
Abstract
Background:
Postpartum thyroid dysfunction occurs in approximately 5–10% of women in the general population within one year of delivery. Differentiation of postpartum Graves' thyrotoxicosis (PPGr) from postpartum destructive thyrotoxicosis (PPDT) is essential because of the difference in treatment measures between the two. However, it is sometimes difficult because radioactive iodine uptake is contraindicated when patients are lactating. We examined the usefulness of determining the time of onset postpartum and measurement of antithyrotropin (anti-TSH) receptor antibodies and thyroid blood flow.
Methods:
Forty-two patients with newly developed thyrotoxicosis after delivery were examined: 18 had Graves' disease and 24 had destructive thyrotoxicosis. Serum free thyroxine (fT4), free triiodothyronine (fT3), and TSH were measured by chemiluminescent immunoassays. Anti-TSH receptor antibodies (TRAb), antithyroglobulin antibodies (TgAb), and antithyroid peroxidase antibodies (TPOAb) were measured by the Elecsys electrochemiluminescence immunoassay. Thyroid volume and blood flow (TBF) were measured quantitatively by color flow Doppler ultrasonography.
Results:
Onset of thyrotoxicosis was distributed from 2 to 12 months postpartum. Twelve (85.7%) of 14 patients who developed thyrotoxicosis at three months or earlier after delivery had PPDT. On the other hand, all 11 patients who developed thyrotoxicosis at 6.5 months or later had PPGr. All patients with PPGr had positive TRAb (14.9±14.9 IU/L, mean±standard deviation (SD)) and all patients with PPDT had negative TRAb (0.1±0.3 IU/L, p<0.0001). Fifteen (83.3%) of 18 PPGr patients had high TBF of more than 4.0% (8.9±4.4), and all PPDT patients had low TBF of <4.0% (1.6±1.0, p<0.0001). The fT3/fT4 ratio was higher in PPGr (64.0±23.9) than in PPDT (38.9±13.1, p<0.0002), but absolute values overlapped between the two.
Conclusion:
Early onset of thyrotoxicosis postpartum was associated mainly with PPDT, and a late onset was suggestive of PPGr. Positive TRAb and high TBF >4.0% are indicators of postpartum onset of Graves' disease.
Introduction
P
Detection of antithyrotropin (TSH) receptor antibodies (TRAb) is a prominent method for the diagnosis of Graves' thyrotoxicosis. However, second-generation TRAb are positive in approximately 10% of patients with painless thyroiditis (8). Indeed, in our study, some overlap of second-generation TRAb was found between Graves' thyrotoxicosis and painless thyroiditis (9). However, third-generation TRAb has greatly improved the sensitivity and specificity (10). Our hospital introduced this assay in 2008 as a routine test for the diagnosis of Graves' disease, after careful evaluation and modification of prototype assay kits (10). The result is obtained within 30 minutes.
We also developed a new method to measure thyroid blood flow (TBF) quantitatively (11). This is also effective for the differentiation between destruction-induced thyrotoxicosis and Graves' thyrotoxicosis, and the result is obtained within 10 minutes (11).
This is the first study in which a sensitive third-generation assay of TRAb and quantitative measurement of TBF have been applied for differential diagnosis of postpartum thyrotoxicosis.
Subjects and Methods
Subjects
Patients are referred to our outpatient clinic for assessment when they have thyroid dysfunction. We retrospectively reviewed the charts of 42 patients who had newly developed thyrotoxicosis within one year after delivery from January 2010 to July 2012. Thirty-one of these 42 patients were lactating at the time of diagnosis. Graves' disease and destructive thyrotoxicosis (painless thyroiditis) were diagnosed according to the diagnostic guidelines of the Japan Thyroid Association (12), defined by clinical findings and the determination of serum free thyroxine (fT4), free triiodothyronine (fT3), TSH, TRAb, and TBF. Patients were followed once every couple of months until they entered a euthyroid state. Blood samples were taken every time they visited our clinic. Final diagnosis was confirmed by following up the patients. Eighteen patients were diagnosed with postpartum Graves' disease (PPGr) and 24 patients with postpartum destructive thyrotoxicosis (PPDT). We excluded patients with previous Graves' disease who had been diagnosed before they became pregnant or were treated by antithyroid drug therapy.
