
Abstract
Background:
Agranulocytosis is a serious adverse effect of antithyroid drugs (ATDs) and mainly develops within three months after the start of uninterrupted ATD treatment. Agranulocytosis can also develop for the first time after interruption and subsequent resumption of the same ATD treatment. However, little is known with regard to agranulocytosis that develops after resumption of the same ATD treatment.
Objectives:
We investigated the characteristics of patients who developed agranulocytosis during their second or later course of ATD treatment.
Methods:
A total of 81 patients at our hospital were diagnosed with ATD-induced agranulocytosis. In 14 of the cases (methimazole (MMI), n=10; propylthiouracil (PTU), n=4), the agranulocytosis developed for the first time in the context of the second or later course of treatment with the same ATD; those patients were designated the “resumed group.” The 35 patients (MMI, n=28; PTU, n=7) who developed agranulocytosis during their first uninterrupted course of ATD therapy were designated the “first group.”
Results:
The median total duration of ATD treatment before the diagnosis of agranulocytosis was 559 days (range 86–1775 days), and the median interval between the final day of the previous course and the first day of the course in which agranulocytosis was diagnosed was 916.5 days (range 153–8110 days). There were no cases in which agranulocytosis developed when treatment with the same ATD was resumed after discontinuation for less than five months. The difference between the start of ATD treatment in the course in which agranulocytosis was diagnosed and the time interval at which agranulocytosis was diagnosed was similar when comparing the first group and the resumed group (39 (20–98) days in the first group vs. 32.5 (21–95) days in the resumed group; n.s.). There were no significant differences between the groups in terms of granulocyte count at the time agranulocytosis was diagnosed, mortality rate, or the interval between the diagnosis of agranulocytosis and recovery.
Conclusions:
When ATD treatment is resumed, patient follow-up is essential in order to monitor for the development of agranulocytosis.
Introduction
A
The present study reviewed cases of patients with Graves' disease who were diagnosed with ATD-induced agranulocytosis at our hospital, and investigated the clinical characteristics of the patients who developed agranulocytosis during their second or later course of ATD treatment. We also compared the clinical characteristics of these patients with those of patients who developed agranulocytosis during the first uninterrupted course of treatment with an ATD.
Subjects and Methods
Electronic medical records were reviewed, and a total of 87 patients at Ito Hospital, Tokyo, Japan, were identified who had been diagnosed with agranulocytosis between July 1983 and August 2012. As shown in Figure 1, six of these 87 patients were excluded from our study because their agranulocytosis was attributed to a viral infection or drugs other than ATD (e.g., cefditoren pivoxil, enalapril, etc.). We defined the second or later course of ATD treatment as one that began after an interval of more than 30 days after the end of a previous course of treatment with the same ATD, irrespective of switching from the other ATD or restarting the same ATD after any ATDs were stopped. Twenty-two patients developed agranulocytosis during their second or later course of ATD treatment, and 14 of these patients who did not exhibit leukopenia, granulocytopenia (granulocyte count below 1000/μL), or agranulocytosis (granulocyte count below 500/μL) in any previous uninterrupted course (more than eight weeks) of ATD treatment were designated the “resumed group.” Eight patients were not included in the resumed group because (i) they had exhibited leukopenia during the first course of treatment with the same ATD (n=3); (ii) there was less than eight weeks of continuous therapy in the previous course (n=5, two cases were in common with the first criterion); (iii) the interval between the final administration of the previous course and the first day of the course in which agranulocytosis was diagnosed was less than 30 days (n=1); or (iv) ATD treatment was resumed at another hospital, and the exact day on which ATD treatment was resumed was unknown (n=1). Forty-five patients developed agranulocytosis during their first course of ATD therapy, and 35 of these patients who took the ATD continuously (as verified by prescription renewal within 1.1 times as many days since the previous prescription had been written) were designated as the “first group.” Fourteen patients could not be classified into either the first group or the resumed group because (i) the ATD prescribed in the previous hospital was unknown (n=4); (ii) treatment with an ATD was started at a different hospital, and it was not known whether there was an interval of 30 days since the previous course (n=9); or (iii) the causative ATD could not be confirmed because of subsequent short-term treatment with a different ATD (MMI for 19 days, then PTU for 5 days; n=1; Fig. 1).
