
Abstract
Background:
Patients with subclinical hypothyroidism (SCH) have lower exercise tolerance, but the impact on oxygen uptake (VO2) kinetics is unknown. This study evaluated VO2 kinetics during and after a constant load submaximal exercise in SCH.
Methods:
The study included 19 women with SCH (thyrotropin (TSH)=6.87±2.88 μIU/mL, free thyroxine (fT4)=0.97±0.15 ng/dL) and 19 controls (TSH=2.29±0.86 μIU/mL, T4=0.99±0.11 ng/dL) aged between 20 and 55 years. Ergospirometry exercise testing was performed for six minutes with a constant load of 50 W, followed by six minutes of passive recovery. The VO2 kinetics was quantified by the mean response time (MRT), which is the exponential time constant and approximates the time needed to reach 63% of change in VO2 (ΔVO2). The O2 deficit—energy supplied by anaerobic metabolism at the onset of exercise—and O2 debit—extra energy demand during the recovery period—were calculated by the formula MRT×ΔVO2. Values are mean±standard deviation.
Results:
In the rest-exercise transition, patients with SCH showed slower VO2 kinetics (MRT=47±8 sec vs. 40±6 sec, p=0.004) and a higher oxygen deficit (580±102 mL vs. 477±95 mL, p=0.003) than controls respectively. In the exercise-recovery transition, patients with SCH also showed slower VO2 kinetics (MRT=54±6 sec vs. 44±6 sec, p=0.001) and a higher oxygen debit (679±105 mL vs. 572±104 mL, p=0.003). The VO2 kinetics showed a significant correlation with TSH (p<0.05).
Conclusions:
This study demonstrates that women with SCH have the slowest VO2 kinetics in the onset and recovery of a constant-load submaximal exercise and highlights that this impairment is already manifest in the early stage of the disease.
Introduction
S
Lower exercise tolerance is an outstanding SCH characteristic. During maximal and submaximal exercises, patients with SCH showed lower efficiency of cardiopulmonary response to effort (3,6 –8). Results are conflicting during recovery (6,7,9). However, the pulmonary oxygen uptake (VO2) kinetics of patients with SCH during rest-exercise (phase-on) and exercise-recovery (phase-off) transitions are not known.
At the onset of exercise (the first 20 sec), there was a rapid increase in VO2 influenced predominantly by increased cardiac output and pulmonary blood flow (cardiodynamic phase 1), followed by an exponential increase in VO2 to the steady state, which reflects muscular VO2 kinetics (exponential phase 2) (10). According to previous studies, the on and off VO2 kinetics for submaximal exercise are well characterized by a mono-exponential equation (11 –13). The ratio that VO2 reaches the steady state is characterized by a mean response time (MRT), which is the exponential time constant of the increased VO2 and represents the time required to reach 63% steady state VO2 (14).
The VO2 kinetics is considered a marker of exercise tolerance, a standard evaluation tool in athletes, normal subjects and patients (15), and has greater prognostic value compared to VO2max (16). Slower VO2 kinetics are associated with greater use of intramuscular phosphocreatine, increased glycolytic activity and lactate production, greater O2 deficit, and early fatigue (17). Moreover, slowed VO2 kinetics are associated with increased cardiovascular dysfunction (18,19) and risk of mortality (16). VO2 kinetic values in healthy individuals range from 20 to 35 sec, while they may exceed 70 sec in cardiovascular and metabolic diseases (10).
In thyroid disorders, there is evidence of impaired VO2 kinetics in patients with hyperthyroidism (20) but not in SCH. Studying VO2 kinetics in SCH may contribute to the understanding of factors related to poor exercise tolerance observed in these patients. Furthermore, identifying factors that influence the adaptation and recovery from exercise is one of the first steps for prescribing optimal training programs to improve physical fitness. Therefore, the aim of this study was to test the hypothesis that the VO2 kinetics of women with SCH during and after submaximal exercise with constant load are slower than those of women without thyroid dysfunction.
