
Abstract
Background:
The prognostic implications of the diagnosis of a papillary thyroid carcinoma (PTC) with tall-cell features are unknown.
Methods:
All PTC patients identified between 1985 and 2005 were analyzed histologically. Classical PTC cases were defined as having <30% tall cells, PTC with tall-cell features (PTC TCF) as 30%–49% tall cells, and tall-cell variant of PTC (TCV) as ≥50% tall cells. All classical PTC, PTC TCF, and TCV ≥1 cm in size were included.
Results:
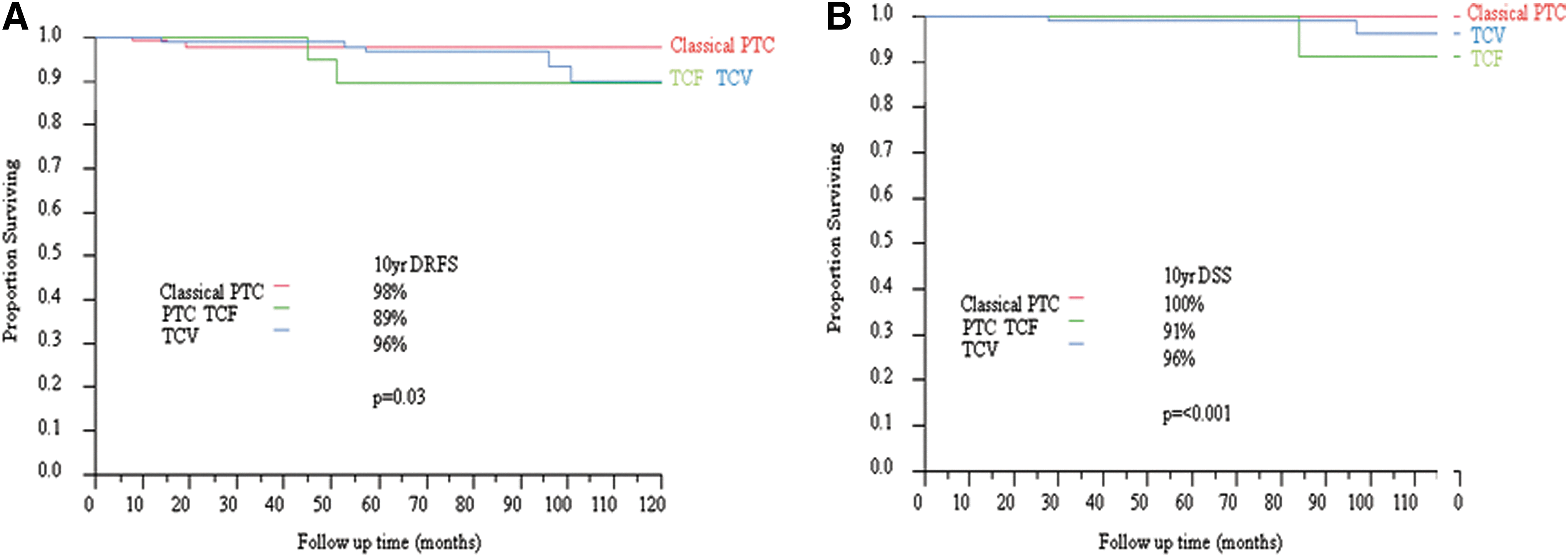
A total of 453 patients satisfied the inclusion criteria (288 classical PTC, 31 PTC TCF, and 134 TCV). Classical PTC patients were younger than their PTC TCF and TCV counterparts (p<0.0002). There was an increase in tumor size from classical PTC to PTC TCF and TCV (p=0.05). Extensive extrathyroid extension and positive margins were more often present in TCV and PTC TCF than in classical PTC (p=0.0001 and p=0.03 respectively). Overall pathologic tumor (pT) stage was more advanced in TCV and PTC TCF than in classical PTC (p<0.0001). Total thyroidectomy and radioactive iodine therapy were more often performed and administered in TCV patients than in their PTC TCF and classical PTC counterparts (p=0.001 and p=0.0001 respectively). Median follow-up was 9.3 years. Ten-year disease-specific survival (DSS) was lower in TCV (96%) and PTC TCF (91%) than in classical PTC (100%; p<0.001). Ten-year distant recurrence-free survival (RFS) was higher in classical PTC (98%) than in PTC TCF (89%) and TCV (96%; p=0.03). In multivariate analysis, the presence of more than five positive nodes and extranodal extension were the only independent prognostic factors of neck and distant RFS respectively. Four (2.4%) of 165 PTC TCF and PTC TCV developed poorly differentiated or anaplastic carcinoma in their recurrence, while none of the 288 classical PTC transformed into higher grades (p=0.017).
