusion:
Risk-based US screening in selected obese patients with risk factors for thyroid cancer is cost-effective. Recommendations for screening this subgroup will result in cost savings and a likely decreased morbidity and mortality in this subpopulation with more aggressive disease.
Introduction
T
Our group has recently shown that a higher body mass index (BMI) is also associated with a more advanced stage and more aggressive forms of papillary thyroid cancer (8). Importantly, advanced stage and aggressive forms of thyroid cancer are strongly correlated with higher morbidity (recurrence, surgical complications, etc.) and mortality. Evidence has also indicated that if thyroid cancer is detected at an early stage and given appropriate initial treatment, its long-term impact includes lower recurrence and mortality rates (9 –11).
Rising healthcare costs have resulted in an increasing interest in cost-effective methods to prevent and manage surgical and nonsurgical disease. Studies on the cost and health benefits of screening have primarily focused on commonly screened cancers, such as mammography for breast cancer (12,13). However, thyroid cancer is also a cancer recommended for early detection by the American Cancer Society (12). Screening, treatment, and long-term follow-up of thyroid cancer extends for many years and can impact quality of life, particularly in those with more aggressive and advanced disease (14,15).
One possible explanation for advanced thyroid cancers in patients with a higher BMI is delayed diagnosis due to difficulty palpating an obese neck. Thus, we speculate that obese patients may benefit from screening for early detection of thyroid nodules. Ultrasound (US) is the initial diagnostic imaging modality for thyroid nodules and has a relatively high sensitivity (84–89%) and specificity (83–96%) (16 –18). US has been used recently with good success to screen obese patients for thyroid cancer (7). Here, we examine the cost-effectiveness of US screening for thyroid cancer in obese patients, a particularly challenging population.
Materials and Methods
Reference case definition
The reference case is a 46-year-old obese patient with unknown thyroid pathology whose thyroid nodule would be detected by palpation. The age of 46 was chosen so that the American Joint Committee on Cancer Staging (AJCC) criteria on staging would be applicable and that all four stages would be relevant (19). The patient is otherwise healthy with no previous history of neck operations. Obesity in this study is defined as a BMI >30 kg/m2, which is the definition of obesity by the National Heart, Lung, and Blood Institute (20). It is a conservative definition, as there have been studies that have shown an increased risk of thyroid cancer in BMIs as low as 25 kg/m2 (21).
Decision model
A cost–utility analysis was conducted using a decision-tree model with TreeAge statistical software (22). The first pathway follows the reference case obese patient who is sent for US if a nodule is palpated in the neck. This situation is the current method of evaluation of most obese patients. Two additional alternative management pathways were created: (i) any obese patient screened with US; and (ii) an obese patient screened with US who also had at least one known risk factor for thyroid cancer (including family history of thyroid cancer, history of significant radiation exposure, Hashimoto's thyroiditis, and/or elevated thyrotropin (TSH); Fig. 1) (23 –30). The model had a cycle length of five years (enough time for follow-up and/or recurrence of thyroid cancer) and included postoperative surveillance, treatment, and mortality.