Methods
Subjects
A total of 38 women aged between 20 and 55 years participated in this study: 19 with SCH and 19 controls without thyroid impairment, with similar characteristics regarding age, body mass, physical activity, and menopause status. Sample size calculation was performed for comparison of a continuous variable (VO2 kinetics) of two independent samples considering 95% confidence, 80% power, and an effect size of 0.88 (21). The volunteers were recruited in the Department of Endocrinology, Maternity Hospital Therezinha de Jesus, School of Medical Sciences and Health of Juiz de Fora. Inclusion criteria for the SCH group were women aged between 20 and 60 years, two TSH values (with a minimum interval of four weeks) above the upper limit of the reference range (0.35–4.94 μIU/mL) and a fT4 level within the reference range (0.70–1.48 ng/dL). Inclusion criteria for the control group were women aged between 20 and 60 years, TSH and fT4 within the reference range, no history of thyroid disease, and negative antithyroid antibodies. Exclusion criteria for both groups were a TSH >15 μIU/mL; use of tobacco and/or drugs or substances that could interfere with thyroid function, heart rate, blood pressure, or VO2 kinetics; known cardiopulmonary or metabolic disease; and inability to perform physical exercise. This research was conducted in agreement with the guidelines and policies of the institutional ethics committee (protocol no. 0164/10), and all participants signed an informed consent form.
Procedure
The volunteers were evaluated over five visits performed on different days. The elapsed time to perform all evaluations ranged from 8 to 12 days. The first visit was in the Service of Endocrinology to conduct clinical examinations and questionnaires. Blood collection and echocardiography were performed at the second and the third visits. The fourth visit was in the Motor Evaluation Laboratory, Faculty of Physical Education and Sports, Federal University of Juiz de Fora to perform the anthropometric evaluation and two constant-load ergospirometry exercise tests (50 W) on a bicycle to obtain the VO2 kinetics. On the last visit, the volunteers performed the third constant load testing, followed by a progressive submaximal testing with an initial load of 50 W and an increase of 10 W/min up to 85% of the maximal heart rate (HRmax). From the progressive testing, VO2max was estimated through VO2 extrapolation by HRmax estimated for age.
Hormonal measures, symptoms of hypothyroidism, physical activity level, and anthropometrics
The blood testing to measure hormonal levels (fT4 and TSH) and antithyroid antibodies was performed by third-generation chemiluminescence immunometric assays (Beckman Coulter ®, Access2®). The specific signs and symptoms of hypothyroidism were evaluated by the Billewicz scale modified by Zulewski et al. (22). The level of physical activity was assessed by the Baecke Questionnaire using its validated and translated version in Portuguese (23). Weight and height were measured during the anthropometric evaluation.
Echocardiographic measures
The echocardiogram was carried out to evaluate cardiac structure and function (Sonos 5500, Hewlett-Packard) using techniques of one- and two-dimensional echocardiography, and pulsed and continuous Doppler color flow mapping. The anatomical and functional data were obtained at rest using a 3.5 MHz linear array transducer placed in the third or fourth left intercostal spaces. The measurements were obtained and analyzed according to standards of the American Society of Echocardiography (24). The cardiac structure (atrium and systolic and diastolic diameters of the left ventricle), systolic function (systolic volume and ejection fraction), and diastolic function (deceleration time of the E wave and isovolumic relaxation time) were evaluated. All readings were made by a single cardiologist who was unaware of the thyroid status of the participant.
Ergospirometry testing
For the ergospirometry testing, volunteers were asked not to perform any strenuous physical activity and to abstain from consuming alcohol or caffeine on the day or the night before the test. Prior to testing, subjects were familiarized with the laboratory environment, the ergometry cycle, and the ergospirometry equipment. The expired fractions of oxygen and carbon dioxide and ventilation were assessed using a computerized online system with breath-by-breath measurement (K4 b2, Cosmed®). Before each testing, the equipment was calibrated with a gas cylinder containing known concentrations of gases. Tests were performed in the laboratory, always at the same time of the day, with a temperature between 20°C and 25°C, and a relative humidity between 45% and 60%. HR was monitored continuously at rest and during testing through a HR monitor (Polar). The oxygen pulse (VO2/HR) was calculated at the end of the sixth minute of exercise. Systolic (SBP) and diastolic (DBP) blood pressures were measured at rest, every three minutes of the exercise period, and during recovery using the auscultation method (Narcosul, 1400-C). The gas exchange threshold was determined by the V-slope method on the K4b2 software equipment (Cosmed®). The perceived exertion was assessed every three minutes in the constant load testing and every minute in the progressive load testing using the CR-10 Borg scale.