Conclusions:
PTC TCF and TCV have similar clinicopathologic features that are more aggressive than classical PTC. PTC TCF and TCV have similar DSS and distant RFS but poorer outcomes than classical PTC. PTC TCF are currently being treated like classical PTC, that is, less aggressively than TCV. PTC TCF and TCV TCV have a higher rates of high-grade transformation than classical PTC. Consideration should be given to using a 30% tall-cell threshold to diagnose TCV.
Introduction
T
The above controversies create therapeutic dilemmas and significant anxiety for patients and their physicians. In order to address these issues, we undertook a clinical and meticulous pathologic examination of a large cohort of classical PTC, TCV, and PTC TCF treated at our institution over a 20-year period.
Materials and Methods
Patient selection
The hospital database was searched for all cases diagnosed as PTC and treated at the Memorial Sloan-Kettering Cancer Center (MSKCC), New York, between 1985 and 2005. After subcentimeter tumors were excluded, all remaining PTC with adequate histologic slides were submitted to re-review by at least one of two head and neck pathologists with special expertise in thyroid neoplasia (R.G. and M.R.). The pathologists were blinded to the clinical outcome of all patients studied. The study was approved by the Institutional Review Board of MSKCC.
Tumor definition
The tumors were defined as follows:
TCV
A tumor was classified as TCV if it contained 50% or more tall cells without tumor necrosis or marked mitotic activity (≥5 mitoses/10 high-power fields, 400×). The tall cells were defined as cells with their height twice their width and having an eosinophilic cytoplasm with a low nuclear–cytoplasmic ratio and the characteristic nuclear features of PTC (i.e., irregular enlarged clear nuclei with grooves and pseudo-inclusions). The required percentage of tall cells and their height–width ratio matched the criteria used for the diagnosis of TCV by the Cancer Genome Atlas Project Working Group (TCGA).
PTC TCF
A tumor was defined as PTC TCF if it harbored between 30% and 50% tall cells (i.e., 30% to <50%). The tumor was not considered a PTC TCF if associated with tumor necrosis or marked mitotic activity (≥5 mitoses/10 high-power fields, 400×).
Classical PTC
A tumor was classified as classical PTC if it showed >1% papillary formations and was composed of cells having the characteristic nuclear features of papillary carcinoma. The classical cases had to contain <30% tall cells and be devoid of tumor necrosis or marked mitotic activity (≥5 mitoses/10 high-power fields, 400×).
Inclusion criteria
Tumors were included in the study if they fulfilled the above definitions and were ≥1 cm in size.
Histopathologic analysis
The largest dimension of the carcinoma was based on review of the gross pathology report and direct microscopic measurement of the tumor on the slides. The mitotic rate of the tumor was determined by counting 10 contiguous high-power fields (400×) using an Olympus microscope (U-DO model BX-40; Olympus America Inc., Melville, NY). Using that microscope type, these 10 high-power fields correspond to 2.4 mm2. Tumor necrosis was defined by a “comedo-like” appearance composed of degenerating cytoplasm and punctate, karyorrhectic nuclear debris. Vascular invasion was categorized as present or absent. Invasion of the tumor capsule defined as transcapsular penetration was recorded. ETE was defined as tumor cells invading beyond the thyroid capsule into perithyroid soft tissue or organs. ETE was subdivided into: (i) none; (ii) focal: presence of one or two microscopic foci of ETE measuring ≤1 mm each; (iii) extensive: presence of more than two microscopic foci of ETE (≤1 mm in size each) or any foci >1 mm in size. The type of perithyroid tissue or organ invaded by the tumor was recorded (e.g., adipose tissue, skeletal muscle, recurrent nerve, trachea, and esophagus). The status of the resection margins was reported as positive (tumor present at the surgical margin) or negative (no tumor at surgical margin). The number of lymph nodes examined microscopically, as well as the number of nodes with metastatic carcinoma, were recorded. On the basis of gross and microscopic examination of the surgical specimen by the pathologist, the greatest diameter of the largest metastatic node was measured, as well as the largest size of the largest metastatic tumor focus. A PTC was defined as transformed if it displayed foci of poorly differentiated or anaplastic thyroid carcinoma in the recurrence. Poorly differentiated carcinoma was defined as a tumor having follicular cell differentiation at the histological or immunohistochemical level with marked mitotic activity (≥5 mitoses/10 high-power fields, 400×) and/or tumor necrosis. Anaplastic carcinoma was defined as a tumor composed of undifferentiated tumor cells lacking follicular cell differentiation at the morphologic and immunohistochemical level.