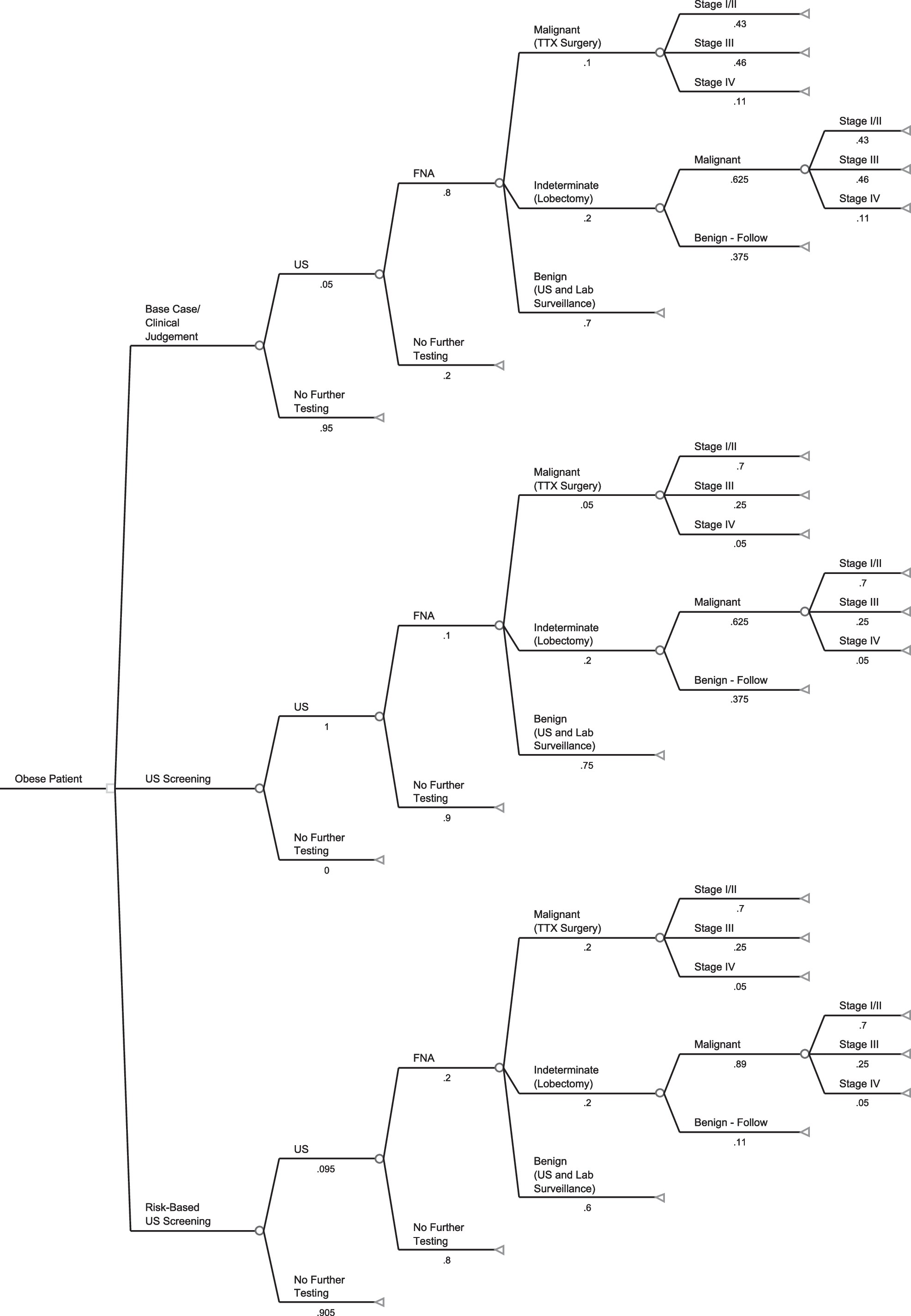
Decision-tree model for thyroid cancer management of obese patients.
Basic structure
The model's event pathways followed current practice opinions of the American Thyroid Association and that of expert clinical judgment on the management of thyroid cancer. Pathway and outcome probabilities were based on an extensive literature review (Table 1). When no literature existed for a specific probability in the decision model, expert opinion was used.
US, ultrasound; FNAB, fine-needle aspiration biopsy; EO, expert opinion used; AVG, average of range of values used; RAI, radioiodine; RLN, recurrent laryngeal nerve.
Risk factors
Four major risk factors for thyroid cancer were identified, and a literature search was conducted to examine their relative risk of malignancy. An average relative risk (RR) for each risk factor was calculated from a range seen in the literature: family history of thyroid cancer (RR 5.0; range 4.1–10), radiation exposure (RR 6.5; range 1.69–11,), Hashimoto's thyroiditis (RR 2.5, range 1.6–2.96), and elevated TSH (RR 5.7, range 1–11.2) (20 –27). This resulted in an average RR of 5.0 for all four risk factors, which was used in determining subsequent pathway probabilities, affecting the outcome probabilities within the third arm (Table 2). Based on a literature search, we used a value of 9.5% for the probability of an obese patient to present with risk factors, which was the value for the most common risk factor seen in the population (Table 2) (31 –33).
