
Abstract
Background:
Overt neonatal Graves' disease is rare, but may be severe, even life threatening, with deleterious effects on neural development. The main objective of this study was to describe the course of thyrotropin (TSH) and free thyroxin (fT4) levels, as well as postnatal weight gain in relation to fT4 levels, in neonates born to women with Graves' disease without overt neonatal thyrotoxicosis. Such information is important to deduce the optimal schedule for evaluation.
Methods:
We conducted a retrospective chart review of neonates born to mothers with Graves' disease between January 2007 and December 2012. The records were reviewed for sex, gestational age, birth weight, maternal treatment during pregnancy, and maternal thyroid stimulating immunoglobulin (TSI) level. For each visit in the clinic, the data included growth parameters, presence of symptoms suspected for hyperthyroidism, blood test results (levels of TSH, fT4, and TSI), and treatment.
Results:
Ninety-six neonates were included in the study (49 males), with a total of 320 measurements of thyroid function tests (TSH and fT4). Four neonates (4%) had overt neonatal Graves' disease; one of them along with nine others were born preterm. In 77 (92.9%) of the remaining 83 neonates (the subclinical group), fT4 levels were above the 95th percentile on day 5. All had normal fT4 on day 15. A negative association was found between fT4 and weight gain during the first two weeks.
Conclusions:
In this cohort, most neonates born to mothers with Graves' disease had a subclinical course with abnormal fT4 levels that peaked at day 5. After day 14, all measurements of fT4 returned to the normal range, although measurements of TSH remained suppressed for up to three months. Elevated fT4 was associated with poor weight gain.
Introduction
N
Maternal thyroid antibody positivity during pregnancy is associated with negative pregnancy outcomes, including miscarriage and preterm delivery (11). Fetal hyperthyroidism may develop during the second half of gestation and cause fetal goiter, impaired growth, advanced bone maturation, and fetal tachycardia (12). Therefore, close follow-up during pregnancy is advised for women who have a current or past history of Graves' disease (13,14). A maternal serum determination of thyrotropin (TSH) receptor antibodies (TRAb) should be obtained at 20–24 weeks' gestation (13,14). Fetal surveillance should be performed in women who have uncontrolled hyperthyroidism and/or women with high TRAb levels (13). Such monitoring may include serial ultrasound for heart rate, growth, amniotic fluid volume, and fetal goiter (15). Umbilical blood sampling should be considered only if the diagnosis of fetal thyroid disease is not reasonably ascertained from the clinical and sonographic data (14). Fetal hyperthyroidism is usually treated with maternal ATD treatment (16).
After birth, neonates at risk of neonatal thyrotoxicosis require close observation and evaluation. Neonatal clinical manifestations may be apparent at birth but are usually delayed for some days due to the effect of maternal ATD (17,18). Common manifestations include neonatal tachycardia, tachypnea, poor weight gain with good appetite, and irritability (19). Other signs are hepatomegaly, splenomegaly, cardiac insufficiency, and liver dysfunction (20). Thyrotoxicosis resolves 3–12 weeks postpartum with the disappearance of maternal antithyroid antibodies from neonatal circulation (21). The cardiac manifestations usually determine the short-term prognosis, while the long-term prognosis is associated with neurodevelopmental abnormalities (22).
Overt clinical neonatal hyperthyroidism has been well researched. The current study focuses on neonates without clear clinical symptoms of hyperthyroidism, which comprise the majority of those born to mothers with Graves' disease. Our objective was to describe the course of TSH and free thyroxin (fT4) levels in these neonates. Such information is important to deduce the optimal schedule for evaluation. In addition, we investigated characteristics of gestational age, birth weight, and postnatal weight gain as subclinical manifestations of neonatal hyperthyroidism.
Methods
The study was approved by the Institutional Review Board of Sheba Medical Center, Ramat Gan, Israel. This is a retrospective chart review of all neonates born to mothers with Graves' disease who were consecutively referred to the Pediatric Endocrine Unit in Edmond and Lily Safra Children's Hospital between January 2007 and December 2012. At our hospital, all newborns of mothers with current or past history of Graves' disease (including those who have had ablative treatment with surgery or radioiodine) are supervised closely during the first few days after delivery. Blood tests for TSH and fT4 are taken routinely when the neonates are two to three days old. In the absence of signs or symptoms of hyperthyroidism, all babies are discharged with a recommendation for repeated blood tests (TSH and fT4) and examination in our Pediatric Endocrine Unit during the following week. After the first visit in the clinic, further follow-up and management are decided upon as needed.