Clinical parameters
The patient's electronic medical records were reviewed for the age at diagnosis, type of surgery, and adjuvant treatment including radioactive iodine (RAI) therapy. Staging was performed according to the AJCC Cancer Staging Manual 7th edition (8). In view of the fact that many cases from the 1980s did not have adequate biochemical data, the patient disease status at recurrence or follow-up was based on a combination of clinical and imaging assessments. These evaluations include history taking, physical examination, RAI scanning, cross-sectional imaging, and/or positron emission tomography (PET) scanning. Thus, biochemical recurrence was not assessed. The type of cervical lymph node dissection/biopsy was recorded as central, lateral, central and lateral, or other. The latter category consists solely of perithyroidal lymph nodes removed with the thyroid specimen or superior mediastinal lymph nodes. The date of initial surgery and last date of follow-up were documented. The status at last follow-up was recorded as follows: no evidence of disease; alive with disease; dead of other causes, and dead of disease (DOD).
Statistical analysis
Pearson's chi-square test was used to assess the relation between categorical variables. Survival probabilities were estimated by the Kaplan–Meier method and compared using the log-rank test. A p-value≤0.05 was considered as significant. Recurrence free survival (RFS) was defined as the time interval between the date of initial surgery and date of first recurrence. Disease-specific survival (DSS) was calculated from the date of initial surgery to last follow-up. DSS status was defined as the presence or absence of DOD at last follow-up. Multivariate analysis was performed using a Cox regression model and log-rank statistics. Statistical analysis was carried out using JMP statistical package (SAS Institute Inc., Cary, NC) and SPSS version 19.0 (IBM Corp., Chicago, IL).
Results
Clinicopathologic features according to the subtype of PTC
Table 1 displays the clinicopathologic features of the tumor according to the subtype of PTC. Patients with classical PTC are younger, have smaller tumor size, lower stage, less positive margins, and less extensive ETE than those with TCV and PTC TCF (p≤0.05). There were no differences between TCV and PTC TCF in regard to the above parameters. In contrast, TCV were more often treated with total thyroidectomy, RAI therapy, and lymphadenectomy than the cohort of patients with classical PTC and PTC TCF (p≤0.05). There were no differences in treatment modalities between those who harbored classical PTC and those with PTC TCF.
In this calculation, pT4 was compared to pT 1–3.
TNM staging as per Edge et al. (8).
Analysis compared extensive to focal/no extrathyroid extension.
The analysis compared the presence to absence of lymphadenectomy.
In three cases, RAI therapy status was not available.
PTC, papillary thyroid carcinoma; RAI, radioactive iodine; TCF, PTC with tall-cell features; TCV, tall-cell variant PTC.
TCV/PTC TCF vs. Classical PTC.
Classical PTC/PTC TCF vs. TCV.
PTC, papillary thyroid carcinoma; RAI, radioactive iodine; PTC TCF, PTC with tall-cell features; TCV, tall-cell variant of PTC.
Anaplastic and poorly differentiated carcinoma transformation in the recurrence sites
Four (2.4%) out of a group of 165 patients with PTC TCF and TCV developed poorly differentiated or anaplastic carcinoma in their recurrence. In contrast, none of the 288 classical PTC transformed into poorly differentiated or anaplastic carcinoma (p=0.017). Three PTC TCF cases harbored anaplastic (n=2) and poorly differentiated carcinoma (n=1) in their recurrence sites. One TCV case relapsed as anaplastic carcinoma.