Thyroid function and autoantibodies
TSH, fT4, and fT3 concentrations were measured using chemiluminescent immunoassays (Architect TSH, Architect fT4, and Architect fT3 respectively; Abbott Japan Co., Tokyo, Japan). Normal ranges are 0.3–5.0 mU/L for TSH, 0.7–1.6 ng/dL for fT4, and 1.70–3.70 pg/mL for fT3. Serum levels of thyroglobulin antibodies (TgAb), antithyroid peroxidase antibodies (TPOAb), and TRAb were measured using an electrochemiluminescence immunoassay (ECLusys 2010; Roche Diagnostics Japan Co., Tokyo, Japan; normal range: <39.9 IU/mL for TgAb, <27.9 IU/mL for TPOAb, and <1.9 IU/L for TRAb), as previously reported (13).
Ultrasound measurements of thyroid volume and blood flow
The ultrasound diagnostic equipment used was the SSA-770A (Aplio 80) and SSA-700A (Aplio 50; Toshiba Medical Systems, Otawara, Tochigi, Japan) in connection with an 8 MHz linear transducer (PLT-805AT; Toshiba Medical Systems, Otawara, Tochigi, Japan). Thyroid volume and TBF were measured quantitatively as reported previously (11). For measurement of TBF, differential tissue harmonic imaging (DTHI) was performed for the gray-scale B-mode imaging, which utilizes nonlinear harmonic signals during propagation of the pulse wave. Advanced dynamic flow (ADF), generally explained as a high-resolution power Doppler mode, was performed for the blood flow detection. The displayed depth was set to 4 cm. The region of interest (ROI) of ADF was expanded to the maximum, and the gain of ADF was set to the maximum but below the noise level. The motion target indication (MTI) filter was set to a minimum in order to detect the blood flow at low velocity. The acquired ADF images were analyzed using dedicated software running on a PC. The software, programmed by C++, has a graphical user interface. When a user draws a ROI as an arbitrary shape, the program calculates (a) the number of pixels of the whole ROI, (b) the number of pixels painted by ADF signals, and (c) the ratio (expressed as %) between the two. The actual area corresponding to the pixel values is always displayed in cm2. Finally, the quantitative value of thyroid blood flow is expressed as a percent, as shown above. TBF measurement was reproducible, and intra-assay CV was 4.74% at 22.5% of TBF. This assay was introduced in 2007 as a routine test in Kuma Hospital. All ultrasound operators have been well trained and subsequently attained high levels of proficiency in our hospital. Calculating TBF is so simple that operator difference is negligible. The operators were blinded to the results of laboratory tests of patients when they performed ultrasound scans. The cutoff value of differentiation between Graves' disease and destructive thyrotoxicosis was 4.0%.
Statistical analysis
Comparisons of various parameters between PPGr and PPDT were performed by the Mann–Whitney U-test. Differences were considered to be significant at p<0.05.
Results
Table 1 shows clinical and laboratory data at the onset of thyrotoxicosis in patients with PPGr and PPDT. The age of onset was significantly older in patients with PPGr than in those with PPDT. Onset time of thyrotoxicosis was distributed from 2 to 12 months postpartum (Fig. 1). Twelve (85.7%) of 14 patients who developed thyrotoxicosis at three months or earlier after delivery had PPDT. On the other hand, all 11 patients who developed thyrotoxicosis at 6.5 months or later had PPGr. All patients with PPGr had positive TRAb, and all patients with PPDT had negative TRAb (Fig. 2). Fifteen (83.3%) of 18 PPGr patients had high TBF >4.0% (Fig. 3), and all PPDT patients had low TBF <4.0%. The low TBF values in three patients with PPGr were 2.8, 3.0, and 3.8%, and their onset times of thyrotoxicosis were three, three, and six months postpartum respectively.