A total of 96 records were reviewed for the following data: sex, gestational age, birth weight, levels of TSH and fT4 taken at the nursery, maternal treatment during pregnancy, and maternal TSI level in the year before the delivery. For each visit in the clinic, the data included weight, height, head circumference, presence of symptoms suspected for hyperthyroidism, TSH and fT4 levels, and treatment.
Weight gain was calculated as the difference between the weight on days 10–14 and the birth weight, since newborns generally return to their birth weight by the second week. Weight gain was calculated for 29 children with weight measurements on days 10–14. There was no difference in birth weight, sex, and gestational age distributions in groups with and without weight data on days 10–14.
At our medical center, TSH and fT4 are measured using the UniCel™ DxI 800 Access Immunoassay System (Beckman Coulter Inc., Brea, CA). TSI is measured using Chinese hamster ovary (CHO) cells stably expressing human TSH receptor. Serum immunoglobulin, prepared using polyethylene glycol (PEG) precipitation (final concentration of 20%), is incubated with the cells in 96-well plates for three hours at 37°C. The amount of cAMP accumulated in the cells is then measured by radioimmunoassay (RIA). The resulting data are expressed as the specimen-to-reference ratio (SRR) percent, which is calculated with the following equation: SRR%=[(Average Test RLU)/(average reference control RLU)]×100%. Results are considered positive when SRR ≥140% of the reference control.
Statistical analyses
Statistical analyses were performed using SAS v9.2 (SAS Institute, Inc., Cary, NC). Categorical variables are presented as number (percentages) and continuous variables as mean±SD or median and ranges. TSH and fT4 measures were categorized as below the 5th percentile, normal range (5–95 percentiles), and above the 95th percentiles, according to reference intervals published previously (23,24).
Mean TSH and fT4 levels were determined for each baby during each time period. For longitudinal follow-up, means and confidence intervals were used to calculate the TSH and fT4 levels for the following age intervals: 2–4, 5–12, 13–20, 21–30, 31–60, and 61–95 days.
The Pearson correlation coefficient was calculated between weight gain and fT4 at 10–14 days in 29 babies for whom data were available. We used a linear regression model to analyze the relationship between weight gain and fT4 as an independent variable, and between weight gain and fT4 and birth weight.
The Pearson correlation coefficient was also calculated between maternal TSI level and first measurement of TSH and fT4 of the neonates, as well as between maternal treatment during the pregnancy and infant outcomes: gestational age, birth weight, and first measurement of TSH and fT4.
Data were excluded from the analysis for babies with overt neonatal Graves' disease and for preterm babies (gestational age <37 weeks), since in preterm babies, the thyroid axis is immature, with low levels of TSH and fT4.
Results
A total of 96 neonates (47 females, 49 males) born to mothers with Graves' disease were treated at our center during the study period. A total of 320 measurements of thyroid function tests (TSH and fT4) were performed. Four babies were diagnosed with overt neonatal Graves' disease. One of the babies with overt neonatal Graves' disease and nine others were born preterm (gestational age 34–36 weeks). The remaining neonates (n=83, gestational age 37–41 weeks, with 258 measurements) were defined as the subclinical group. Their clinical characteristics are presented in Table 1, and mean and range values for TSH and fT4 are presented in Table 2. TSI levels were available for 32 mothers (M=241±182%; range 22–792%) and for 14 neonates (M=87±63%; range 0–230%).
ATD, antithyroid drugs (propylthiouracil and methimazol).
TSH, thyrotropin; fT4, free thyroxin.
The course of mean and confidence intervals of TSH and fT4 levels of the subclinical group, computed for six age intervals (2–4, 5–12, 13–20, 21–30, 31–60, and 61–95 days), are depicted in Figure 1 on the background of reference range of newborns. The numbers of measurements for the consecutive time points are 84, 83, 35, 21, 25, and 10. The mean fT4 level was above the 95th percentile during the first 5–12 days of life and then decreased to within the normal range. However, it remained in the upper part of the normal range during the subsequent two months. Mean TSH levels were within the normal range during the entire follow-up period.