Outcome of the whole patient population
The median follow-up was 112 months (range 4–291 months). The 10-year DSS was 98% with only six patients DOD. Overall, 45 patients recurred with a RFS of 84% at 10 years. Forty-one patients recurred in the neck, and 13 at distant sites with a 10-year neck RFS of 86% and a 10-year distant RFS of 95%.
Prognostic factors of recurrence-free survival
Tables 2 and 3 list the variables affecting neck and distant RFS respectively. Male sex, extensive ETE, the presence of positive nodes, a high number of nodal metastasis, and a large size metastatic node (>1 cm) conferred worse neck RFS (p≤0.05). The subtype of PTC did not influence neck RFS. In contrast, patients with TCV and PTC TCF had a poorer distant RFS in comparison to those with classical PTC (p=0.03; Fig. 1A). Other factors predicting worse distant RFS were pT4 tumor, positive margins, extensive ETE, a high number of nodal metastasis, a large size metastatic node (>1 cm), and extranodal extension (p≤0.05). In multivariate analysis (Table 4), the presence of more than five positive nodes and extranodal extension were the only independent prognostic factors of neck and distant RFS respectively.
TNM staging as per Edge et al. (8).
In three cases, RAI therapy status was not available.
Extensive vs. focal/none.
NRFS, neck recurrence-free survival.
TNM staging as per Edge et al. (8).
In three cases, RAI therapy status was not available.
TCV/PTC TCF vs. Classical PTC.
pT4 vs pT1–3.
Extensive vs. focal/none.
DRFS, distant recurrence–free survival.
Prognostic factors of DSS
Table 5 lists the variables affecting DSS. Older age patients, those with pT4 tumor, positive margins, or extranodal extension had worse 10-year DSS (p≤0.05). Individuals with TCV and PTC TCF had a higher risk of dying from thyroid carcinoma than those with classical PTC (p<0.001; Fig. 1B). It was not possible to perform multivariate analysis for DSS, since only six patients died of disease.
TNM staging as per Edge et al. (8).
In three cases, RAI therapy status was not available.
TCV/PTC TCF vs. Classical PTC.
pT4 vs. pT1–3.
Clinicopathologic characteristics of patients who died of disease
Table 6 shows the clinicopathologic characteristics of the six patients who died of thyroid carcinomas. All patients had nodal metastasis at presentation. Five (83%) of the six patients harbored TCV or PTC TCF in the primary tumor. In four (67%) of six patients, the tumor transformed to a higher grade (anaplastic or poorly differentiated thyroid carcinomas) in the recurrence site (Fig. 2).
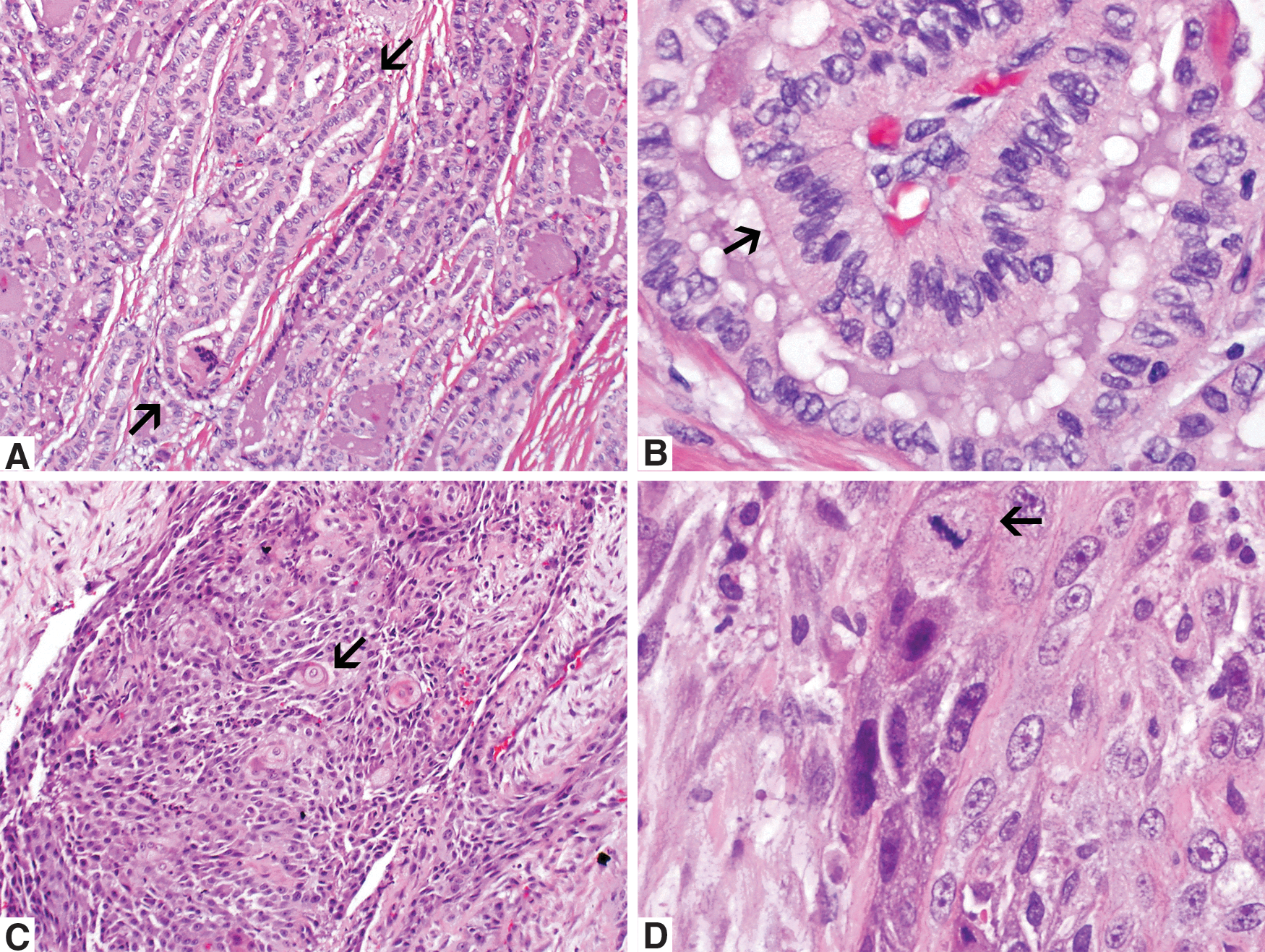
A 64-year-old female with PTC TCF that transformed as anaplastic carcinoma in the pleura seven years after diagnosis and resulted in death.
TNM staging as per Edge et al. (8).Ca, carcinoma.
Discussion
In the current series, patients with TCV presented at an older age and higher stage than their classical PTC counterparts. This is in agreement with the large amount of literature on the subject (1
–4,9
–14). Similar to patients with TCV, those with PTC TCF were significantly older and harbored more aggressive tumor features (e.g., higher stage, extensive ETE) than patients with classical PTC. There was no difference in lymph node positivity rate between the three subtypes of PTC. This is in disagreement with some publications that demonstrated a higher rate of nodal metastases in the TCV (2,4)