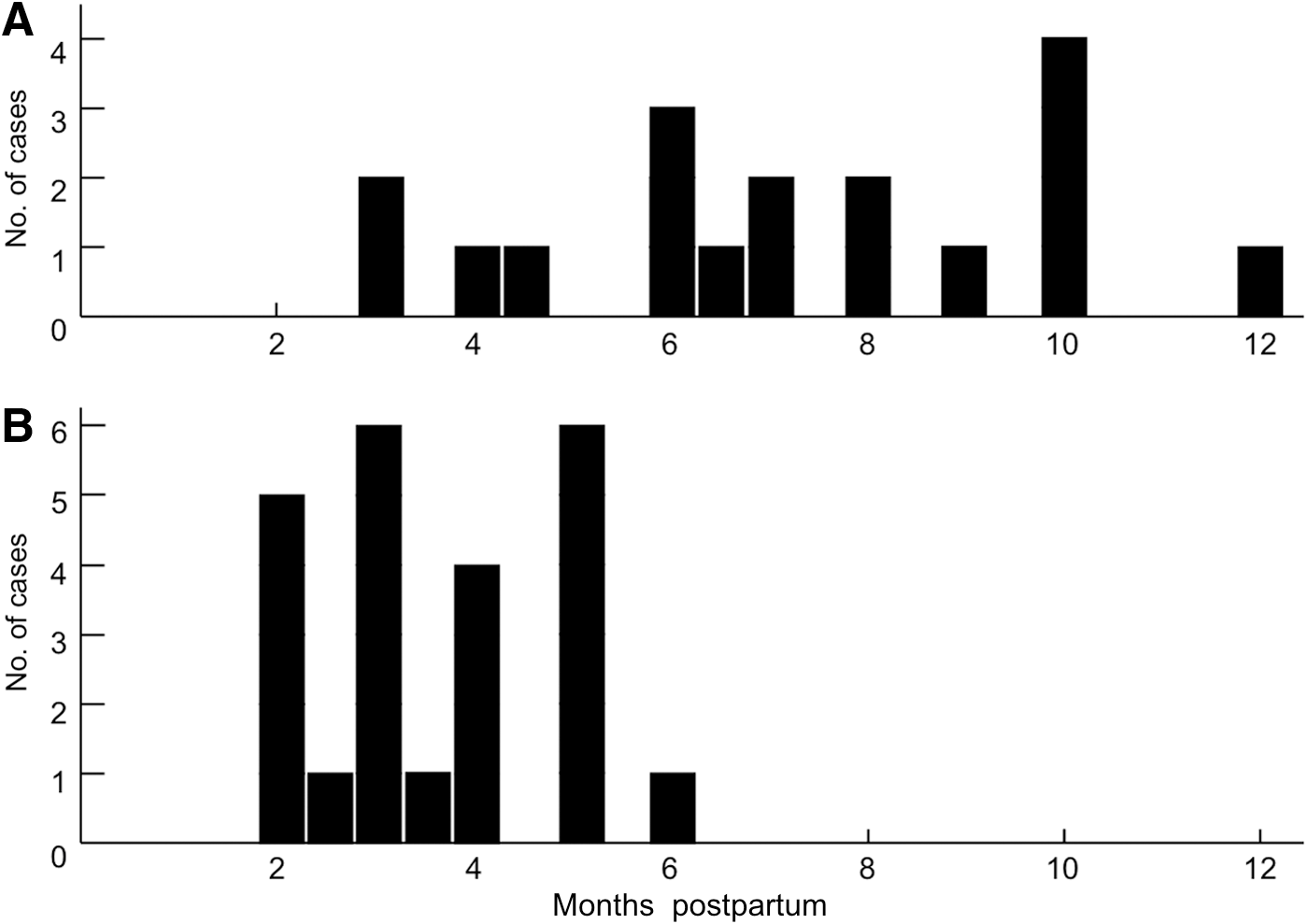
Onset time of postpartum Graves' thyrotoxicosis (
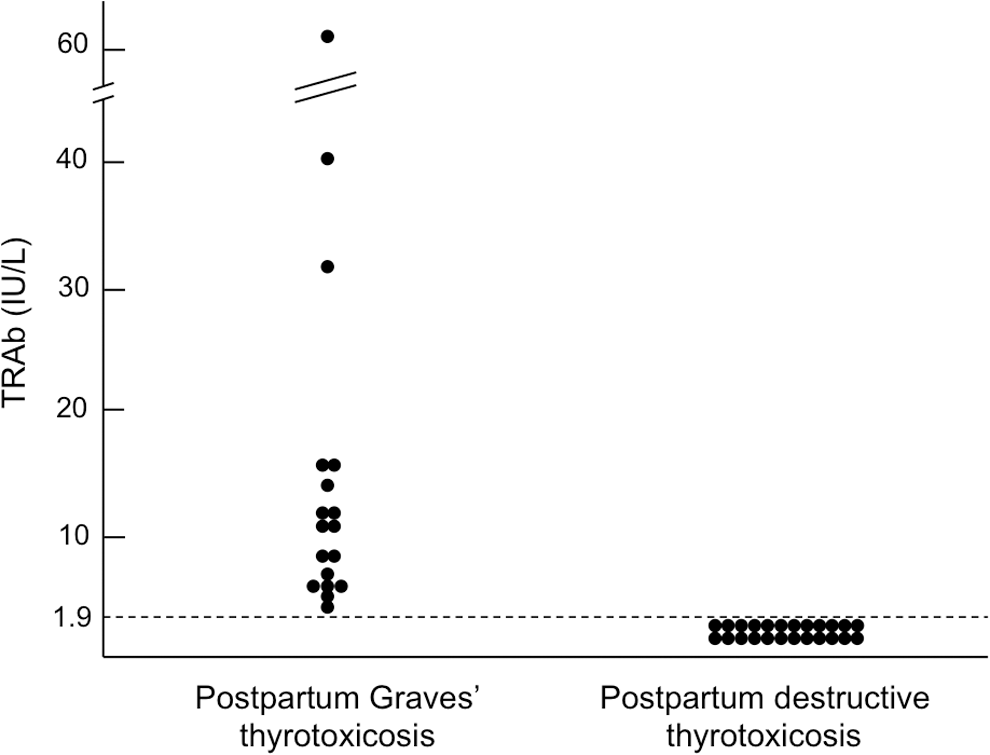
Comparison of antithyrotropin receptor antibodies (TRAb) between postpartum Graves' thyrotoxicosis and postpartum destructive thyrotoxicosis.