Mean and confidence intervals of
Figure 2A and B presents, for the subclinical group, the proportions of fT4 and TSH measurements respectively that were abnormal, that is, below the 5th and above the 95th percentile of the normal range, during the first 17 days of life.
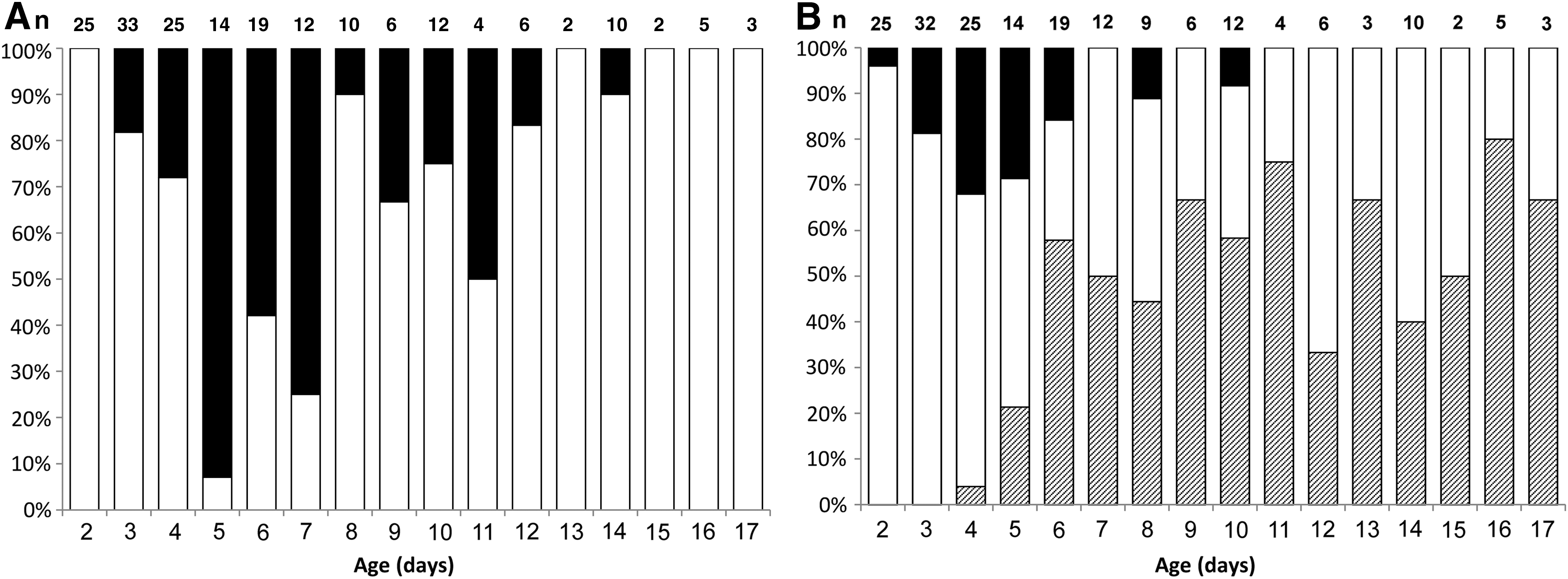
The percent of measurements of
fT4 measurements
No neonate had an fT4 level below the 5th percentile. Most of the results above the 95th percentile were measured between day 3 and day 12. The peak was at day 5 when 92.9% of the measurements were above the 95th percentile. From day 15, all fT4 measurements were within the normal range.
TSH measurements
A considerable proportion of the measurements (16–32%) were above the 95th percentile during days 3–6. From day 5, the proportion of measurements below the 5th percentile increased to more than 60%. Some TSH measurements remained below the normal range for a couple of weeks.