Submaximal exercise testing with constant load
The exercise test was carried out on an electromagnetic ergometer bicycle under constant load. The protocol consisted of three minutes at rest sitting on the bicycle, six minutes of exercise with a load of 50 W, while maintaining a rate of 60 rpm, followed by six minutes of passive recovery. On the first visit to the laboratory, after the volunteer had been familiarized with the equipment, two rest-exercise transitions were performed, separated by a rest period that were sufficient to allow a return to the pre-exercise VO2 and HR values. The third transition was performed on a different day, prior to the progressive testing. A recent study showed that VO2 kinetics are not affected by the sequence of data collection for loads below the anaerobic threshold, and the best estimate is the average result of at least three tests (25). The absolute load of 50 W was chosen based on previous studies (11,26 –28) and by representing similar intensity to most daily voluntary activities.
Measurement of VO2 kinetics
The analyses of VO2 kinetics of constant load testing were performed on the K4b2 software equipment (Cosmed®). A mono-exponential model was used from the exercise onset and recovery (t=0 sec) using nonlinear regression and the least squares method. To reduce the presence of noise, a smoothing procedure was used in breath-by-breath data, through averaging every five breaths (11,27 –30).
To calculate the time constants, equations 1 and 2 were used:
VO2(t) represents the VO2 at any time, VO2b indicates the VO2 immediately before the exercise onset, VO2ss is VO2 steady state at the end of the sixth minute of exercise, ΔVO2 is the amplitude of VO2 variation during the exercise and recovery, τ is the time constant of VO2 response, and Td is the time delay in the VO2 response. The quantification of VO2 kinetics was performed by MRT, comprising the phases 1 and 2 (MRT=Td+τ), using the mean of the three transitions (25,31 –33). The O2 deficit and O2 debit were calculated by the formula MRT×ΔVO2 (14). The mono-exponential modeling proved adequate for data of both the SCH and control groups (VO2 on-kinetics: R 2=0.85±0.09 vs. 0.88±0.06; VO2 off-kinetics: R 2=0.91±0.05 vs. 0.92±0.04 respectively). Significant intragroup correlation coefficients were observed for VO2 on-kinetics (r=0.83 [CI 0.71–0.91], p=0.001) and VO2 off-kinetics (r=0.82 [CI 0.69–0.90], p=0.001), confirming the reproducibility of the measurement already observed in other studies (11,25).
Statistical analysis
All data are presented as mean±standard deviation. Normality and equality of variance were confirmed by the Kolmogorov–Smirnov and the Levene tests respectively. The independent samples t-test was used to test for differences in continuous variables between groups. Paired t-tests were used to determine the symmetry between VO2 on- and off-kinetics within groups. The effect size (ES) was calculated by Cohen's d. Pearson's product–moment and partial correlation coefficients were used to test relationship between continuous variables. All statistical analyses were conducted using SPSS v19 (IBM Corp., Armonk, NY). Statistical significance was accepted when p<0.05.
Results
Women with SCH had higher TSH and higher symptoms of hypothyroidism than the control group (3.47±1.65 vs. 2.47±0.96 points respectively; p=0.03). Both groups were similar in fT4, age, weight, height, body mass index, physical activity, and HR at rest (p>0.05). Women with SCH had higher DBP (p=0.05) and slightly higher SBP than controls (p=0.08). During constant load exercise, there was no significant difference in the hemodynamic response (HR, SBP, and DBP), perceived exertion, and O2 pulse between groups (p>0.05). During submaximal progressive testing, no significant differences were observed at the anaerobic threshold, VO2max estimation, and efficiency of oxygen uptake (Table 1).
Note. Values are mean±standard deviation. Physical activity measured by the Baecke's questionnaire (3–14.75 points). Perceived exertion: Borg scale (0–10 points).
Women with SCH differ from controls (p<0.05).
SCH, subclinical hypothyroidism; BMI, body mass index; TSH, serum thyrotropin; fT4, free thyroxine; HR, heart rate; SBP, systolic blood pressure; DBP, diastolic blood pressure; VT, ventilatory threshold; VO2, oxygen uptake; ΔVO2/ΔW slope, oxygen uptake efficiency slope; VO2max, estimated maximal oxygen uptake.
