
Abstract
Background:
Papillary thyroid cancer occasionally occurs in women of childbearing age. As papillary thyroid microcarcinoma (PTMC) rarely grows or becomes clinically apparent, observation without surgery is an appropriate strategy for patients with low-risk PTMC. Human chorionic gonadotropin possesses weak thyroid-stimulating activity. The aim of this study was to assess the effect of pregnancy on PTMC.
Methods:
We studied 9 patients with PTMC who became pregnant between 2005 and 2011. Twenty-seven age-matched nonpregnant female PTMC patients from a database we used in our previous report served as controls. Tumor enlargement was defined as an increase in the diameter of the tumor of 3 mm or more.
Results:
PTMC enlargement occurred in 44.4% (4/9 patients) of the pregnant subjects, whereas it occurred only in 11.1% (3/27 patients) of the controls (p=0.0497). Three of the pregnant patients who exhibited tumor enlargement underwent surgery after delivery. No relationship was detected between the changes in the serum thyroglobulin level, the serum thyrotropin level, and tumor size during pregnancy. Immunohistochemical examinations did not detect the estrogen receptor in the tumors of the three patients who underwent surgery.
Conclusions:
This study is an initial report indicating that the risk of PTMC enlargement might increase during pregnancy. PTMC should be carefully followed-up for possible disease aggravation during pregnancy. Even if a PTMC enlarges during pregnancy, the patient's prognosis will probably not worsen.
Introduction
P
The World Health Organization defined papillary thyroid microcarcinoma (PTMC) as a small PTC of less than 10 mm in diameter (3). In 1993, we initiated an observation trial of incidentally detected PTMC at Kuma Hospital (4). Between 1993 and 2004, 340 patients with PTMC underwent observation. The length of the observation period ranged from 18 to 187 months (mean 74 months). In patients who preferred observation to surgical treatment, we measured the size of the tumor and assessed their regional nodal status by ultrasonography once or twice a year. After follow-up periods of 5 and 10 years, 6.4% and 15.9%, respectively, of the patients had PTMC that had enlarged by 3 mm or more (5). In another report, 22 of 300 PTMCs (7%) had increased in size after 1–17 years of observation (6). On the basis of these Japanese reports, observation without surgery was accepted as an appropriate strategy for patients with low-risk PTMC in the guidelines for the management of thyroid tumors developed by the Japanese Society of Thyroid Surgeons and the Japanese Association of Endocrine Surgeons (1).
Pregnancy has a profound impact on the thyroid gland and thyroid function. Human chorionic gonadotropin (hCG) is a member of a family of glycoprotein hormones, which also includes thyrotropin (TSH), that share a common alpha-subunit but possess unique beta-subunits. There is considerable homology between the beta-subunits of hCG and TSH. As a result, hCG exhibits weak thyroid-stimulating activity (7). Some reports have suggested the importance of growth factors (mainly TSH, but also hCG) for the growth, progression, and spread of papillary tumors (8). Kimura et al. also showed that in normal early pregnancy, the thyroid gland is physiologically activated by serum hCG, which possesses intrinsic thyroid-stimulating activity (9). Therefore, it is plausible that pregnancy could promote the onset of the growth of benign or malignant nodules via pregnancy-induced iodine deficiency, the thyroid-stimulating effect of hCG, and/or high estrogen levels (9).
The American Thyroid Association treatment guidelines recommend that nodules whose cytological findings are indicative of PTC and that are discovered early in pregnancy should be monitored sonographically. If they grow substantially by 24 weeks of gestation (i.e., by 50% in volume or 20% in diameter in two dimensions), surgery should be performed (10,11). In addition, the Endocrine Society's clinical practice guidelines state that fine-needle aspiration cytology should be performed for thyroid nodules discovered during pregnancy that are predominantly solid and larger than 1 cm in diameter (12). However, even these guidelines do not discuss the management of PTMC during pregnancy. In a previous systematic review, it was found that thyroid cancer that is discovered during pregnancy does not have a significant prognostic impact (13). However, there are no reports about the observation of PTMC during pregnancy. In the present study, we demonstrate the effect of pregnancy on PTMC.
