
Abstract
Background:
The treatment of advanced medullary thyroid carcinoma (MTC) has evolved significantly over the past decade. The discovery of genetic abnormalities in MTC has led to the development of targeted therapies such as vandetanib and cabozantinib. Other kinase inhibitors (KI), such as sorafenib, have been investigated in this setting and are an alternative therapeutic option. The lack of specificity of these KIs to a single target may result in additional, unexpected effects. In this report, we describe a patient with metastatic MTC and Ectopic ACTH (adrenocorticotropic hormone) Syndrome in whom treatment with sorafenib resulted in complete resolution of hypercortisolism.
Summary:
A 45-year-old male with progressive metastatic MTC presented with clinical manifestations suspicious for Cushing's syndrome. Investigation revealed ACTH-dependent hypercortisolism suggestive of Ectopic ACTH Syndrome. Treatment with sorafenib 400 mg twice a day was initiated resulting in a rapid and significant reduction of cortisol and ACTH levels associated with dramatic clinical improvement. The rapid and effective control of hypercortisolism in the absence of a significant tumor reduction raises the question of whether sorafenib may have a direct effect on ACTH or cortisol hypersecretion.
Conclusions:
This report suggests a previously unknown potential effect of sorafenib on the pituitary–adrenal axis. Further studies will be necessary to investigate the role of sorafenib in other cases of ACTH excess and to understand the mechanisms by which it alters steroid synthesis, action, or secretion.
Introduction
M
The discovery of these molecular abnormalities provided the basis for the development of targeted molecular therapies for advanced metastatic MTC. In the past two years, two kinase inhibitors (KI)—vandetanib and cabozantinib—have been approved by the Food and Drug Administration (FDA) for the treatment of progressive metastatic MTC (5,6). Other KIs, such as sorafenib, have been investigated in Phase II studies, and represent a therapeutic off-label option (7).
As other neuroendocrine cells, parafollicular C cells have the potential to produce peptides such as adrenocorticotropic hormone (ACTH) and/or corticotropin releasing factor (CRF) that can ultimately result in Cushing's syndrome (CS). Ectopic ACTH Syndrome (EAS) is an uncommon cause of CS. Small-cell lung carcinoma (SCLC) is the most frequent malignancy associated with EAS; other associated tumors include neuroendocrine tumors arising from the lung, bronchus, thymus, pancreas, and from the thyroid gland (8). Despite being uncommon, EAS in MTC is usually associated with extensive metastatic disease and is therefore associated with a poor prognosis. Control of hypercortisolism by drugs that inhibit cortisol synthesis such as ketoconazole and metyrapone is usually initiated prior to antitumor treatment to improve the clinical status and enable treatments that aim at tumor mass reduction to achieve control of ACTH production.
Here, we report a case of progressive metastatic MTC with EAS in whom treatment with sorafenib, despite being initiated prior to introduction of cortisol synthesis inhibitors, resulted in an unexpectedly rapid control of hypercortisolism without significant reduction of the tumor mass.
Methods
The patient provided written consent, and the Institutional Research Ethics Committee approved publication of the case report.
Serum and urinary cortisol, ACTH, and calcitonin levels were measured by chemiluminescent assays (Immulite 2000 system, Siemens Healthcare, Surrey, United Kingdom). CEA levels were measured by an eletrochemiluminescent assay. The reference ranges for serum cortisol, urinary cortisol, ACTH, calcitonin, and CEA are 5–25 μg/dL, 50–310 μg/24 h, 12–55 pg/mL, <8.4 pg/mL, and <10 pg/mL respectively.
Genomic DNA was extracted from peripheral blood according to a standard salting-out protocol. Exons 5, 8, 10, 11, and 13–16 were amplified by polymerase chain reaction (PCR). Mutation analysis was conducted on a 3130xl automated sequencer (Applied Biosystems, Foster City, CA) according to the manufacturer's recommendations.