TSH, thyrotropin.
Probabilities
Importantly, base case probabilities (top arm, Fig. 1) for stage I/II, III, and IV distribution were calculated using the odds ratio of 2.57 for the increased odds of an obese patient presenting with stage III or IV disease, based on a previous study performed by our group (8). Probabilities of more aggressive and advanced disease were thus presumed for the base case based on a previous literature review of the increased risk of thyroid cancer aggressivity within obese patients. This is why these percentages look skewed and much higher than what is normally expected. The all-US screening and risk-based US screening branches assumed distribution of disease stage of the general population using the National Cancer Institute's Surveillance, Epidemiology and End Results database (1).
The probability of receiving an US in the base case was 5%, based on the relative rate of palpable thyroid nodules in our base case population. We estimated that 80% would then progress to fine needle aspiration biopsy (FNAB) (34,35). In the US screening group, 100% received US screening, and a conservative estimate of 10% were assumed to progress to FNAB. Expert opinion was used to calculate this probability based on the relative prevalence of thyroid nodules in a 46-year-old female (30%) (34) combined with the high sensitivity of US for microcarcinomas and incidentalomas. In the risk-based screening group (third arm), based on prevalence data, as noted above, 9.5% of obese patients were estimated to have at least one risk factor for thyroid cancer and would progress to US screening. Based on the relative risk of 5.0 for having a malignant thyroid nodule, a calculated 20% were assumed to progress to FNAB (Table 1).
The probabilites of FNAB and lobectomy results were determined from Reports from the National Cancer Institute Thyroid Fine-Needle Aspiration State of the Science Conference and the American Thyroid Association (Table 1). The base case probability of FNAB results were 10% malignant, 20% indeterminate, and 70% benign (36,37). Overdetection of thyroid nodules with US screening was anticipated, and an adjusted decreased malignancy rate was used for the US screening group to 5% malignant, 20% indeterminate, and 75% benign. The relative risk of 5.0 for any one of the risk factors was used to determine the probability of FNAB results in the risk-based screening group, resulting in 20% malignant, 20% indeterminate, and 60% benign.
In our model, all indeterminate FNAB results include follicular neoplasm of undetermined significance, atypia of undetermined significance, follicular neoplasm, and suspicious for papillary thyroid cancer. These indeterminate FNAB results underwent lobectomy for definitive diagnosis. We did not choose total thyroidectomy for “suspicious for malignancy” FNAB results or for indeterminate thyroid nodules that have a history of radiotherapy or a family history of thyroid cancer, although we recognize that many patients are offered this as treatment for various individualized reasons. Since it is not standardized, we chose to use lobectomy as a formal, more conservative diagnostic surgical option followed by completion thyroidectomy if the nodule was determined malignant.
We did not include any molecular testing in this model. All patients with malignant FNAB results underwent definitive surgery (total thyroidectomy with or without lymph node removal depending on stage). The probability of a malignant nodule found on lobectomy (62.5%) was assumed to be the same across all groups. We recognize that some FNABs will be determined “insufficient” or “nondiagnostic.” In this model, we assumed that those people re-entered the model and had subsequent FNAB diagnoses. To account for this cost, the FNAB cost was increased by 10% (38).
The AJCC system was used to stratify those diagnosed with thyroid cancer into three different groups: local (stage I/II), regional (stage III), and remote (stage IV) disease on presentation. The stratification was chosen because clinical outcomes (recurrence, mortality, complications) and cost-effectiveness (costs, extent of long-term follow-up, and quality of life) can be clearly distinguished between these groups. This final endpoint was chosen due to significant differences in the relative risk of thyroid cancer seen in obese patients.