One of the most interesting findings in this study is a higher proportion of transformation to anaplastic and poorly differentiated thyroid carcinomas in the TCV and PTC TCF groups. Four of 165 (2.4%) TCV and PTC TCF transformed to these higher-grade tumors when compared to none of 288 classical PTC (p=0.017). This is another example of the higher aggressive biological behavior of TCV, as well as PTC TCF, and should prompt the pathologist to sample these tumors generously for microscopic examination in search of an anaplastic or poorly differentiated component, especially in older patients. Indeed, all the transformed cases occurred in individuals who were over the age of 50 years. Many molecular factors have been incriminated as responsible for the aggressive behavior of TCV. MUC1 was often shown to be amplified at the DNA level and overexpressed at the transcript and protein levels in TCV (15). In a previous study, we detected MUC1 by immunostaining in a significantly higher proportion of TCV than classical PTC (15). The overexpression of this transmembrane epithelial cell surface glycoprotein in many carcinomas interferes with integrin-mediated adhesion to the extracellular matrix and with cadherin-mediated cell–cell adhesion. This could lead to cellular dissociation and oncogenic progression (16,17) contributing to the biologic behavior of TCV. The 72-kd type IV collagenase (matrix metalloproteinase-2; MMP-2) was shown to be overexpressed in TCV compared to a group of classical, follicular variant, and microcarcinoma PTC (18). This neutral metalloproteinase initiates the degradation of type IV collagen in basement membranes. Its production by tumor cells has been correlated with invasion and metastasis. The aggressive behavior of TCV may also be related to a higher prevalence of BRAF V600E point mutations in TCV when compared to classical PTC (19). Finally, c-MET was shown to have a higher rate of overexpression by immunostaining in TCV than in classical PTC (20). The proto-oncogene cMET encodes the tyrosine kinase receptor for hepatocyte growth factor/scatter factor, and its overexpression is speculated to result in increased motility and invasiveness in PTC (21). The Thyroid Cancer Genome Atlas (TCGA) program is now undertaking the comprehensive genotyping of 500 PTC using various platforms (e.g., exome sequencing, expression arrays, gene methylation, and microRNA arrays). Many TCV are included in this analysis, and their histologic definition (≥50% of tumor cells) is similar to the one used in this study. This deep sequencing study will help to characterize the molecular profile of TCV better.