Maternal treatment and neonate outcomes
Of the 83 mothers forming the subclinical group, 43 were treated with ATD during pregnancy, 14 with levothyroxine due to prior thyroidectomy or radioablation, and 16 were not treated. There was no correlation between maternal treatment during the pregnancy and the outcomes of the subclinical group: gestational age, birth weight, and the first measurement of TSH and fT4. Interestingly, three of the four mothers of neonates with overt hyperthyroidism were treated with ATD during pregnancy, and one had radioablation and was treated with levothyroxine—all known risk factors for neonatal hyperthyroidism.
Maternal TSI level and neonate thyroid function
TSI levels were available for 32 mothers. No correlation was found between TSI levels and first measurements of TSH and fT4 of the neonates. It should be noted that for three of the four neonates with overt hyperthyroidism, the TSI value during pregnancy was available, and all had TSI levels above the normal range (Table 3). The most severe case had a TSI level of more than three times the upper limit of normal (patient 1; Table 3).
The family was advised to give propylthiuracil and propranolol, but they preferred close observation only.
ND, not done; TSI, thyroid stimulating immunoglobulins.
Birth weight, gestational age, and weight gain
The mean gestational age of the subclinical group was 38.9±1.2 years, and the mean birth weight was 3168.0±474 g (Table 1). Twenty-nine neonates had both fT4 level and weight measurements on days 10–14. In these neonates, the fT4 level was found to be associated negatively with weight gain, as calculated on days 10–14. An increase of five units of fT4 (pmol/L) was associated with poor weight gain (defined as at least 100 g less gain than expected) on days 10–14 (p=0.04). When the birth weight was added to the analysis, the weight gain was correlated to both birth weight (p=0.02) and fT4 level (p=0.09; Fig. 3).
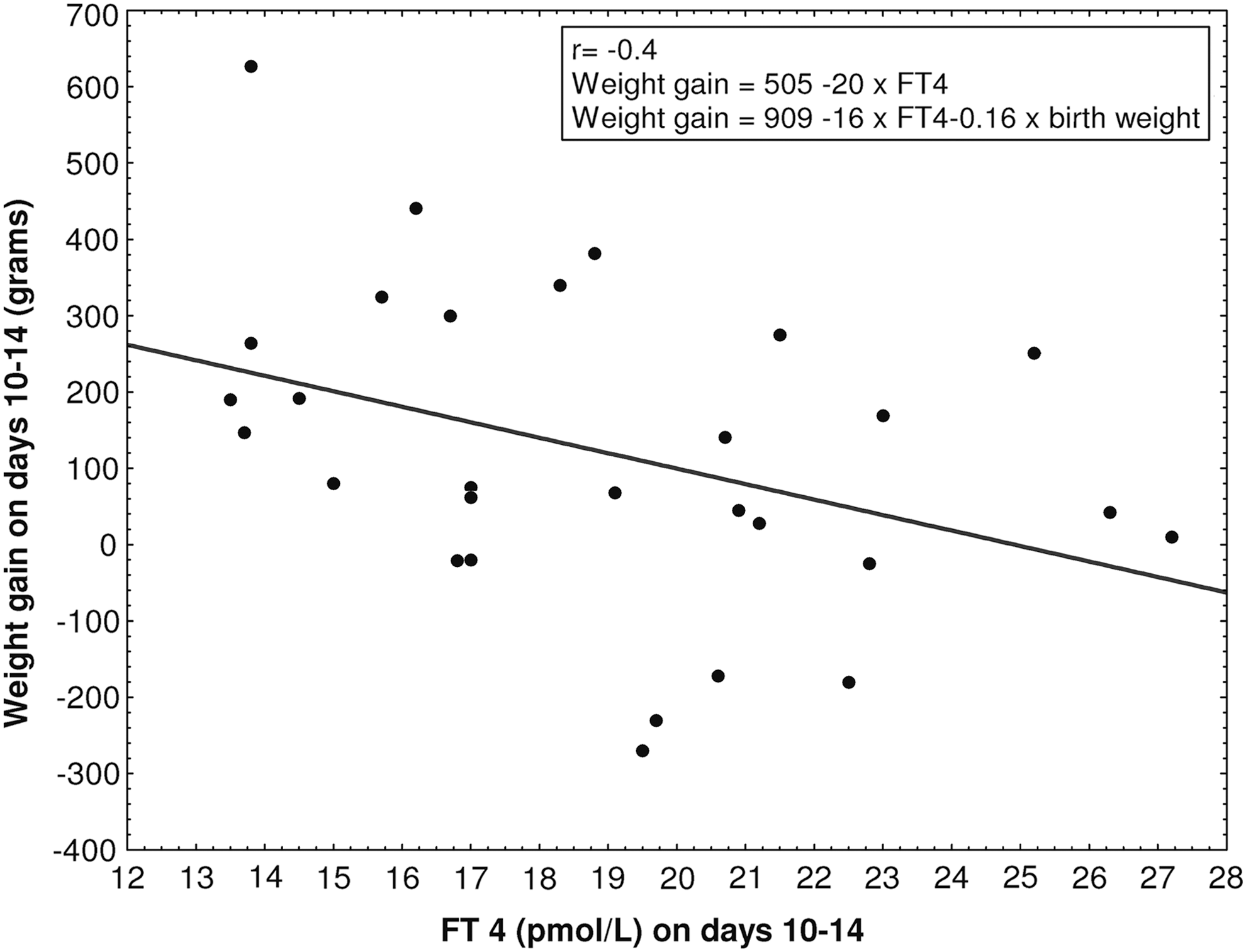
The correlation between fT4 levels, weight gain on days 10–14, and birth weight based on 29 neonates.
Overt neonatal hyperthyroidism