Follow-up
Five-year follow-up of thyroid cancer management followed general management guidelines. The length of five years was chosen given the increased aggressiveness in obese patients of this disease. Most patients who recur with this type of aggressive disease or who have morbidity from this disease do so within five years (39). Additionally, a considerable difference in five-year mortality has been shown in those presenting with later stages (40).
The probability of receiving radioactive iodine (RAI) was estimated to follow current trends. Approximately 38% of the population receives RAI in localized disease, and approximately 100% receive RAI in regional and remote disease (37,41). We determined a 6% rate of chemotherapy only for those with stage IV disease. Recurrence rates for each stage of illness were determined based on a literature review (Table 1).
Complications
The risk of recurrent laryngeal nerve (RLN) injury for those with US screening was that of the general population (1.9%). Risk of RLN injury in the base case nonscreening was set higher (17%). This was based on previous studies performed by our group, which showed a significantly higher rate of preoperative vocal cord paralysis due to local invasion (odds ratio 9.2) (8). Risk of permanent hypoparathyroidism was similar across all groups for an initial operation (1.9%) and reoperation (5%) (14,42). The recurrence rate was assumed to be similar across all groups and depended on the stage (43,44) (Table 1).
Costs
Costs for management, surgery, and follow-up are summarized in Table 3. The costs for laboratory tests were obtained from the 2012 Medicare Clinical Laboratory Feed Schedule (45). Direct medical costs were estimated using reported Medicare charge and reimbursement data. The inpatient costs were estimated by calculating the Medicare cost-to-charge ratio of 0.145 for Diagnosis-Related Groups (DRGs) 627 from the Medicare Provider Analysis Review database. Anesthesia costs were calculated using the following formula: (base units+time units+modifying units)×conversion factor, where base unit=6, time units=# min procedure/15, and conversion factor national average=21.10. The outpatient costs were estimated on the basis of national facility rates from the Medicare Hospital Outpatient Prospective Payment system for their corresponding outpatient Current Procedural Terminology (CPT) codes. Costs of complications and chemotherapy were obtained from previous studies (46,47).
LFSC, lab fee schedule codes.
Total costs for each branch of the decision-tree analysis can be seen in Table 3. In the decision analysis tree, “no further testing” resulted in a cost of $0. “Follow-up” of benign FNAB consisted of an US, laboratory testing (free thyroxine and TSH), and a clinician/endocrinology visit. “Follow-up” of benign lobectomy consisted of an US, laboratory testing (free thyroxine and TSH), a clinician/endocrinology visit, and levothyroxine costs (assuming a 35% patient need for levothyroxine replacement) (48). Treatment costs of each stage incorporated preoperative US, surgical consult, inpatient costs, surgical costs (surgery, anesthesia, cytopathology), levothyroxine costs, and five-year follow-up. Five-year follow-up for each stage consisted of labs (free thyroxine and TSH), routine neck US at each visit, and the cost of clinician/endocrinology visits. Stage I/II patients were followed at six months, and one, three, and five years. Stage III and stage IV patients were followed at six months and every year for five years, and received a single diagnostic whole body scan. For those receiving RAI, lab values of stimulated TSH and thyroglobulin antibodies were drawn every one, three, and five years.
Costs of recurrence and/or chemotherapy were built into each stage based on probability. Complication costs (surgical morbidities, RLN injury, and hypoparathyroidism) and chemotherapy treatment were estimated from costs gathered from previous studies (45 –47). The cost of recurrence was based on the use of a modified radical neck dissection for surgery, but otherwise assumes the patient re-enters the decision model and incurs costs of treatment and probability of complications. Calculations of costs and probabilities of recurrence were similar to estimates of other studies (14,37,49).