Case Report
In May 2012, a 45-year-old white male with metastatic MTC was referred to our institution after being treated unsuccessfully with two systemic chemotherapy regimens. At presentation, he complained of weight gain, muscle weakness, and diarrhea. On physical examination, the patient was plethoric and had a moon facies, fullness of supraclavicular fat pads, a buffalo hump, central obesity, and severe proximal muscle weakness leading to the suspicion of hypercortisolism. Imaging studies to evaluate tumor extent as well as laboratory tests to rule out CS were ordered.
Imaging studies revealed widespread metastatic disease with involvement of mediastinal and abdominal lymph nodes, lungs, and liver. Analysis of the RET proto-oncogene failed to reveal a germline mutation. Biochemical analysis revealed elevated calcitonin and CEA levels, as well as elevated ACTH and cortisol levels (Fig. 1 and Table 1). These results were consistent with ACTH-dependent hypercortisolism that, in the context of metastatic MTC, was suggestive of EAS.
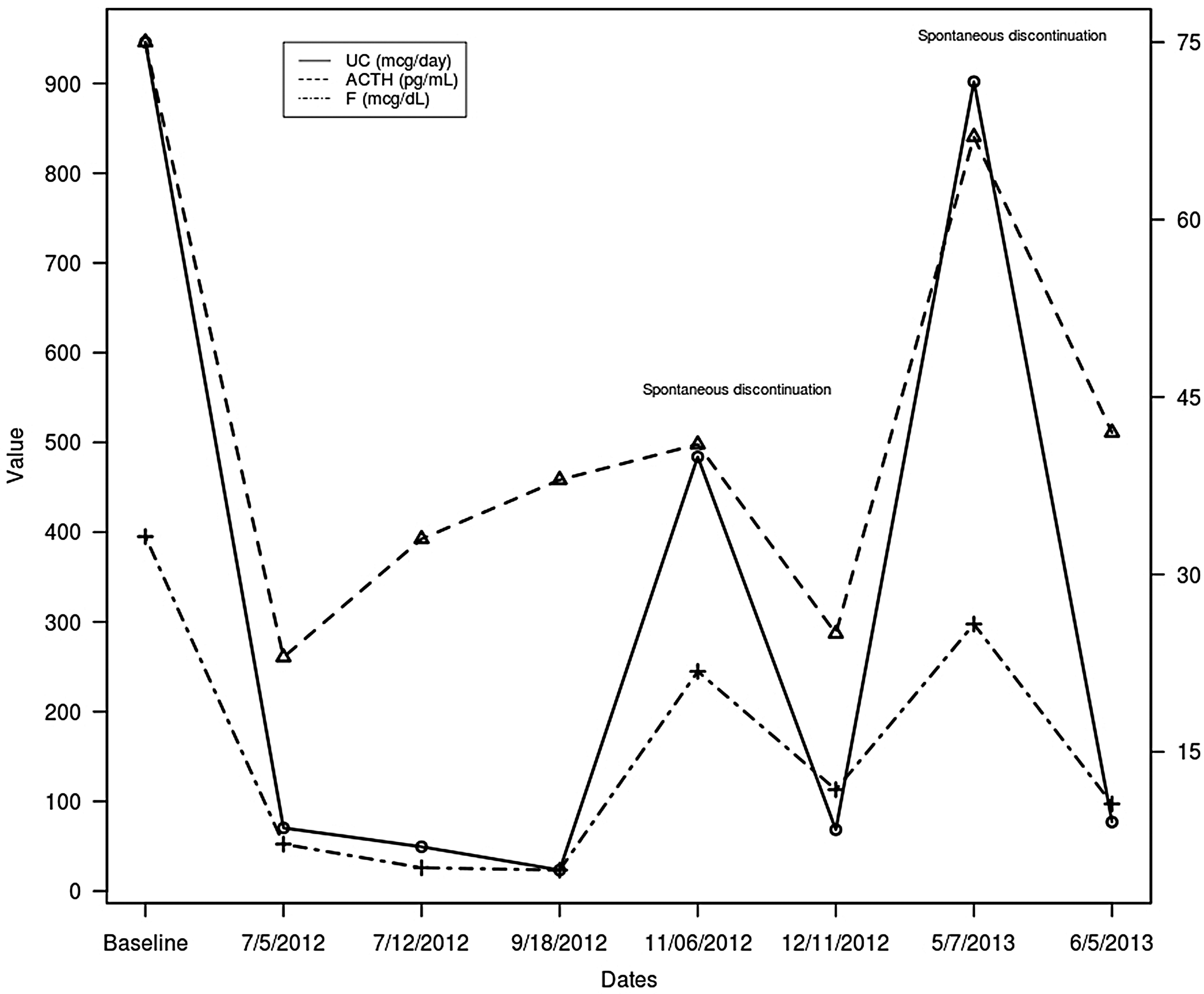
Serum cortisol, 24 hour urinary cortisol (UC), and adrenocorticotropic hormone (ACTH) levels while on sorafenib therapy. The graph depicts levels at baseline (time when hypercortisolism was suspected) and after initiation of sorafenib (6/29/2012) at a dose of 400 mg twice a day. The measurements on 11/6/2012 and 05/07/2013 were performed while the patient was off sorafenib.
Off sorafenib.
CEA, carcinoembryonic antigen; ACTH, adrenocorticotropin hormone; UC, urine cortisol.
As vandetanib or cabozantinib were not available at our institution, it was decided to initiate sorafenib 400 mg twice a day to control tumor mass, and metyrapone to control cortisol hypersecretion. However, while waiting for importation of metyrapone, the patient received sorafenib alone. Surprisingly, one week after starting sorafenib, the patient showed significant clinical improvement, and laboratory evaluation revealed a dramatic reduction of urinary cortisol and ACTH levels—a 94% and 69% reduction from baseline respectively (Fig. 1 and Table 1).
