
Abstract
Background:
While there is consensus that significant extrathyroidal extension (ETE) (T4) should upstage a patient with well-differentiated thyroid cancer, the importance of minimal ETE (T3) remains controversial. Additionally, the importance of nodal metastases on prognosis has come under scrutiny. Recent publications highlight the importance of size, number of positive nodes, and, in particular, the presence of extranodal extension (ENE) as measures of disease aggressiveness. In this study, we examined whether ETE is a predictor of ENE.
Methods:
A retrospective review was conducted from January 2004 to March 2013. All node-positive patients who underwent total or completion thyroidectomy were included. Histologic features defined by the College of American Pathologists (CAP) protocol for thyroid carcinoma were recorded.
Results:
A total of 193 patients qualified for review. Patients who were found to have ETE were 12 times more likely to have lymph nodes in the primary setting with ENE than patients with intrathyroidal primary tumors (p<0.000). After exclusion of all T4 cases (n=6), patients with minimal ETE were 13 times more likely to have ENE than those with no ETE (p<0.000). Twenty percent of microcarcinomas with ETE demonstrated ENE.
Conclusion:
We have found that the biology of the primary tumor is conferred to the lymph node in that the presence of ETE leads to a significantly higher incidence of ENE. Awareness of this relationship should be accounted for in the management of primary and recurrent lymph nodes. This study shows that minimal ETE is a significant predictor of ENE. Although long-term survival and recurrence follow-up is not available for the majority of patients in this series, the presence of ENE as a surrogate for more aggressive disease biology and its strong association with minimal ETE supports the upstaging of patients with minimal ETE.
Introduction
T
In terms of the primary thyroid malignancy, Ito et al. argued that the use of minimal ETE as a poor prognostic indicator is not justified (2). They contend that there is not a significant difference in disease-free survival between patients with T1/T2 tumors and those with T3 neoplasms that were upstaged on the basis of ETE alone (2). As a result, Ito et al. and others have challenged the current classification systems (2,3), which upstage patients on the basis of minimal ETE (4,5).
On the other hand, a number of recent publications have highlighted the prognostic significance of specific histologic features of involved lymph nodes rather than simply the presence of metastatic deposits (3,6 –10). One of the main criticisms of the current staging system is that the controversial practice of prophylactic central compartment neck dissections for clinically node-negative patients (cN0) results in potentially unwarranted upstaging (1).
The current trend in thyroid cancer staging has moved toward classifying lymph nodes based on a number of significant characteristics, including the size, number of affected nodes, and the presence of extranodal extension (ENE) (1,6 –8,10,11). ENE in thyroid cancer was first reported in 1989 by Spires et al. However, they did not identify this as a significant adverse prognostic feature (12). Since that initial publication, ENE has been found to be significantly associated with the development of distant metastases (7,8,13), disease persistence (10), and disease-specific mortality (6).
In their initial report, Spires et al. (12) did allude to the possible correlation between the presence of ETE and ENE, while more recently a significant relationship between extensive ETE and ENE was described by Lango et al. (10). However, to date, no study has systematically examined the effect of minimal ETE on the extranodal status of the affected lymph nodes.
In this study, we examined the effect of ETE on the extranodal status of the affected lymph nodes removed in the primary setting, in order to determine if ETE is predictive of ENE in node positive patients. We hypothesized that if ETE represents a more virulent phenotype of well-differentiated thyroid cancer (WDTC), then this aggressiveness might be conferred to the metastatic lymph nodes.
Materials and Methods
Following IRB approval, a single surgeon retrospective review was conducted from January 2004 to March 2013. Cases were identified using the thyroid cancer diagnosis code (ICD9: 193) and included both total and completion thyroidectomies. The standard practice of the senior surgeon (M.L.U.) has been the performance of bilateral central compartment neck dissections for both cN0 and cN1 patients.