Sensitivity analysis
Sensitivity analysis was used to test the level of uncertainty of reference case assumptions. Clinically relevant variables that affect the analysis the most were tested independently across a range of possible values to determine the impact on cost savings and effectiveness. US costs varied between $0 and $1200. The impact of the prevalence of various risk factors for thyroid cancer was examined and varied between 0% and 20%. A total model sensitivity analysis of all variables could not be done, since the sum of the probabilities of each arm (e.g., FNAB result malignant) are nonindependent due to clinical variability (e.g., risk factors, prevalence).
Results
Cost analysis
A summary of outcomes from the decision-tree analysis is given in Table 4. The average cost per person for evaluation of a thyroid nodule in our base case scenario without screening was $210.73. The average cost of US screening for all obese patients for thyroid cancer was calculated to be $434.10 per person and was not cost-effective in relation to the base case scenario. However, risk-based screening was more cost-effective than the base case, resulting in a total per person cost of $166.72, a cost savings of 21% in comparison to the base case.
Sensitivity analysis
As the cost of US was between $0 and $1200, the risk-based screening strategy remained more cost-effective relative to the base case (up to an US cost of $1113) per obese patient screened (Fig. 2). When the prevalence of risk factors was varied between 0% and 20%, the risk-based arm continued to be cost-effective until more than 14% of obese patients were screened (Fig. 2). This indicated cost-efficiency had relatively low sensitivity to US cost variability and a limited sensitivity to a percent range of patients with risk factors.
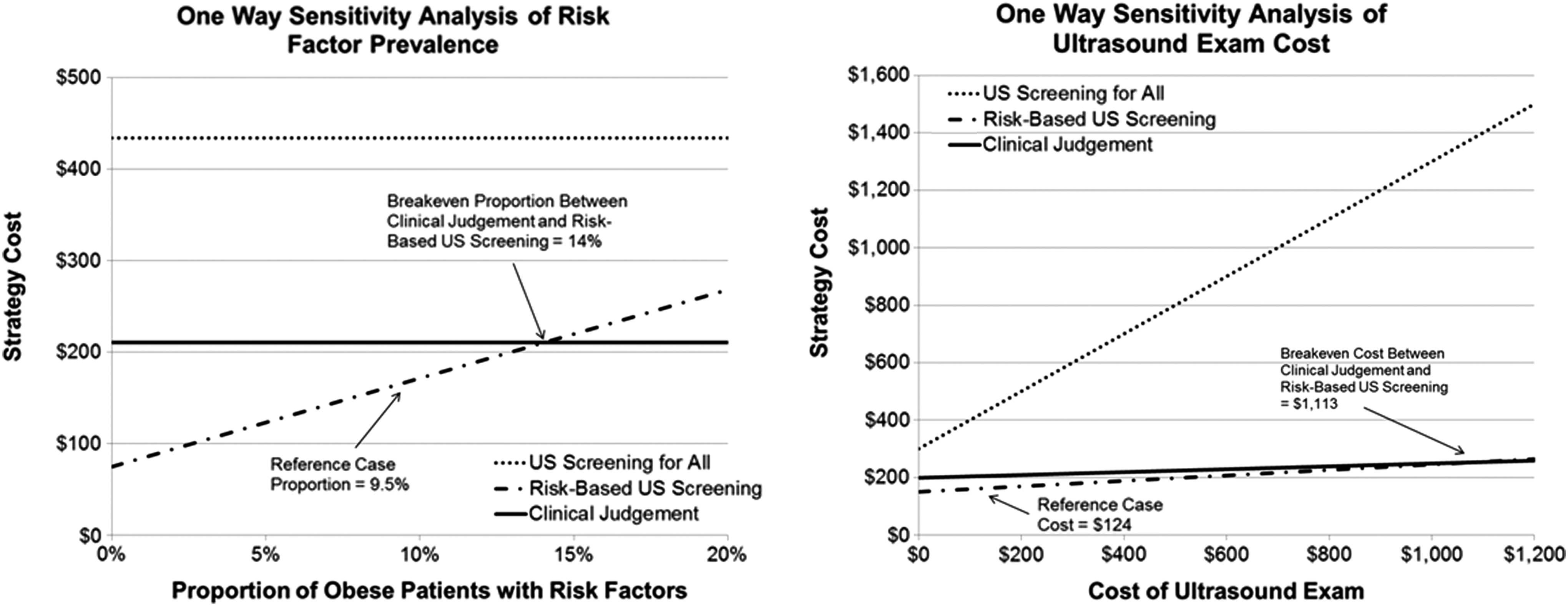
One-way sensitivity analysis of variable cost of ultrasound and risk-factor prevalence.