Urine and serum cortisol levels remained in the normal range throughout therapy except for two periods of spontaneous discontinuation of sorafenib in June 2012 due to foot pain and in May 2013 for ocular pain and asthenia. While off sorafenib, a 24-hour urine collection for cortisol was coincidently performed, revealing an elevation of the cortisol level that returned to normal range after reintroduction of sorafenib (Fig. 1). Despite a reduction of calcitonin and CEA levels observed after initiation of sorafenib therapy (Table 1), imaging studies to assess tumor response showed no reduction of tumor mass but rather stabilization of disease. The disease remained stable until August 2013 when imaging and laboratory studies revealed significant progression of disease and loss of hypercortisolism control. At that time, sorafenib was discontinued to start alternative therapy. The levels of calcitonin, CEA, ACTH, and urinary cortisol after sorafenib discontinuation are shown in Table 1.
Discussion
EAS accounts for 5–10% of cases of CS, and covers a spectrum of tumors ranging from occult lesions to extensive metastatic and aggressive malignancies (9). CS in MTC is rare. In a French retrospective series, among 1640 patients with MTC, 13 developed EAS (0.7%) (10). Definitive treatment of EAS consists of surgical resection of the ACTH secreting tumor. When surgical resection is not an option, anticancer agents and drugs to control cortisol hypersecretion should be initiated. Ketoconazole, metyrapone, and mitotane are the most frequently used steroid synthesis inhibitors. Ketoconazole is widely available, but liver dysfunction is a concern in patients with extensive liver metastases. For this reason, we intended to use metyrapone treatment in addition to the antineoplastic treatment. As our patient had previously failed two chemotherapy regimens and neither vandetanib nor cabozantinib were available in our country, we opted to start off-label sorafenib.
As demonstrated in Figure 1, the initiation of sorafenib alone resulted in a rapid and significant reduction of cortisol and ACTH levels associated with a dramatic improvement of the patient's well-being. This fact, associated with modest reduction of calcitonin and CEA levels and the stable tumor size, suggests that sorafenib could have a direct effect on hormonal hypersecretion. Furthermore, the rise of urine cortisol while the patient was temporarily off sorafenib with normalization after re-initiation of therapy further suggests this possibility (Fig. 1).