Patients and Methods
Patients
This study is a retrospective study of all the women who were being observed at Kuma Hospital for PTMC and who subsequently became pregnant between 2005 and 2011. Patients whose tumors were not measured before pregnancy and/or after delivery were excluded. As a result, 9 patients who ranged in age from 25 to 36 years (mean age 30.7 years) were included in this study. We extracted the control group from a database of observed PTMC patients that we had used in a previous study. Between 1993 and 2004, 340 patients with PTMC underwent observation. Twenty-seven age-matched (25–36 years old) nonpregnant female patients were selected from this population and used as the control group. The controls ranged in age from 26 to 36 years (mean age 31.0 years). The length of the follow-up period did not differ between the pregnant and control groups. The increase in tumor size was defined as the change in the maximum diameter of the tumor on ultrasonography images. Tumor enlargement was defined as an increase in the tumor diameter of 3 mm or more. In this study, we defined the pregnant period as follows: first trimester (pregnancy <15 weeks), second trimester (<29 weeks), third trimester (≥29 weeks), and the postdelivery period (<6 months after delivery).
Statistical analysis
The significance of the differences in the examined variables among the groups was calculated using the chi-square test, Fisher's exact test, or the independent t-test. All statistical tests were two-sided, with the level of significance set at p<0.05.
Results
Enlargement of PTMC during pregnancy
No difference in tumor size at the initial diagnosis was detected between the groups. In the pregnant group, the mean tumor size at the last examination was larger than that seen in the control group, but the difference was not significant (p=0.058) (Table 1). PTMC enlargement of 3 mm or more was detected in 4 (44.4%) of the 9 pregnant patients, whereas it was observed only in 3 (11.1%) of the 27 patients in the control group. The difference between the two groups was significant (Fisher's exact test, p=0.0497). Figure 1A shows the change in tumor size in the patients whose tumors enlarged by 3 mm or more during pregnancy. Three patients underwent surgical treatment after delivery because of tumor