Discussion
This study demonstrates that US screening is a cost-effective strategy for a subset of obese patients who have additional well-established risk factors for thyroid cancer, including: family history, radiation exposure, Hashimoto's thyroiditis, and/or elevated TSH. This suggests that obese patients over the age of 46 years who have known risk factors should undergo thyroid cancer US screening.
Other studies on the cost-effectiveness of initial diagnostic strategies and the management of thyroid carcinoma have been examined in the past (14,50 –52). For example, FNAB was shown to be the most cost-saving diagnostic tool for distinguishing between benign and malignant nodules (50). Molecular testing for indeterminate FNABs has also been shown to be cost-effective (52). The use of calcitonin in routine screening of thyroid nodules has been implicated to be cost-effective with respect to life years saved (51). In the treatment of low-risk papillary thyroid cancer, total thyroidectomy was shown to be more cost-effective than hemithyroidectomy (14). However, to our knowledge, this is the first study to evaluate the cost-effectiveness of screening in the long-term management of thyroid cancer in obese patients.
The utility of US screening in thyroid nodules has been studied. US in one study was shown to be the most effective initial diagnostic strategy to classify palpable nodules correctly as benign or malignant (but more costly relative to FNAB in short-term diagnostic costs) (50). The prevalence of both palpable and nonpalpable thyroid nodules in the general population of the United States is approximately 30% (with a slight increasing trend with age). Five percent of these are usually malignant (34). Because of this high prevalence of thyroid nodules in the general population with low malignancy potential, US screening has not been thought of as cost-effective for all patients.
The sensitivity of US in detecting nodules and their malignant potential is quite high. In one study, using a combination of sonographic features (e.g., irregular nodular margins, intranodular vascular pattern), 87% of cancers could be accurately detected with US alone (53). Thus, the use of initial US screening followed by FNAB would be an effective strategy for the management of nonpalpable nodules in the obese population, a subpopulation with known risk factors of aggressive disease.
Even though “no cancer screening” for the general population would be less costly, we as a society have accepted the cost of general screening for several types of cancers (colon, breast, cervical, etc.) in order to improve outcomes, reduce morbidity, and reduce mortality, all of which benefit society as a whole. Current recommendations made by the American Cancer Society indicate all individuals should be screened for thyroid cancer (12). However, thyroid cancer treatment and follow-up is long and extensive (14,15). Thus, screening for this cancer must take into account the perioperative costs and benefits. This is one of only a few studies to quantify the cost-effectiveness of screening, inclusive of the cost of long-term cancer surveillance. In those with higher stage or more aggressive cancers, it is clear that the cost increases drastically and quality of life decreases. Obese patients are not only at a higher risk for thyroid cancer (4 –7) but also have been shown to present with more aggressive thyroid cancers (8). They are also a much more vulnerable group due to the difficulty of physically palpating nodules in the obese neck.
Despite the increased risk of aggressive thyroid cancers in the obese, we have shown that in an obese patient, nonselective US screening was not cost-effective, despite the fact that they present in a later stage at baseline. This could be due to overdiagnosis of thyroid cancers and the requirement of further treatment and surveillance. Based on previous studies (23,31 –33), however, we estimated that selected risk factors (family history of thyroid cancer, significant history of radiation exposure, Hashimoto's thyroiditis, and/or elevated TSH) were present in an average of 9.5% of obese patients with an average relative risk of malignancy of 5.0 (23 –30). These values substantially decrease the number of patients receiving US screening and increase the probability of finding malignancy. By limiting the screening to those at high risk, this resulted in cost savings and afforded patients a higher quality of life relative to the base case scenario. This would suggest that one could prevent severe local and systemic complications in this subpopulation by using US screening.