A review of the literature has provided some insights into potential mechanisms by which sorafenib could in fact regulate the pituitary–adrenal axis. First, the magnitude and rapidity of cortisol reduction suggests a direct role of sorafenib on the inhibition of ACTH or cortisol synthesis. Regarding ACTH synthesis, Fukuoda et al. (11) showed by in vitro studies that gefitinib (a KI targeting EGFR) effectively suppresses POMC mRNA expression and ACTH secretion in human, canine, and mouse corticotroph adenoma cell lines. They further showed that the effect of EGFR on the POMC promoter was MAPK-dependent. Given that sorafenib is a BRAF inhibitor, one could hypothesize that sorafenib could regulate ACTH synthesis by inhibition of the MAPK pathway. A second hypothetical mechanism would be downregulation of the ACTH action by the inhibition of the downstream signaling pathway by sorafenib. Recent work by Carbajal et al. (12) has demonstrated an important regulatory pathway in steroidogenesis that involves a crosstalk between membrane G protein-coupled receptors, such as the ACTHR, and membrane receptor tyrosine kinases. It has been shown that the activation of cAMP/PKA by ACTH in adrenalcortical cells (Y1 adrenal cells) leads to ligand-independent trans-activation of the EGFR, which in turns lead to activation of MAPK and phosphorylation of STAR, a step required for rapid steroidogenesis (12). The other possibility is that treatment with sorafenib could result in cortisol deficiency by inducing ischemia of the adrenal and/or pituitary gland. Kamba et al. (13) demonstrated high expression of VEGFR-2 and VEGFR-3 in endothelial cells of the adrenal cortex and pituitary. Mice treated with continuous inhibition of VEGF presented significant capillary regression in these organs. In another animal study, treatment with sunitinib (a tyrosine kinase inhibitor of VEGFR 1, 2, and 3, PDGFRβ, and c-Kit) induced a dose- and time-dependent impairment of the adrenal cortex microvasculature, resulting in adrenal congestion, hemorrhage, or necrosis (14). Based on this study, the FDA recommended monitoring for adrenal insufficiency (AI) in patients on sunitinib treatment that are under stress from surgery, trauma, or severe infection (15).
Kinase inhibitors, including sorafenib, are promiscuous, as they can target several signaling pathways at once and affect several different cellular functions that can result in a variety of unexpected and unwanted effects. Although there are reports of different hormonal abnormalities in patients treated with TKIs, the best documented and most prevalent associated disorder is hypothyroidism, observed in 27–85% of patients (16,17). As treatment with sorafenib and other kinase inhibitors are often associated with side effects such as nausea, vomiting, anorexia, and fatigue, we also raise the question of whether these symptoms could be secondary to partial hypoadrenalism induced by kinase inhibitors. Recently, two different groups reported two cases of reversal of CS by vandetanib: one in a 58-year-old man with sporadic MTC (18), and the other in a child with multiple endocrine neoplasia 2B associated with MTC (19). Similar to this case report, the authors reported a rapid decrease in cortisol level after starting the TKI, dissociated from the antitumoral action, suggesting a direct effect of the TKI on hormonal secretion. These reports indicate that regulation of ACTH and/or cortisol synthesis is not unique to sorafenib but is extended to other kinase inhibitors.
In conclusion, we report a patient with widely metastatic MTC with EAS in whom treatment with sorafenib resulted in an efficient and sustained reduction of cortisol levels. This report suggests that sorafenib could be an effective treatment of hypercortisolism and also raises the question of whether common side effects associated with TKI treatment could be related to hypoadrenalism. Further studies will be necessary to define clearly the role of sorafenib on adrenal function, and to investigate the role of sorafenib in the treatment of EAS or in severe hypercortisolism from CS.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.