Patients with WDTC and pathologically positive nodes (either central and/or lateral) were identified and included in the study population. Patients with no nodal metastases or aggressive histologies (medullary, tall cell, anaplastic) were excluded from the review. Although this study spans a 9-year period, the majority of patients were identified in the latter portion of this time period because ENE was not routinely and uniformly reported by the pathologists in our institution until the last several years. This precludes our ability to provide meaningful follow-up in the majority of patients in this series.
All qualifying patients were categorized into one of four groups based on the information in their pathology report (Fig. 1). The histologic slides were then reviewed again by the senior pathologist (B.M.W.) to confirm the designation of ETE, ENE, as well as lymph node positivity. Histologic features defined by the College of American Pathologists (CAP) protocol for thyroid carcinoma were recorded (14).
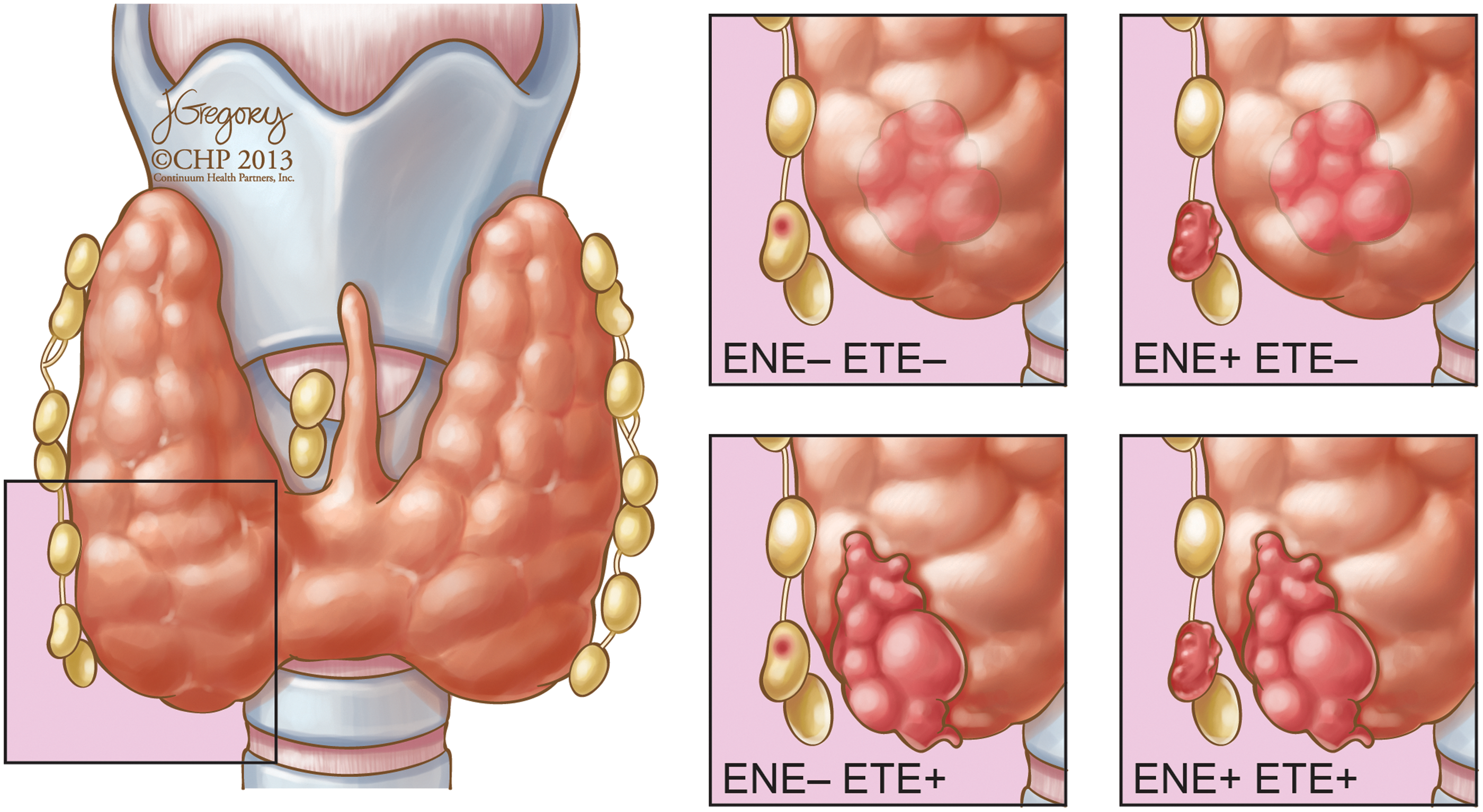
Illustrations depicting the four categories that patients were classified into based on the status of extrathyroidal extension (ETE) and extranodal extension (ENE). Color images available online at
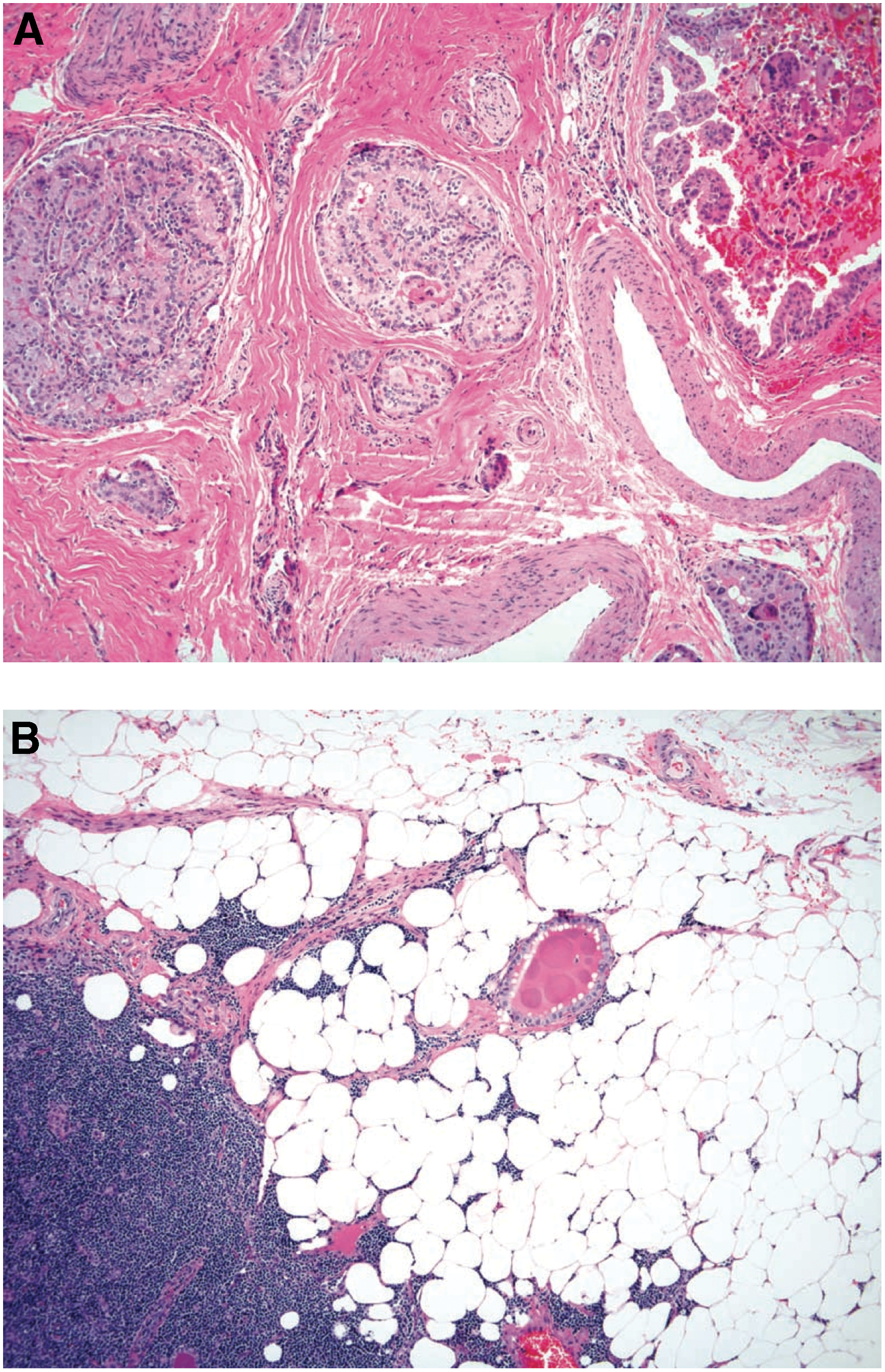
Minimal ETE was defined as invasion into fat, skeletal muscle, nerve, and/or thick-walled vascular structures. Extensive ETE, justifying upstaging to pT4a, was defined as invasion of the recurrent laryngeal nerve, esophagus, trachea, jugular vein, or subcutaneous soft tissues (Fig. 2a). ENE was defined using the same criteria mentioned for ETE, but no distinction was made based on extent of invasion (Fig. 2b).