Of 96 neonates born to mothers with Graves' disease, only four had overt neonatal hyperthyroidism. Their data are presented in Table 3. The most severe case (patient 1) was a female infant born to a mother who was diagnosed with Graves' disease a few months prior to conceiving and was treated with propylthiuracil throughout the pregnancy. She delivered vaginally at 39 weeks gestation, complicated by meconium-stained amniotic fluid. Birth weight was 3.210 kg with Apgar scores of 9 and 10 at 1 and 5 minutes respectively. The first physical examination was unremarkable. Laboratory studies at one day old revealed hyperbilirubinemia and polycythemia. She was treated with intravenous fluid infusion and phototherapy. Due to the maternal history, thyroid tests were monitored. Her fT4 and TSH levels for the first two months of life are presented in Figure 4. At one week old, her fT4 level reached a peak of 59.4 pmol/L, and the TSH was suppressed to a level of 0.06 mIU/L. This prompted initiation of propyl thiuracil treatment at a dose of 5 mg/kg/day.
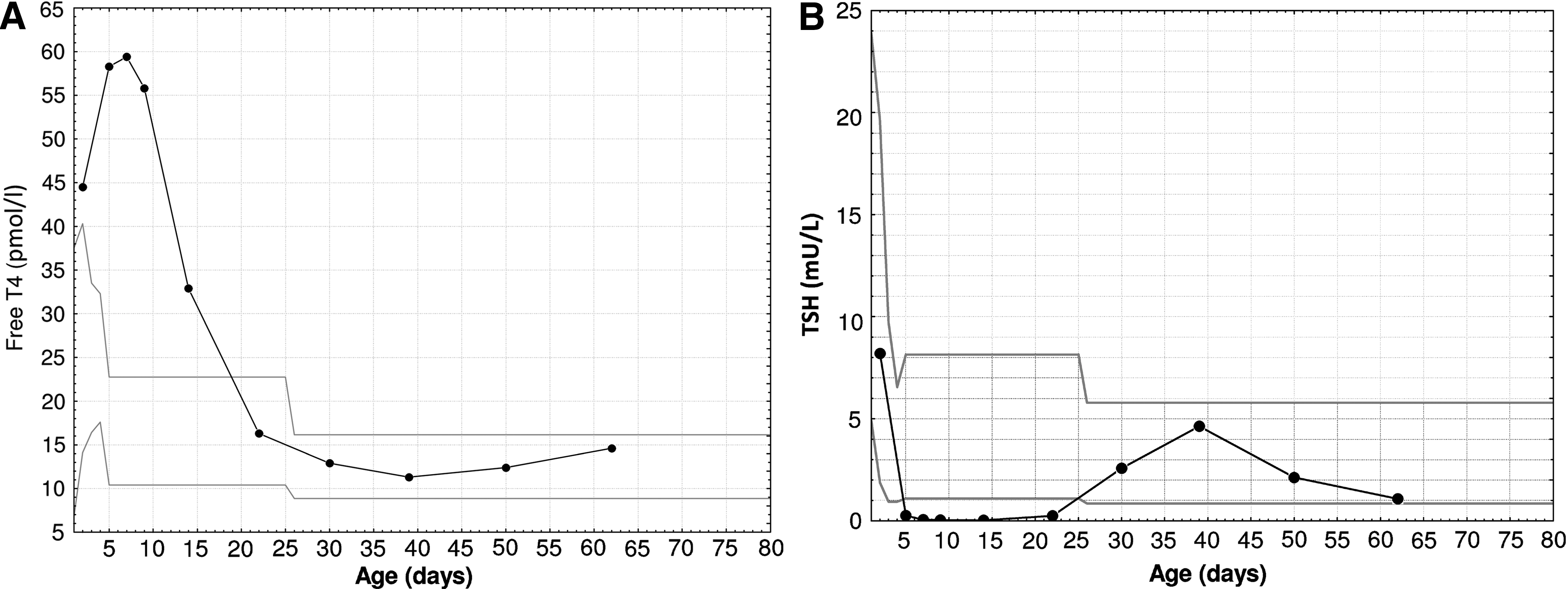
fT4 and TSH levels of patient 1 depicted by the black line. The gray lines represent the reference range (the 5th and 95th percentiles).
Discussion
Four percent of the study group developed overt neonatal hyperthyroidism with greatly elevated levels of fT4 and a suppressed TSH, similar to the rate documented in previous studies (3,4). Their main symptoms were tachycardia and poor weight gain. In the subclinical group, the mean fT4 level between days 5 and 12 was above the normal range. From 14 days old, all measurements of fT4 returned to the normal range, but some measurements of TSH remained suppressed for up to 3 months. We found a negative association between fT4 level and weight gain during the first two weeks of life.
Neonates born to mothers with Graves' disease require close observation and evaluation after birth, including blood tests for thyroid function. However, the exact protocol for blood testing in neonates without clear symptoms—that is, the timing of the first blood test, frequency of blood tests, and duration of follow-up—has not been determined. The situation may be complicated by interaction among factors that impact thyroid function of the neonate: maternal ATD, which usually are cleared within a few days; maternal TSI levels, which are cleared within a few of weeks; and sometimes the effect of coexistent blocking antibodies.