One of the most important controversies in the assessment of PTC relates to the independent prognostic value of a diagnosis of TCV. This has practical implications, since there seems to be a recent increase in the number of TCV diagnosed at a lower stage in young patients. While some authors believe that TCV is more aggressive than classical PTC only because of its higher stage and older age at presentation (4), others consider it as an independent prognostic factor of outcome (5,6,13,22). In the current study, PTC subtype was not an independent predictor of RFS. The disparate results between several publications could be related to the definition utilized for the diagnosis of the TCV and to the presence or absence of a meticulous histologic analysis. In our study, we excluded all tumors with high mitotic activity and/or tumor necrosis, while a matched paired analysis using the Surveillance, Epidemiology, and End Results (SEER) database could not control for these pathologic variables, since no re-review of the histologic slides is possible with SEER cases (22). In the latter study, the presence of high-grade TCV tumors could have imparted an independent prognostic value to the diagnosis of TCV. In that regard, Akslen and Livolsi found a higher frequency of tumor necrosis in TCV compared to other subtypes of PTC (7). Furthermore, they found that the histologic grade (defined as nuclear atypia, tumor necrosis, and vascular invasion) and tumor size, rather than PTC subtype, were independent prognostic factors (7). Multivariate analysis could not be performed for DSS, since only six patients died of thyroid carcinoma. This low death rate could also be attributed to the absence of PTC with high-grade proliferative features in our patient cohort. Alternatively, the discrepant results between investigators could be simply related to variation in sample size and outcome measures. In a previous publication on TCV and classical PTC without ETE, we found that there was a higher but not statistically significant rate of recurrence and distant metastasis in TCV than in classical PTC using histological definitions similar to the one utilized in the current study (23). However, in contrast to the current investigation, the sample size was much smaller, and recurrence was assessed using not only clinical but also biochemical parameters. Clearly, there is a need for larger studies on the subject with re-review of the histology slides, and clear definitions of PTC subtypes and outcome measures. Because of these controversial data regarding the independent prognostic value of TCV and PTC TCF and their lack of independent predictive power for clinical recurrence in that study, we recommend at the present time refraining from aggressive treatment in low-stage TCV and PTC TCF that do not display any worrisome features (i.e., high mitotic rate, tumor necrosis, angioinvasion, cervical node involvement, and ETE).
In conclusion, this study confirms the aggressive nature of TCV as a group of tumors compared to classical PTC. It also shows that PTC TCF behave like TCV. However, they are currently treated like classical PTC. Therefore, PTC TCF should be considered as TCV, and the threshold for the diagnosis of TCV should be lowered to 30% of tall cells in the tumor. The independent prognostic value of TCV and PTC TCF at least in regard to RFS is still subject to debate. TCV as well as PTC TCF have a higher risk of transformation to higher-grade tumors. This should prompt generous tissue sampling of these carcinomas in search for anaplastic and poorly differentiated foci, especially in patients over 50 years old.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.