Statistical analysis
Pathologic results were entered into a de-identified database, and an odds ratio estimate was used to examine the null hypothesis that patients with positive ETE are not more likely to have ENE when compared to those without ETE. Cohorts were compared using Fisher's exact test and odds ratio.
Results
A total of 193 patients were identified who met the study criteria. After the pathologic review, 31 patients were found to have positive ETE and negative ENE, 41 patients were found to have positive ETE and positive ENE, 12 patients were found to have negative ETE and positive ENE, and 109 patients were found to have negative ETE and negative ENE (Table 1).
Patients with positive extrathyroidal extension (ETE) were 12 times more likely to manifest lymph nodes with extranodal extension (ENE) than patients with intrathyroidal tumors (p<0.000).
Excluding T4 cases (n=6), 27 patients were found to have positive ETE and negative ENE, 39 patients were found to have positive ETE and positive ENE, 12 patients were found to have negative ETE and positive ENE. A total of 109 patients were found to have negative ETE and negative ENE (Table 2). ENE was identified in metastatic lymph nodes as small as 3.5 mm.
After excluding the T4 cases, patients with minimal ETE were 13 times more likely to have positive lymph nodes with ENE than T1/T2 tumors (p<0.000).
Statistical analysis of all 193 cases demonstrated that patients with positive ETE were 12 times more likely to manifest lymph nodes with ENE than patients with intrathyroidal tumors (p<0.000). After excluding the T4 cases, we found that patients with minimal ETE were 13 times more likely to have positive lymph nodes with extranodal spread than T1/T2 tumors (p<0.000). Twenty percent of microcarcinomas that presented with ETE had positive nodes with ENE.
Excluding patients with extensive ETE, patients with +ETE/+ENE had a significantly larger primary tumor size as compared to patients with −ETE/−ENE (p=0.004). Patients with +ETE/−ENE had a marginally statistically significantly larger primary tumor size as compared to patients with −ETE/−ENE (p=0.053). Patients with −ETE/+ENE did not have a significantly larger primary tumor size as compared to patients with −ETE/−ENE (p=0.399; Table 3).
Patients with +ETE/+ENE had a significantly larger primary tumor size (2.3 cm) as compared to patients with −ETE/−ENE (1.4 cm) (p=0.004).
Using Bonferroni correction.
Fifty-four percent of cases that were +ETE/+ENE had primary tumors that would have been staged as T1 on the basis of size alone (Table 4). There was no significant relationship between the size of the primary tumor and the probability of ENE.
This shows that 54% of T3 cases with ENE (n=39) would have been staged as T1 on the basis of primary tumor size alone.