Of note, Hashimoto's thyroiditis was included in the risk factors for thyroid cancer. We acknowledge that there has been controversy and conflicting data about the true effect of this risk factor on the occurrence of thyroid cancer. In our model, the effect is minimal. If this risk factor were eliminated, the analysis would use the same percentage of risk factors (9.5%), and the relative risk of more aggressive disease would be even higher in obese patients (increasing to 5.7 instead of 5.0). Thus, if anything, the effect we have shown by including Hashimoto's as a risk factor is more conservative. Our conclusions would more strongly support US screening if we eliminated this risk factor.
Studies have also shown that thyroid cancer disease-specific mortality rates increase in populations with delayed thyroid cancer treatment (9,10). Recurrence and metastatic disease is highly dependent on the size and aggressiveness of the neoplasm when discovered (11). Surgical complications, disease management, and long-term follow-up are also dependent on the aggressiveness of the cancer (1,8,14,37,42 –44,54). In our study, we found that if a nodule was malignant, a higher stage resulted in an overwhelming increase in the costs and quality-of-life changes in patients with thyroid cancer. Our analysis may have actually underestimated the benefit-to-cost ratio. The relatively high sensitivity and specificity of US, as compared to palpation, may even skew the proportion of screened patients toward lower stage cancers (I/II) due to earlier detection. Furthermore, our follow-up time period was only five years. The base case reference's potential remaining life expectancy is another 35 years, and an even more long-term analysis may have shown a greater benefit-to-cost ratio.
A potential limitation of the model is the assumption that obese patients will have the same cancer stage distribution as the normal population if screened with US. This would assume that obese patients and nonobese patients have the same pathophysiology of disease. It has been suggested, however, that another potential cause of more aggressive tumor types within the obese population is due to a difference in biology (55). Another limitation to our study is that certain variables required extrapolation or expert opinion when data were not available. The risk factors and certain probabilities were estimated from the nonobese population. However, these estimated values are unlikely to change the cost-effectiveness calculated, since they were used similarly across all groups compared.
An additional issue with the model is that we chose to do a thyroid lobectomy for those patients with indeterminate thyroid nodules even if they had a history of radiotherapy, a family history of thyroid cancer, or their diagnosis on FNAB was suspicious for malignancy. These patients are sometimes offered total thyroidectomies as an initial option given the high risk of malignancy in an indeterminate nodule in patients with those risk factors (50–70%) (56). However, this is not a standardized treatment protocol. Thus, we chose to use the more conservative and more costly surgical approach, which is to perform a lobectomy for diagnosis and a completion thyroidectomy if the lesion was found to be malignant. Thus, it is not surprising that when we did rerun the model as though all patients with these risk factors got total thyroidectomies, it did not change the conclusion. In fact, it showed a greater cost-effectiveness to screening obese patients.
The risk factors chosen for this analysis were based on extensive literature review and expert opinion of the most well-known associations of the development of differentiated thyroid cancer (23 –30). We chose to focus on the obese population due to the difficulties in screening, thus altering their initial presentation and the complications associated with their diagnosis. Future work of interest includes examining whether US screening retains its cost-effectiveness in the general population with these risk factors as well.
Conclusion
While we recognize that US screening of the general obese population may be unfeasible, we have found that in obese patients with established risk factors (family history, radiation exposure, Hashimoto's, elevated TSH), US screening for thyroid cancer is cost-effective. Thus, consideration for using US for thyroid cancer screening among targeted subgroups of obese patients is warranted and will likely decrease morbidity and mortality in this subpopulation with aggressive disease.
Footnotes
Acknowledgments
There are no outside sources of funding/support.
Author Disclosure Statement
The authors have nothing to disclose.