All VO2 kinetic parameters obtained during on and off transitions of both groups are shown in Table 2. At the onset of exercise, no significant differences were observed between the groups at baseline VO2, ΔVO2, and steady-state VO2 (p>0.05). However, patients with SCH had a higher O2 deficit (p=0.003, ES=1.04) and slower kinetics during exercise (p=0.004, ES=1.0) compared to the control group. At recovery of exercise, no significant differences were observed between the groups in initial VO2, ΔVO2, and VO2 at the end of recovery (p>0.05). However, patients with SCH had a higher O2 debit (p=0.003, ES=1.02) and slower kinetics during recovery (p=0.001, ES=1.55) compared to the control group. In terms of symmetry, VO2 off-kinetics was slower than VO2 on-kinetics (Table 2). A representative example of VO2 on- and off-kinetics of both groups is shown in Figure 1.
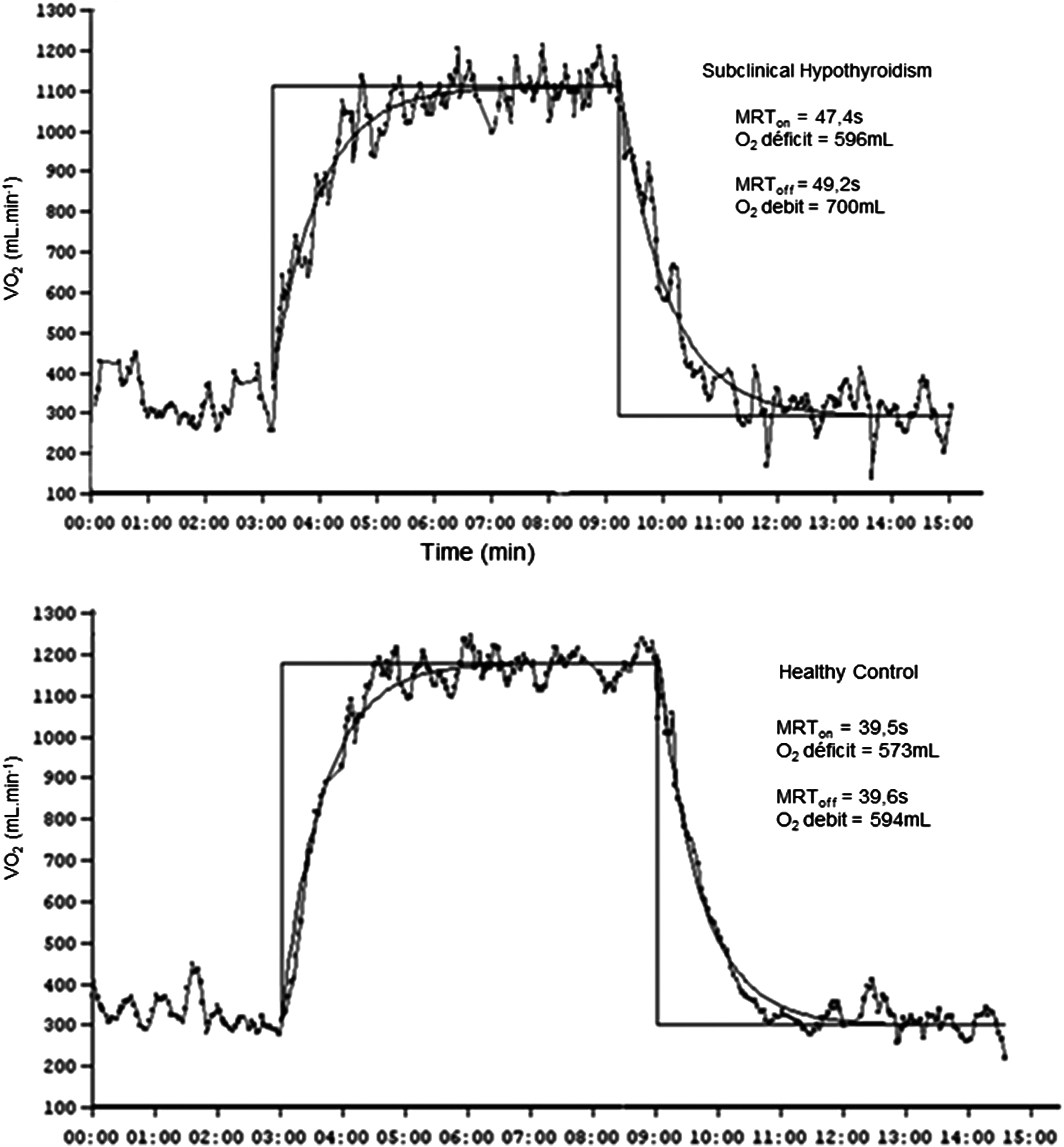
Pulmonary oxygen uptake kinetics during and after six minutes of submaximal exercise with constant load (50 W) in a representative woman with subclinical hypothyroidism (upper panel) and a woman without thyroid impairment (below panel). MRTon/off, mean response time of rest-exercise and exercise-recovery transition, time constant to reach 63% of ΔVO2 at the onset of exercise and recovery.