Discussion
Lymph node metastases have been reported to occur in up to 82% of patients who undergo treatment for WDTC (15). It has become increasingly apparent that not all types of nodal metastases have the same level of prognostic significance, and in particular, there is a considerable amount of controversy regarding the clinical importance of the smaller end of the spectrum of nodal metastases (1). Virtually all of the current staging systems for differentiated thyroid cancer that include lymph node status are based on the mere presence of positive lymph nodes. However, recent literature has focused on the importance of specific features of the nodal metastases, including size, number of positive nodes, and presence of ENE (1). The current clinical practice guidelines advise surgeons to perform a lymph node dissection when encountering clinically apparent lymph nodes and/or biopsy proven nodal metastases (16). However, there is no consensus as to the role of prophylactic central or lateral compartment dissection, and the ATA currently does not advise for or against prophylactic central compartment neck dissection.
It has been documented that the incidence of nodal metastases increases as the size of the primary thyroid cancer increases, notwithstanding the fact that even microcarcinomas have nodal metastases in up to 64% of cases (17). If the clinician had information that would provide clues as to the potential virulence of those lymph nodes, it could affect clinical decisions both in the primary treatment setting as well as when managing patients with recurrent nodal disease.
Ideally, the clinician should be able to use available information regarding the primary tumor to understand the potential virulence of metastatic lymph nodes. It has already been established that extensive ETE is a poor prognostic indicator, a manifestation of a more aggressive tumor, and is significantly correlated with ENE (2,3,10,18). Other features of the primary disease, such as the BRAF V600E mutation, have been shown to predict a significantly worse disease-free survival, particularly when it presents simultaneously with ENE (9,19,20).
In this study, we found that the more aggressive biology of the primary tumor, demonstrated by ETE, was reflected in the metastatic lymph nodes in the form of ENE. It has been previously shown that minimal ETE is significantly associated with increased rates of central compartment metastases (3,21,22), and is correlated with a higher rate of recurrence (18). However, a 2006 retrospective review by Ito et al. concluded that for patients older than 45 years, minimal ETE had no effect on the disease-free survival over an 8-year (mean) follow-up (2). Similar findings were reported by Nixon et al. in a 2011 review, who found that minimal ETE did not have a significant impact on disease-free survival or recurrence-free survival (5). A separate study by Leboulleux et al. arrived at similar findings that minimal ETE was not a prognostic factor for persistent or recurrent disease (mean follow-up 8 years) (3). As a result, there is controversy regarding the clinical implications of minimal ETE.
On the other hand, there is a growing body of evidence regarding the clinical implications of ENE. The first mention of ENE as a measure of disease aggressiveness was in 1989 by Spires et al. (12). Since then, there has been complete agreement in the literature that ENE indicates a more aggressive tumor (Table 5) (1,6,7,9,10,12,13,23 –29). In particular, lymph node metastases that have extranodal spread are associated with increased risk of nodal persistence and decreased probability of biochemical remission (3,6,7,10,13). Patients with ENE also have an increased reported risk of systemic disease progression (7,10), as well as a worse disease-specific survival (1,9). In 2007, Ito et al. separated ENE into minimal and extensive extension (based on intraoperative findings). ENE predicted worse disease-free and cause-specific survival, but there was not a significant difference between minimal and extensive disease extension into the perinodal soft tissues.
RAI, radioactive iodine.
It is tempting to hypothesize that the presence of ENE is related to the size of the metastatic deposit and that perhaps a progression exists between lymph node size and growth of disease through the lymph node capsule. Although the size of the lymph node with ENE was not available for all cases in our review, it is noteworthy that there were at least two cases in which ENE presented in a lymph node that was less than 5 mm. This suggests that there may not be a direct relationship between lymph node size and ENE positivity, and that ENE may be an independent manifestation of an aggressive thyroid cancer. A large study examining the relationship between lymph node size and ENE is needed to evaluate this relationship further.
ENE is a well-accepted indicator of poor prognosis, while the implications of minimal ETE are more contentious. One potential reason for this difference could be the theory alluded to by Ricarte et al. that ENE presents later in the disease process (9). If ENE does in fact represent a later manifestation of more virulent disease, then it would follow that patients with ENE would have a poorer prognosis that should be identified in a shorter follow-up period. Additionally, both studies that reported minimal ETE as an insignificant predictor of poor prognosis had a mean follow-up period of 8 years. This contrasts with the longest follow-up time reported in the ENE group of studies, which was almost 14 years (7).