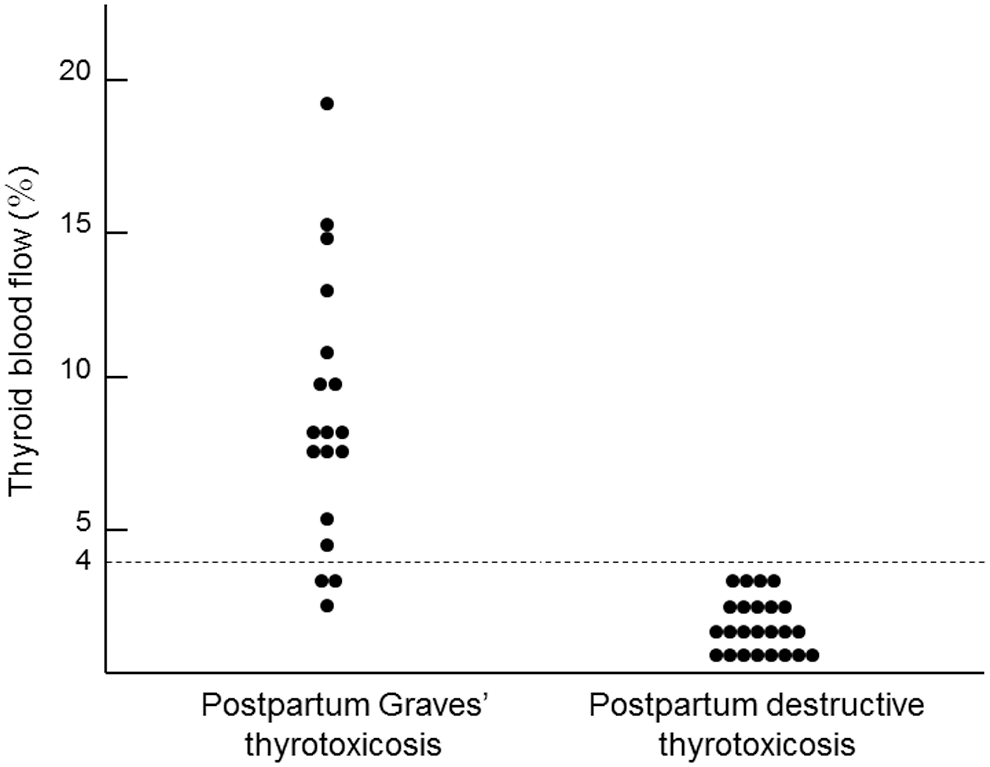
Comparison of thyroid blood flow between postpartum Graves' thyrotoxicosis and postpartum destructive thyrotoxicosis.
Undetectable levels of TRAb, TgAb, and TPOAb <1.3 IU/L, 39.9 IU/mL, and 27.9 IU/mL were respectively calculated as 1.3, 39.9, and 27.9. fT3, free triiodothyronine; fT4, free thyroxine; TRAb, anti-TSH receptor antibodies; TgAb, antithyroglobulin antibodies; TPOAb, antithyroid peroxidase antibodies.
Serum fT4 and fT3 were significantly higher in patients with PPGr, and the serum fT3/fT4 ratio was also significantly higher in PPGr than in PPDT (Table 1), but absolute values overlapped somewhat between the two. Thirteen (72.2%) of 18 PPGr patients and 21 (87.5%) of 24 PPDT patients had positivity for TgAb. In addition, 10 (55.6%) of 18 PPGr patients and 11 (45.8%) of 24 PPDT patients had positivity for TPOAb. There was no significant difference in thyroid volume and the levels of TgAb and TPOAb between patients with PPGr and PPDT.