According to the scheme suggested by Oglivy-Stuart, blood tests for TSH and fT4 should be taken from cord blood and again 10–14 days later in all babies. In high-risk cases, blood tests should also be taken at days 2–7 (10). However, in a study of 69 neonates, cord blood T4 and TSH failed to predict subsequent neonatal Graves' disease (1). In that study, transient hyperthyroidism was diagnosed in 6 of the 69 neonates, at a mean age of 4.7 days. Cord blood tests showed hyperthyroidism in two of the six neonates, hypothyroidism in two, and normal thyroid function in two. Thus, TSH and fT4 levels in cord blood reflect fetal thyroid function and do not help to establish the diagnosis of neonatal hyperthyroidism.
Blood tests taken during the first 2–3 days after delivery did not identify overt neonatal hyperthyroidism, and thus did not predict the deterioration that later appeared in the laboratory results and clinical examinations of these babies. Our study demonstrates the importance of measuring thyroid function in neonates of mothers with Graves' disease when the neonates are 3–5 days old. Neonates with fT4 levels above the reference range should be evaluated for symptoms such as irritability, tachycardia, and poor weight gain. Treatment or further supervision should be determined according to the presence of symptoms and thyroid function tests. For neonates with normal fT4 levels on day 14 and no symptoms, there does not seem to be a need for further blood testing. However, they should be followed clinically by a primary care physician, since rare cases of overt hyperthyroidism have been reported to occur even more than a month after birth (17). Moreover, our data demonstrate that TSH values should be interpreted in conjunction with fT4 levels, and with the overall clinical presentation and history of the patient. Both elevated (>95th percentile) and low (<5th percentile) TSH levels were detected within the first days after birth (Fig. 2).