In our retrospective review, we found that ETE (both minimal and extensive) made a patient with positive lymph nodes 12 times more likely to have ENE. When we excluded the T4 (extensive ETE) cases, we found that patients with minimal ETE were 13 times more likely to have lymph nodes with ENE. We did not find a significant relationship between the size of the primary tumor and the probability of ENE in the lymph nodes. Of note, 21 of the 39 T3 tumors in the +ETE/+ENE cohort (54%) would have been staged as T1 on the basis of tumor size alone. Because of the trend away from performing prophylactic central neck dissections, in practice many of these 21 patients with <2 cm primary tumors would likely not undergo a central neck dissection and therefore ENE would not be identified. Additional outcomes data with long-term follow-up is required for an analysis of the impact of a prognostic factor on survival. However, this study has demonstrated the strong statistically significant association between minimal ETE and nodal metastases with ENE. Due to the evolving number of reports that reflect the negative impact of ENE on prognosis, the results of this study can be interpreted as offering indirect support for continued upstaging of tumors with minimal ETE.
The strongly significant relationship between minimal ETE and ENE suggests that the spread of the primary tumor into the fat, skeletal muscle, nerve, or fibroconnective tissue surrounding the thyroid is a manifestation of a more aggressive disease biology. The significant link between ETE and ENE is particularly important because the prognostic implications of ENE have been studied over longer time periods than ETE, and it has been suggested that ENE may present later in the disease process. It is possible, then, that the two studies that found minimal ETE to be an insignificant predictor of recurrence- and disease-free survival were unable to appreciate this relationship due to an insufficient follow-up period.
Another aspect of the disease biology that remains unknown is whether there is a predetermined progression of disease in lymph nodes that will manifest over time if a disease is allowed to progress over the course of decades. While it stands to reason that all lymph node metastases begin as microscopic deposits, it is unclear as to whether they all have the potential to progress to macroscopic nodes, nodes with minimal ENE, and finally nodes with gross ENE. It is equally uncertain as to whether a node with ENE has the biologic ability to continue to progress in the extranodal environment and to invade surrounding visceral, neural, and vascular structures.
This relationship has implications for the management of the thyroid cancer patient, both in the primary setting and in the face of recurrence. The significant association between minimal ETE and ENE, as well as the information that minimal ETE is a significant predictor of ipsilateral metastases (22), should be considered by the surgeon when treating the patient with a cN0 neck. Furthermore, when faced with nodal recurrence, the clinician should consider the increased risk of a more virulent group of metastatic lymph nodes in patients with a primary tumor manifesting ETE. This fact may be quite significant in the multifactorial decision as to whether to proceed with surgery or observation.
Conclusion
Thyroid cancer generally carries a favorable prognosis, but it is a disease that requires lifelong surveillance (30 –32). Studies have reported opposing conclusions as to the prognostic implications of minimal ETE, while there is growing consensus regarding ENE. In our patient population, those with minimal ETE were significantly more likely to have ENE in affected lymph nodes. It appears that the biology of the primary tumor is conferred to the metastatic nodes and predetermines a different nodal phenotype. Thus, ETE, both minimal and extensive, should alert the clinician to a more aggressive disease process. This study shows a strong and significant association between minimal ETE and nodes manifesting ENE. The literature supports the fact that ENE has adverse prognostic implications. Therefore, it can be inferred that minimal ETE should be considered a marker for poor prognosis. However, long-term follow-up is required to determine if the apparent virulence of the disease affects disease-specific mortality and/or risk of recurrence.
While that follow-up will take years to determine, the knowledge that patients with ETE have a significantly higher likelihood of harboring metastatic nodes with ENE has important management implications. The conference of an aggressive biology to the nodes should be accounted for in the decision to perform a prophylactic lymph node dissection and is also important in deciding how best to manage recurrent lymph nodes, especially if there is a higher likelihood that the nodes will have ENE and the potential to invade surrounding structures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.