Note. Values are means±standard deviation.
Women with SCH differ from controls (p<0.05).
VO2b, baseline oxygen uptake; ΔVO2, amplitude of change in oxygen uptake; VO2ss, oxygen uptake in steady state; MRT, mean response time of VO2, time needed to reach 63% of ΔVO2; VO2rec, oxygen uptake at the end of recovery; O2 deficit, energy supplied by anaerobic metabolism at onset of exercise; O2 debit, extra energy demand during the recovery period. Both calculated by the formula: MRT×ΔVO2.
TSH levels showed a statistically significant positive correlation with VO2 on-kinetics (r=0.53, p=0.001) and VO2 off-kinetics (r=0.57, p=0.001). No relationship was found between the level of physical activity and TSH (p>0.05). The physical activity showed a statistically significant negative correlation with the VO2 on-kinetics (r=−0.44, p=0.006) and VO2 off-kinetics (r=−0.46, p=0.004). After controlling for the level of physical activity, TSH was positively correlated with VO2 on-kinetics (r=0.50, p=0.002) and VO2 off-kinetics (r=0.55, p=0.001). No correlation was observed between VO2 kinetics and VO2max (p>0.05). There were also no significant correlations between echocardiographic variables and VO2 kinetics (p>0.05).
Discussion
According to the literature, this is the first study to assess VO2 kinetics in patients with SCH. The results show that when performing a submaximal exercise of 50 W, patients with SCH have slower VO2 kinetics at on and off transitions and a greater O2 deficit and O2 debit than women without thyroid impairment. The effect size of the difference on the VO2 kinetics between groups indicates that this result may be related to the subclinical thyroid disease, since the groups were similar regarding possible confounding variables (age, BMI, physical activity, and VO2max). The systolic and diastolic cardiac functions at rest and the cardiopulmonary and hemodynamic responses at the steady state and during the submaximal exertion were preserved in patients with SCH. The results also show that higher TSH levels are associated with higher time constants (slower VO2 kinetics) and the measurement of VO2 kinetics in SCH is reproducible.
The kinetic response of VO2 during constant workload exercise has been studied in several clinical conditions and has allowed to identify and quantify, noninvasively, the impairments in oxidative metabolism and its determinants (34). Our results corroborate other research that found a delayed VO2 response at rest-exercise transition in different clinical populations (12,26 –28,31,35). According to our results, the VO2 on-kinetics of patients were on average 18% slower than in the control group (47 vs. 40 sec respectively). This delay in VO2 response to exercise caused a higher O2 deficit, implying greater predominance of anaerobic metabolism for energy supply at the exercise onset, through the predominant use of high-energy phosphates (ATP and phosphocreatine) and anaerobic glycolysis. The VO2 on-kinetic values found in patients with SCH are similar to those observed in beta-thalassemia (33), individuals with a history of myocardial infarction (19), transplanted patients (27), and those with mild coronary artery disease (26,28,31).
The physiological mechanisms involved with delayed VO2 kinetic response are still the subject of debate in the literature. Some authors believe that the kinetic response would be determined mainly by O2 delivery to active muscles, but recent studies suggest that the inertia of the intramuscular oxidative machinery is primarily responsible, involving the calcium absorption for activation of the hydrolysis and ATP synthesis (10,17). Tschakovsky and Hughson (36) believe that the adaptation of muscular aerobic metabolism in the exercise onset is determined by the interaction between metabolic inertia and the inertia in O2 transport. In thyroid disorders, it is possible to speculate that central (20) and peripheral factors are involved in VO2 kinetics slowed, especially in muscle enzymes and oxidative processes (20,37 –42).