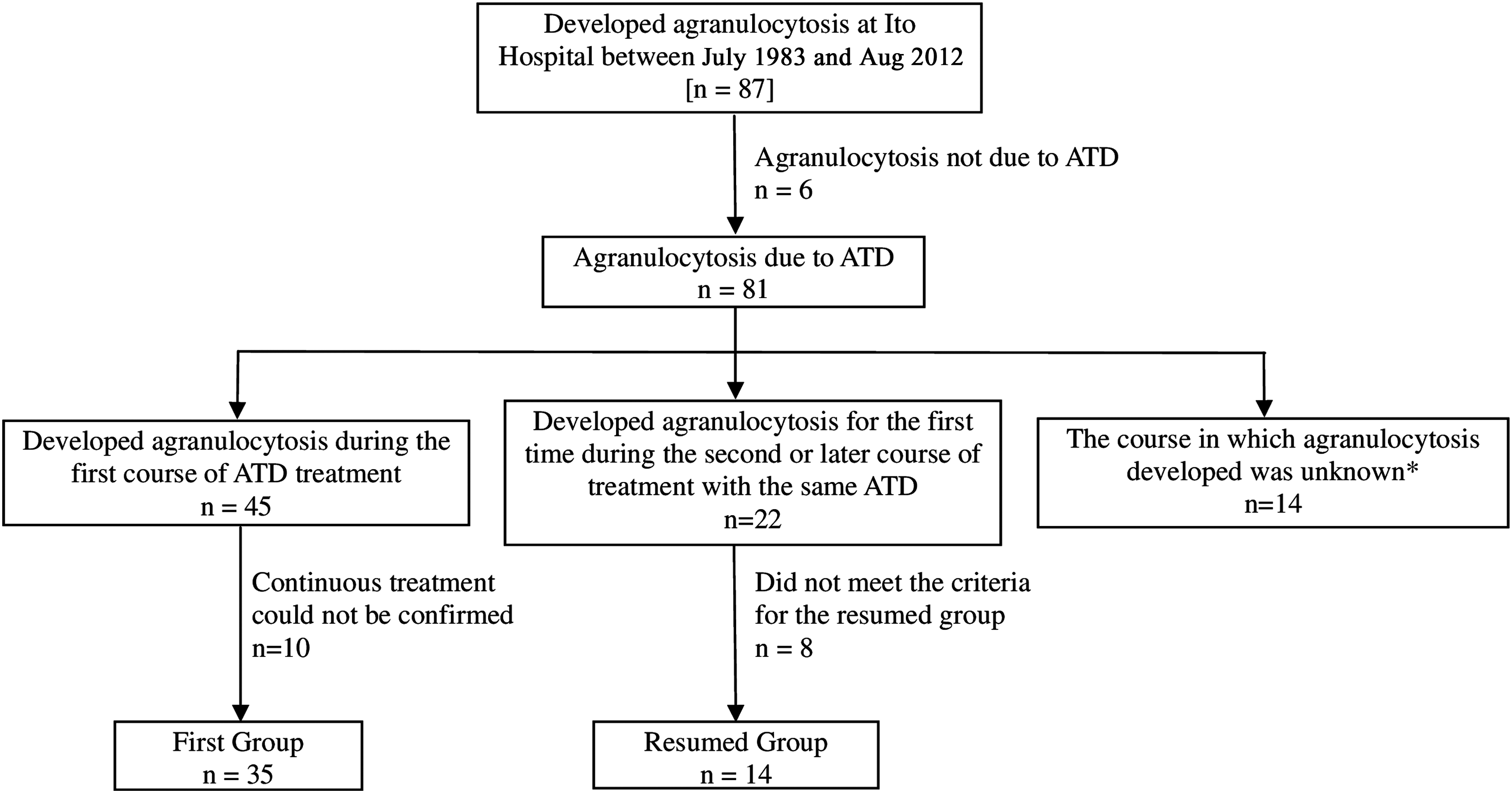
Flowchart of patients who developed agranulocytosis. *The antithyroid drug (ATD) prescribed in the previous hospital was unknown (n=4). Treatment with the ATD at the previous hospital was started more than 30 days before admission to our hospital, and it was unknown whether the discontinuation period was more than 30 days (n=9). The causative ATD could not be identified because a different ATD was subsequently prescribed (methimazole [MMI] for 19 days, then propylthiouracil [PTU] for five days; n=1).
Diagnosis of ATD-induced agranulocytosis
A diagnosis of ATD-induced agranulocytosis was made when the granulocyte count fell below 500/μL after treatment with an ATD (13). The patient was determined to have recovered from agranulocytosis when the granulocyte count reached 1000/μL or more.