enlargement. As for the remaining patient, her tumor enlarged by 3 mm during pregnancy; however, we continued observing it because it reduced in size after delivery. Figure 1B shows the serial changes in tumor size in the 5 patients whose tumors enlarged by less than 3 mm during pregnancy. Among these PTMCs, three tumors slightly decreased in size after delivery, supporting the hypothesis that PTMCs enlarge during pregnancy.

The changes in tumor size observed in the patients whose papillary microcarcinomas enlarged
Changes in serum thyroglobulin and TSH levels during pregnancy
Of the nine pregnant patients, test results for thyroglobulin (Tg) antibody were negative in six. We were able to measure the serum Tg concentration before, during, and after pregnancy in four of the patients who had negative Tg antibody results. In one of the four patients, the tumor increased in size by more than 3 mm during pregnancy, and the patient's serum Tg levels also increased (Fig. 2, solid line); however, they displayed lower serum Tg levels than the other three patients. Figure 3A shows the changes in the serum TSH level observed in the 4 patients whose tumors enlarged by 3 mm or more during pregnancy. Figure 3B shows the changes in the serum TSH level observed in the 5 patients whose tumors enlarged by less than 3 mm during pregnancy. Two patients received levothyroxine treatment while they were pregnant. No relationship between tumor growth and the serum TSH level was found.
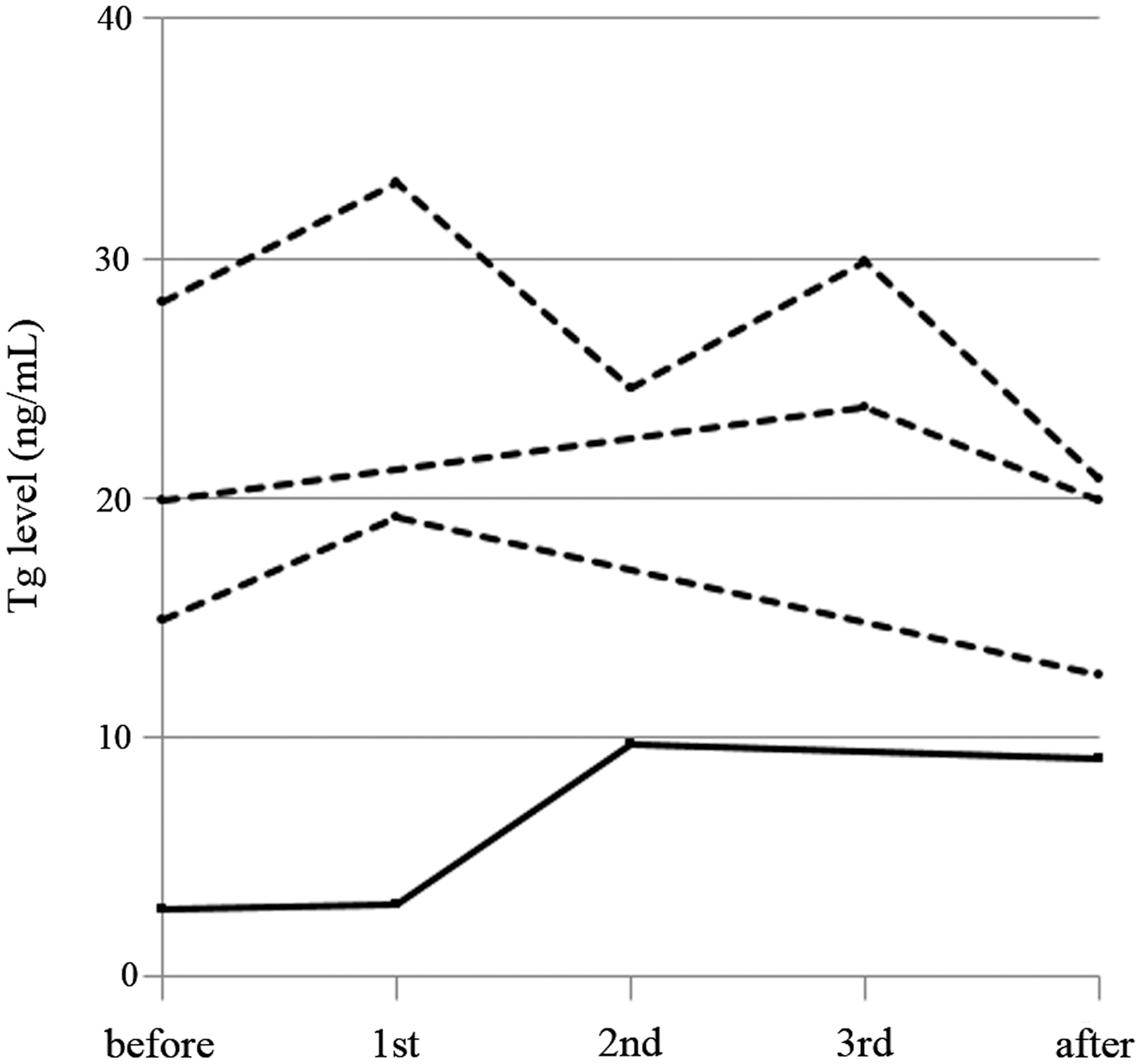
The change in the serum Tg level during pregnancy in the Tg antibody-negative cases. Solid line, surgically treated cases; dashed line, observed cases. Tg, thyroglobulin.
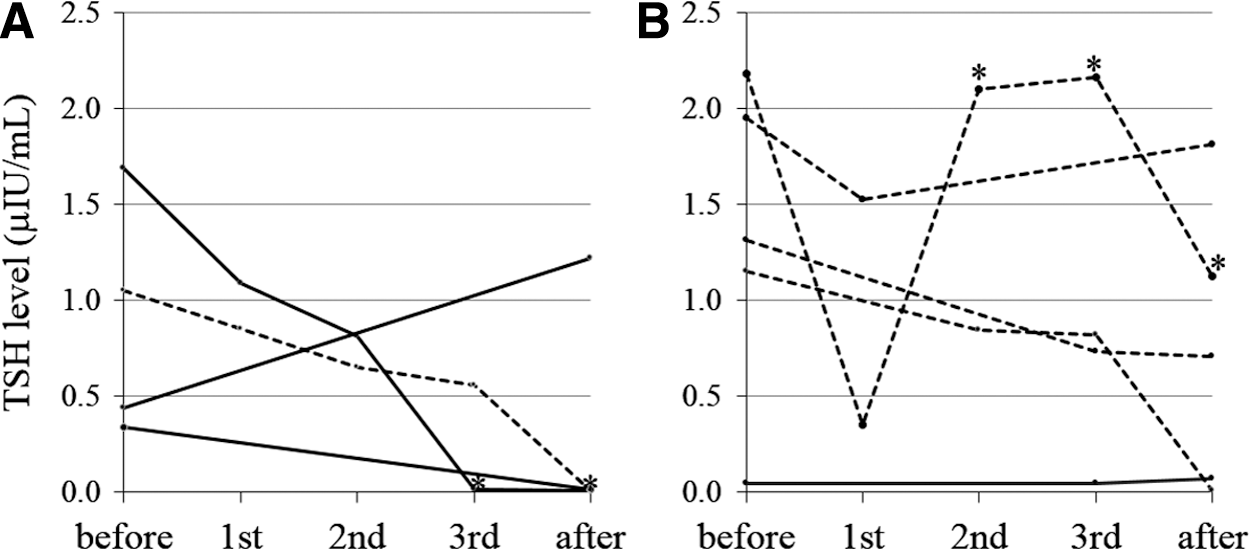
The changes in the TSH level observed in the patients whose papillary microcarcinomas enlarged
Pathological diagnosis in the cases in which the PTMC enlarged during pregnancy
No extrathyroidal invasion was detected in the three patients who underwent surgery. Pretracheal and paratracheal lymph node metastases developed in one case. Immunohistochemical examinations of estrogen receptor (ER) expression did not detect the ER in any of the three surgically excised tumors. In addition, none of the patients in either group suffered tumor recurrence or died of their disease.