It is known that thyroid hormones are determinants of the metabolic and contractile phenotype of skeletal muscles, and that they have a profound impact on the mitochondria (39). Thyroid hormones activate processes of ATP production, increasing mitochondrial respiration, so that the deficiency of these hormones leads to changes in the efficiency of oxidative phosphorylation processes (40). In hypothyroidism, there is evidence of changes in structure and biochemistry of skeletal muscle (39) as well as changes in mitochondrial metabolism (41). The presence of reduced expression of mitochondrial transcription factor A (h-mtTFA) has been described in Hashimoto's hypothyroid myopathy and is inversely correlated with TSH and aerobic threshold lactate, and positively correlated with the fT4 level (43).
Regarding VO2 off-kinetics, our results also confirm findings from other studies that found a delayed VO2 recovery after exercise in patients compared to healthy controls (30,44 –46). On average, VO2 off-kinetics of SCH patients were 23% slower than in the control group (54 vs. 44 sec respectively). The delayed VO2 recovery implies greater metabolic cost to perform repeated tasks and may have a significant implication for daily living tasks (45). If a patient with SCH performs various submaximal efforts throughout the day, oxygen deficits are generated and cannot be compensated during recovery before a new effort and hence lead to early fatigue.
The delay in the VO2 recovery may be a consequence of the inability of the circulatory system to deliver quickly the amount of oxygen required for restoring the peripheral muscle myoglobin, the impairment of gas exchange in the lung, and the use of mitochondrial oxygen (44).
An advantage of this study, compared to others that investigated cardiopulmonary responses in SCH, is the control of possible variables involved with VO2 kinetics, allowing analysis on the disease itself. It is known that VO2 kinetics are influenced by several factors, including physical fitness and the presence of diseases (10).
Importantly, no differences were observed in cardiopulmonary and hemodynamic responses and the efficiency of oxygen uptake during exercise between the groups. Monzani et al. (38) and Caraccio et al. (6) found significant differences in the cardiopulmonary and hemodynamic system during exercise in SCH. In both studies, however, the groups were not matched for VO2max. Our results corroborate a previous study that compared the efficiency of oxygen consumption (ΔVO2/ΔW) in patients with hyperthyroidism (20). It seems that the impairment of these patients in terms of response to stress occurs during the onset and at the end of exercise. This implies that factors related to the activation and suppression of the autonomic nervous system may also be involved in the explanation of VO2 kinetics in SCH. This study shows that although patients with SCH respond physiologically similarly to the healthy controls in the steady state of submaximal exercise, the SCH patients have an impaired VO2 response in rest-exercise and exercise-recovery transitions.
It is established that VO2 kinetics are associated with the physical activity, suggesting that the more active a person, the faster the VO2 kinetics. There is evidence in healthy population that demonstrate improvement in VO2 kinetics through physical training (47). However, this subject needs to be investigated in patients with SCH, as a recent study suggested that patients with SCH do not respond the same way to physical training compared to healthy individuals (48).
The kinetics measurement of VO2 in SCH patients showed high coefficients of reproducibility, with no significant differences between transitions performed on the same day or on different days. Our results show that VO2 kinetics are a reliable submaximal measure for assessing the functional capacity in SCH.
From a practical standpoint, measurement of VO2 kinetics in SCH may be used to monitor the effectiveness of strategies for improving exercise tolerance in these patients. Of note, prolonged kinetics during low-intensity exercise are related to poor prognosis in patients with mid to moderate congestive heart failure (16). The results of this study suggest that the physiological profile of patients with SCH is different from people without thyroid impairment, and therefore longitudinal studies should be conducted to verify the possibility of using this variable as a predictor of health-related outcomes of these patients.
There are several limitations to this study. First, only female volunteers were included. Moreover, the results apply only to exercise on a cycle ergometer with an intensity of 50 W. Since it was not the purpose of the study, it was not possible to determine the physiological mechanisms responsible for the slower kinetics in SCH. Thus, further studies should be performed to evaluate cardiac output, the O2 arteriovenous difference, the autonomic response and/or aspects of muscular metabolism, and other factors that are involved in VO2 kinetics in SCH patients. Furthermore, longitudinal studies should investigate the effect of physical training on VO2 kinetics in these patients.
In conclusion, VO2 kinetics of women with SCH are slower in rest-exercise and exercise-recovery transitions compared to women without thyroid impairment. This finding indicates a possible impairment in the dynamics of supply and use of O2 in SH patients during and after exercise. The degree of impairment may be associated with higher TSH levels.
Footnotes
Acknowledgments
We would like to thank Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for financial support and the Federal University of Ouro Preto (UFOP).
Author Disclosure Statement
The authors declare that they have no conflict of interest.