Statistical analysis
Statistical analysis was performed with JMP software v10.0 (SAS Institute, Inc., Cary, NC). Continuous variables are shown as median values along with the smallest variable and the largest variable. Categorical variables are expressed as rates and proportions. Differences in the data for continuous variables between the two groups were analyzed by the Mann–Whitney test (nonparametric test), as they were continuous variables without normal distribution. Differences between categorical variables were analyzed by the chi-square test and by Fisher's exact test when appropriate. A p-value of <0.05 was considered to represent statistical significance.
Results
The characteristics of the 14 patients in the resumed group—10 of whom were being treated with MMI, and four of whom were being treated with PTU at the time agranulocytosis was diagnosed—are shown in Table 1. Agranulocytosis developed during the second course of ATD therapy in nine patients in the resumed group, during the third course in four patients, and during the eighth course in one patient. The median total duration of ATD treatment before agranulocytosis was diagnosed (total duration of the first course and the later courses were combined) in the resumed group was 559 days (range 86–1775 days). The median interval between the final day of the previous course and the first day of the course in which agranulocytosis was diagnosed (discontinuation period) was 916.5 days (range 153–8110 days). Interestingly, there were no cases in which agranulocytosis developed after the same ATD was resumed after a discontinuation period of less than five months. Ten patients had been treated with two different ATDs (i.e., MMI and PTU) before the diagnosis of agranulocytosis, and nine of these patients had experienced minor adverse effects, including skin eruptions, pruritus, hair loss, slight fever, and liver dysfunction, when previously treated with the other ATD.
Interval between the final day of the previous course and the first day of the course in which agranulocytosis was diagnosed.
ATD, antithyroid drug; MMI, methimazole; PTU, propylthiouracil.
Thirty-five patients—28 patients treated with MMI and seven patients treated with PTU—met the criteria for inclusion in the first group. The clinical characteristics of the first group and the resumed group are summarized in Table 2. The difference between the start of ATD treatment in the course in which agranulocytosis was diagnosed and the time the diagnosis of agranulocytosis was made was similar when comparing the first group and the resumed group (39 (range 20–98) days in the first group vs. 32.5 (range 21–95) days in the resumed group; p=0.6416). There were no significant differences between the groups in terms of leukocyte count (1919±1035/μL vs. 1370±75/μL; p=0.0879), granulocyte count (68/μL (range 0–295/μL) vs. 78/μL (range 0–432/μL); p=0.6793]), febrile episodes (63% vs. 75%; p=0.5054), documented infection (29% vs. 50%; p=0.1764), pancytopenia (5.7% vs. 7.1%; p=1.0000) at the time agranulocytosis was diagnosed, or mortality rate (5.7% vs. 0%; p=1.0000). Among three patients who developed pancytopenia (two patients in the first group and one patient in the resumed group), two patients in the first group died of infection. A bone marrow biopsy was performed in one patient in the first group and in one patient in the resumed group, and their marrows were hypoplastic. The intervals between the diagnosis of agranulocytosis and recovery in the two groups were similar (7 days (range 0–22 days) vs. 6 days (range 1–13 days); p=0.9724). There was a significant difference between the first and the resumed group in the rate of patients who had experienced minor adverse effects when treated with the other ATD, among patients who had been treated with two different ATDs before the diagnosis of agranulocytosis (p=0.0050).
Interval between the start of ATD treatment in the course in which agranulocytosis was diagnosed and the diagnosis of agranulocytosis.
Not significant (NS) due to the small sample size (first group n=6; resumed group n=4).
Interval between the diagnosis of agranulocytosis and recovery.
Rate of patients who had experienced minor adverse effects when treated with the other ATD, among patients who had been treated with two different ATDs before the diagnosis of agranulocytosis.
Discussion
Agranulocytosis is one of the most serious adverse effects of ATDs. The cause of ATD-induced agranulocytosis is not completely understood, but an immune-mediated mechanism has been proposed. Some reports suggest that an antibody against mature blood cells and bone precursor cells is involved in the etiology of the agranulocytosis induced by ATDs (10,14), while other studies have reported that an autoimmune mechanism that targets an antigen on neutrophils is involved in the etiology of ATD-induced agranulocytosis (15). An association between the development of ATD-induced agranulocytosis and certain HLA class II haplotypes has also been reported (16). Agranulocytosis is also caused by other drugs (e.g., clozapine, penicillin G, procainamide, rituximab, ticlopidine, cefditoren pivoxil, enalapril, etc.), viral infections, congenital agranulocytosis, and cyclic neutropenia (17 –19).