Discussion
Most postpartum thyroid dysfunctions occur due to exacerbation of subclinical autoimmune thyroiditis. The postpartum autoimmune thyroid syndrome is defined as a type of thyroid dysfunction, including Graves' disease and Hashimoto's thyroiditis, newly occurring during the postpartum period in individuals who have no previous experience of thyroid dysfunction (1). It often manifests as transient thyrotoxicosis (destructive thyrotoxicosis), but some cases involve persistent thyrotoxicosis (Graves' disease). This is the first study in which a sensitive third-generation TRAb assay combined with quantitative measurement of TBF could confirm the differential diagnosis of postpartum thyrotoxicosis.
We classified postpartum thyroid dysfunctions into five categories: (I) persistent thyrotoxicosis, (II) transient thyrotoxicosis, (III) destructive thyrotoxicosis followed by transient hypothyroidism, (IV) transient hypothyroidism, and (V) persistent hypothyroidism (1).
The prevalence of postpartum thyroid dysfunction is approximately 5–10% in the general population (6). The prevalence of postpartum Graves' disease (both persistent and transient) is estimated at 11% of those with postpartum thyroid dysfunction (7). Destructive transient thyrotoxicosis is the most prominent form of postpartum thyroid dysfunction, accounting for 50–60% of all thyroid dysfunction (7).
It is reported that thyrotoxicosis in postpartum Graves' disease (PPGr) usually occurs at four to six months postpartum; on the other hand, destructive thyrotoxicosis develops at one to three months postpartum (1). In this study, we also found that PPGr occurred later than PPT (7.2 months vs. 3.6 months). In the early postpartum period, Th1 immune reaction is predominant, and this condition is associated with tissue destruction. Subsequently, Th2 immune reaction becomes predominant and is often associated with the production of autoantibodies, including TRAb (1).
Thyroid scintigraphy with radioiodine may be used to differentiate between Graves' disease and destructive thyrotoxicosis, but the use of 131I is contraindicated in lactating patients. Although 123I and 99mTc are alternative scanning substances, they still require interruption of lactation for a couple of days. Up to 20% of cases are labeled as hyperthyroidism of indeterminate origin (14,15).
For differentiation of the two types of thyrotoxicosis, we previously reported on the T3/T4 ratio (16). Recently, using the fT3/fT4 ratio, a significant difference between Graves' disease and painless thyroiditis was found (17). Similar results were obtained in this study, but there was marked overlap of individual values between the two groups. Therefore, this parameter is not useful for exact differentiation.
TRAb estimation has proved to be the most sensitive tool to identify individuals with Graves' disease. TRAb can be measured by competitive binding assays, which have developed further and had their accuracy improved over the past 15 years (18,19). A third-generation commercial TRAb assay was introduced by Smith et al. (20). Furthermore, a new rapid and fully automated electrochemiluminescence immunoassay for the determination of TRAb based on the ability of TRAb to inhibit the binding of a human thyroid-stimulating monoclonal antibody (M22) has been established (9). This assay system has high sensitivity for detecting Graves' disease without loss of specificity (9). In this study, all patients with PPGr were TRAb positive; on the other hand, all patients with PPT were negative for TRAb. For this reason, TRAb is the most sensitive test to differentiate postpartum thyrotoxicosis (Fig. 2). Moreover, regarding titers of TRAb, we found that they are relatively low (mean TRAb 14.9 IU/L; Fig. 2). This means that patients with PPGr were diagnosed in the early phase of the disease. Ultrasonography is a noninvasive, cost-effective (at least in Japan), and widely available diagnostic tool. We previously established a new technique of measurement for TBF. We found that there is a high correlation between TBF and RAIU at 3 or 24 hours, that is, the measurement of TBF is a reliable alternative to RAIU tests to identify the cause of thyrotoxicosis (11). Advanced dynamic flow was developed in high-resolution power Doppler mode. A previous study clearly differentiated Graves' disease from the destructive forms of thyrotoxicosis with a cutoff value of 4.0% (10). In this study, there were three patients with PPGr who had TBF values <4.0% (3.8%, 2.8%, and 3.0%). Their times of onset of thyrotoxicosis were three, three, and six months postpartum respectively. These data strongly suggest that a very early stage of PPGr may not be associated with an increase of TBF.
In conclusion, postpartum early onset (within three months) of thyrotoxicosis was associated mainly with PPDT, and late onset (more than 6.5 months) was suggestive of PPGr. Positive TRAb and high TBF >4.0% indicate postpartum onset of Graves' disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.