Discussion
This study is an initial report suggesting that PTMCs enlarge during pregnancy. The Japanese treatment guidelines for such tumors state that surgical treatment is mandatory for PTMC patients who exhibit clinical lymph node metastasis on palpation or imaging studies, distant metastasis, or significant extrathyroidal extension. Patients without these features are candidates for observation, provided that the situation has been fully explained to them and their informed consent has been obtained (1). Male sex, multicentricity, and advanced age are prognostic factors for papillary carcinoma, but these features do not affect the risk of PTMC progression during observation. Furthermore, no relationship between PTMC enlargement and tumor size at diagnosis has been demonstrated (5). Recently, a report by Ito et al. suggested that PTMC might be more progressive in young patients than in older patients (14). Therefore, we used age-matched patients as the control group. The findings of the present study suggest that pregnancy is a risk factor for PTMC enlargement. However, no relationship was detected between tumor size at diagnosis and tumor enlargement during pregnancy.
Regarding the progression of microcarcinoma, at least three factors should be considered: (i) tumor-stimulating factors, (ii) the biological nature of the carcinoma cells involved, and (iii) the suppression of immune surveillance. It is evident that the elevated hCG levels present during pregnancy stimulate the thyroid gland. Therefore, we consider that tumor enlargement might be facilitated by the weak thyroid-stimulating activity of hCG (7 –9). Several previous reports have suggested that thyroid cancer is aggravated during pregnancy. For women without persistent disease, pregnancy itself has not been shown to increase the risk of cancer recurrence (15 –17). However, in women with persistent disease (structural or biochemical) disease progression can occur during pregnancy (15,16). There is little published data comparing the outcomes of pregnant and nonpregnant PTC patients (13). The American Thyroid Association treatment guidelines for thyroid disease during pregnancy and the postpartum period (10) state that surgery for differentiated thyroid cancer can be postponed until the postpartum period without impacting on the risk of tumor recurrence or mortality. This approach can also be applied to microcarcinomas; thus, in the three cases in the present study in which surgery was deemed necessary, the procedures were postponed until the postpartum period. TSH suppression combined with observation might be an effective strategy for preventing PTMC progression (14). In this study, no correlation between tumor growth and the serum TSH level was found. Differences in the distribution and expression patterns of the ER, as well as variations in the ERα:ERβ ratio might play a role in thyroid cancer cell proliferation, as well as in the outcome of thyroid cancer (18). We were not able to identify the clinical features of the cases in which tumor enlargement occurred. In three patients, we decided to operate because of tumor enlargement, but the ER was not expressed by these patients' tumors.
In human thyroid cancer, both the humoral and cellular immune systems provide important protection against tumor progression (19). Active immunization (19) and dendritic cell vaccination (20) have been reported to be partially effective at inhibiting the growth of thyroid papillary carcinoma. During pregnancy, both Th1 and Th2 immune reactions are suppressed to prevent fetus rejection (21,22); therefore, the suppression of immune surveillance might influence the clinical course of PTMC growth. It is necessary to clarify this because most PTMCs remain inactive during pregnancy.
In conclusion, PTMC should be carefully followed-up for possible disease aggravation during pregnancy. Even if a PTMC enlarges during pregnancy, the patient's prognosis will probably not worsen.
Footnotes
Author Disclosure Statement
No competing financial interests exist.