There are several pitfalls in the interpretation of the thyroid function tests in neonates. Normally, serum TSH concentrations rise abruptly to 60–80 mU/L within 30–60 minutes after delivery in healthy term babies. Serum TSH concentrations then decrease rapidly to about 20 mU/L 24 hours after delivery, and then more slowly to 6–10 mU/L at one week. The initial surge in TSH stimulates thyroidal T4 secretion; fT4 concentrations subsequently rise to a peak at 24–36 hours of life. Serum T3 concentrations also rise at the same time. These sharp changes in plasma TSH and thyroid hormones render the interpretation of thyroid tests in neonates difficult.
Moreover, thyroid hormone values are population- and method-dependent (25,26). Several studies have published reference ranges of thyroid hormones in children (23,27 –36). Slight differences in values among these studies can be explained by different analytical assays and by differences in ethnicity, and in population and geographic derived covariates, such as salt iodination and nutrition (30). All these parameters should be taken into consideration when evaluating neonate thyroid test results. Medical centers that treat neonatal hyperthyroidism should establish newborn reference intervals according to their particular populations and testing methods.
This study demonstrated abnormal thyroid tests among most neonates born to mothers with Graves' disease. For a large proportion of them, fT4 levels were above the normal range during days 3–12, with a peak on day 5. Accordingly, TSH levels were suppressed. This finding differs from previous data that showed only 3% of babies of mothers with Graves' disease to have biochemical hyperthyroidism in the absence of symptoms (4).
We did not find a correlation between maternal TSI levels and the newborns' first thyroid function measurements, probably due to the small number of TSI measurements available. Nevertheless, we note that for three of the four neonates with overt hyperthyroidism, the TSI value during the pregnancy was available, and all had a TSI value above the reference range. The most severe case had a TSI level more than three times the upper limit of normal. This concurs with previous studies showing that the best predictor of fetal or neonatal thyrotoxicosis in pregnant women with Graves' disease is the presence of TRAb, which has been estimated to have a predictive value of 42% (4,37,38). Therefore, the most recent guidelines recommend measurement of TRAb at 20–24 weeks gestation (13). Orgiazzi suggested that when the TRAb level is significantly elevated during late pregnancy, TRAb should be determined in cord blood in the newborn (39). While cord blood TSH and fT4 levels cannot predict later hyperthyroidism, higher titers of TSI in cord blood have been shown to be associated with a greater risk of subsequent neonatal hyperthyroidism (21).
We found a negative association between fT4 level and weight gain during the first two weeks of life. Various studies have investigated the effects of abnormal maternal thyroid tests during pregnancy on birth weight (40 –44). A number of studies have shown a substantially increased risk of low birth weight in children born to hyperthyroid mothers (40 –42). Even maternal high-normal fT4 levels were recently associated with lower fetal weight (45). However, contrary to what might be expected based on this negative association, a positive association was found between cord fT4 levels and birth weight (45). Our data demonstrate that even a mild elevation of fT4 levels during the first two weeks of life may have an important impact on weight gain. Further studies are needed to elucidate the complex relations between maternal and newborn thyroid parameters and weight.
This study has some limitations. Due to the retrospective chart review design of the study, not all measurements were obtained on the same days. In addition, cord blood measurements were not drawn. While cord blood TSH and fT4 levels cannot predict later hyperthyroidism, higher titers of TSI in cord blood have been shown to be associated with a greater risk of subsequent neonatal hyperthyroidism (21). The strengths of our study are the large cohort and the longitudinal follow-up of up to three months.
In conclusion, we show that most neonates born to mothers with Graves' disease have abnormal fT4 and TSH levels that peak at day 5. Therefore, we recommend thyroid function tests be taken between postnatal days 3–5 to ensure early detection of hyperthyroidism. If the fT4 level is normal on day 14, and the neonate is asymptomatic, further blood tests are not needed. Finally, we found a negative association between fT4 level and weight gain during the first two weeks of life, indicating that even mildly increased fT4 levels can have important consequences for the newborn.
Footnotes
Acknowledgments
We thank Ms. Cindy Cohen for her editorial assistance and Mr. Yotam Hamiel for his graphic assistance.
Author Disclosure Statement
Authors declare that there are no conflicts of interest.