Table 3 summarizes data from several previous reports of agranulocytosis that first developed during the second course of treatment with the same ATD. There have been four reports on the interval between the start of the second course of ATD treatment and the onset of agranulocytosis (3,6,9,10). The intervals were mainly within two months, although two exceptions were reported by Tamai et al. (13 and 18 months) (3). Tajiri et al. reported no significant difference in the interval between the start of treatment with MMI and the onset of agranulocytosis when comparing a group in which agranulocytosis developed during the first course of treatment with MMI (n=31) and a group in which agranulocytosis developed during the second course of treatment with MMI (n=6) (6). In the present study, there was no significant difference between the first group and the resumed group in the interval between the start of ATD treatment in the course in which agranulocytosis was diagnosed and the time at which the diagnosis of agranulocytosis was made. There was no significant difference between the first and the resumed group in other clinical parameters or in leukocyte count, granulocyte count, febrile episode, documented infection, pancytopenia at the time agranulocytosis was diagnosed, mortality rate, or the intervals between the diagnosis of agranulocytosis and recovery. These data demonstrate that duration after starting or resuming ATD until the development of agranulocytosis was the same, and that the clinical severity of agranulocytosis was the same when comparing the two groups.
Interval between the final day of the previous course and the first day of the course in which agranulocytosis was diagnosed.
N/A, not available.
There have been three reports regarding ATD discontinuation periods: one involving MMI, and two involving PTU. Tamai et al. described four cases in which agranulocytosis developed during the second course of treatment with MMI, and the shortest discontinuation period was five months in a patient treated with MMI (3). Shiran et al. described four cases, and Fibbe et al. described one case in which agranulocytosis developed during the second course of PTU treatment, and the shortest discontinuation period was three years (9,10). These results are consistent with those from the present study, in which the shortest discontinuation was 153 days for MMI and 987 days for PTU. Shiran et al. raised the possibility that the discontinuation period might be longer in relation to PTU than in relation to MMI. Our data showed a tendency for a discontinuation period to be shorter in the MMI group (median 710.5 days (range 153–4567 days); n=10) than in the PTU group (median 6878 days (range 987–8110 days); n=4; Table 1), but this difference did not reach the level of statistical significance, possibly due to the small sample size.
The American Thyroid Association recommends that pregnant women who were started on MMI before their pregnancy be switched to PTU during the first trimester and then changed back to MMI after the second trimester (11). When following this recommendation, treatment with MMI is resumed as much as three months after discontinuation of treatment with MMI. No previous study has investigated the risk of developing agranulocytosis in cases in which treatment with MMI was resumed after such a short discontinuation period. As discussed above, the shortest discontinuation period was five months for MMI in the previous report and in the present study. Although the studies are small, these data suggest that agranulocytosis is unlikely to develop when ATD is resumed after a short discontinuation period (i.e., within five months). It is possible that some minimum duration of ATD discontinuation period is necessary to lose the inhibitory factors or mechanisms that prevent patients from developing agranulocytosis, such as T-suppresser cells or blocking antibodies (9). Another possibility is that the number of cases in which ATD was resumed after a short discontinuation period (i.e., within five months), including patients developing agranulocytosis and those not developing agranulocytosis, might be too small. This could account for the lack of reports of patients in which agranulocytosis occurred when MMI was resumed after such a discontinuation period. However, the number of pregnant women in which MMI is resumed after a short discontinuation period is increasing because of the guidelines issued by the American Thyroid Association. Therefore, clinicians might begin to encounter more cases in which agranulocytosis develops when MMI is resumed after such a short discontinuation period.
Interestingly, there was a significant difference between the first and the resumed group in the rate of patients who had experienced minor adverse effects when treated with the other ATD, among patients who had been treated with two different ATDs before the diagnosis of agranulocytosis (Table 2). This result suggests that resumption of ATD treatment should be avoided in patients who have experienced a minor reaction that prompted the discontinuation of the first ATD.
Of note, Cooper et al. reported that the frequency of agranulocytosis did not increase in patients who received a previous course of treatment with the same drug (5), whereas Shiran et al. reported that the incidence of agranulocytosis increased when PTU was resumed (0% in the first course vs. 7.2% in courses after the first course). However, in our study, we were unable to show the incidence of agranulocytosis.
In conclusion, when ATD treatment is resumed, patient follow-up is essential in order to monitor for the development of agranulocytosis.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing financial interests.