
Abstract
Objective:
The purpose of this study was to develop a novel open-window needle aspiration method and evaluate its efficacy in drainage and sclerotherapy of cystic thyroid nodules that cannot be aspirated with an 18-gauge needle.
Methods:
Two rectangular windows 5.0 mm in length and 1.0 mm wide were placed at the end of the percutaneous transhepatic cholangiography (PTCA) needle trocar to develop a new open-window intervention needle. The efficiency of the open-window intervention needle was compared either to a porous interventional needle or to an ordinary PTCA needle by assessing the aspiration efficiency. The efficacy of the modified open-window approach was tested by carrying out sclerotherapy and drainage on 21 thyroid cystic nodules that could not be aspirated with an 18-gauge needle and comparing it to aspiration with an 18-gauge PTCA needle of 50 cystic thyroid nodules.
Results:
The efficacy of aspirating coupling agents of various specifications using the new open-window intervention was superior to aspiration using the PTCA trocar needle or a porous needle (p<0.05). Ethanol ablation efficacy in the treatment of 21 cystic thyroid nodules that could not be aspirated with an 18-gauge needle and the aspiration efficacy of 50 cystic thyroid nodules with an 18-gauge PTCA needle were not significantly different (p>0.05).
Conclusion:
The new open-window intervention needle approach was highly effective in conducting ethanol ablation of cystic thyroid nodules that could not be aspirated using conventional methodologies.
Introduction
N
Materials and Methods
Development of an open-window intervention needle
The open-window intervention needle was generated by drilling two rectangular windows 5.0 mm in length and 1.0 mm in width at the end of a percutaneous transhepatic cholangiography (PTCA) trocar (Patent no.: 201220323579.1, China; Fig. 1). The aspiration efficiency of the open-window needle was assessed by comparing aspiration of a coupling agent to aspiration observed for different gauge needles (14-, 16-, and 18-gauge needles with a stem length of either 7 or 13 cm), a porous puncture needle, or an ordinary PTCA needle. Aspiration efficiency was defined by the time required to aspirate 5 mL of the coupling agent by the different needles when connected to 50 mL syringes under maximum negative pressure.
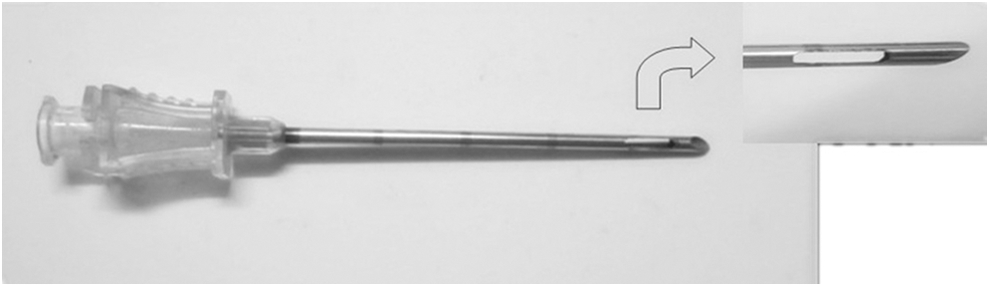
Schematic diagram of the open-window intervention needle.
Patient enrollment
The protocol for this prospective study was approved by the Institutional Review Board, and informed consent was obtained prior to the review of images and medical records. All patients undergoing ultrasound-guided fine-needle aspiration biopsy (FNAB) and EA provided written informed consent before each procedure.
Between October 2011 and December 2013, 71 patients with cystic nodules (predominantly cystic thyroid nodules) were treated by EA at The Second Affiliated Hospital of Fujian Medical University. Eleven patients were male and 60 were female, and they were aged between 26 and 57 years (M age=42.5 years). In 50 cases, fluid was successfully aspirated using an 18-gauge needle. However, 21 cysts could not be aspirated in this manner (or the volume of liquid aspirated was <0.5 mL).
The inclusion criteria were (i) presentation with a single cystic or predominantly cystic nodule (<50% solid), and (ii) cosmetic or pressure problems. Exclusion criteria included (i) suspicion of malignant cystic nodules confirmed by FNAB; (ii) a history of neck irradiation; (iii) presence or suspicion of multiple endocrine neoplasia types 1 or 2; (iv) a family history of thyroid cancer; and (v) previous sclerotherapy treatment.
Pre-ablation assessment
The following three indicators were used to evaluate treatment efficacy: (i) symptom ranking by Visual Analogue Scale (VAS) before and after treatment; (ii) physician assigned cosmetic grading scores (1, no palpable mass; 2, no cosmetic problem but palpable mass; 3, a cosmetic problem on swallowing only; and 4, a readily detected cosmetic problem); and (iii) cyst volume. Each of the three orthogonal diameters of the lesion (the largest diameter and two other mutually perpendicular diameters) where measured using a 7.5 MHz linear probe using a real-time ultrasound system (Prosound LOGIQ P6; GE Healthcare) and the volume of each lesion was calculated using the following equation: V=π abc/6, where V is the volume, a is the largest diameter, and b and c represent the other two diameters. A three-dimensional ultrasound was also conducted using a Voluson 730 Expert (GE Healthcare) ultrasound system equipped with a RAB 6–12 L probe (General Electric, United States) and virtual organ computer-aided analysis (VOCAL) software.
Procedures
Patients were placed in a supine position with mild neck extension. All procedures were carried out under ultrasound guidance. After skin sterilization and application of anesthesia (2% lidocaine at the puncture site), an 18-gauge needle was gradually inserted through the epidermis to the thyroid pericapsular space using the transisthmic approach (11 –16). When the needle reached the center of the cyst, the needle core was removed, and aspiration was carried out with a 20 mL syringe. Quantification of negative pressure was unnecessary, as it is more important to adjust the negative pressure according to the rate of aspiration. As much fluid as possible was aspirated, followed by repeated irrigations with isotonic saline until the cyst was drained. Then, 99% anhydrous alcohol was injected into the cysts and repeated washings were carried out (two or more as needed) until the aspirated liquid was clear. The volume of isotonic saline or alcohol injected into the cysts equaled the volume removed each time. Injected anhydrous alcohol was retained within nodules for about 10 min. The volume of alcohol utilized in the treatment of thyroid cysts was at least 1–1.2 times the volume of the respective cyst. Sclerotherapy efficacy was improved by puncturing solid portions of the cyst in multiple directions. If the liquid could not be aspirated, the modified 18-gauge open-window needle procedure was used (Fig. 2). Patients remained in the hospital for 30 min after the procedure.
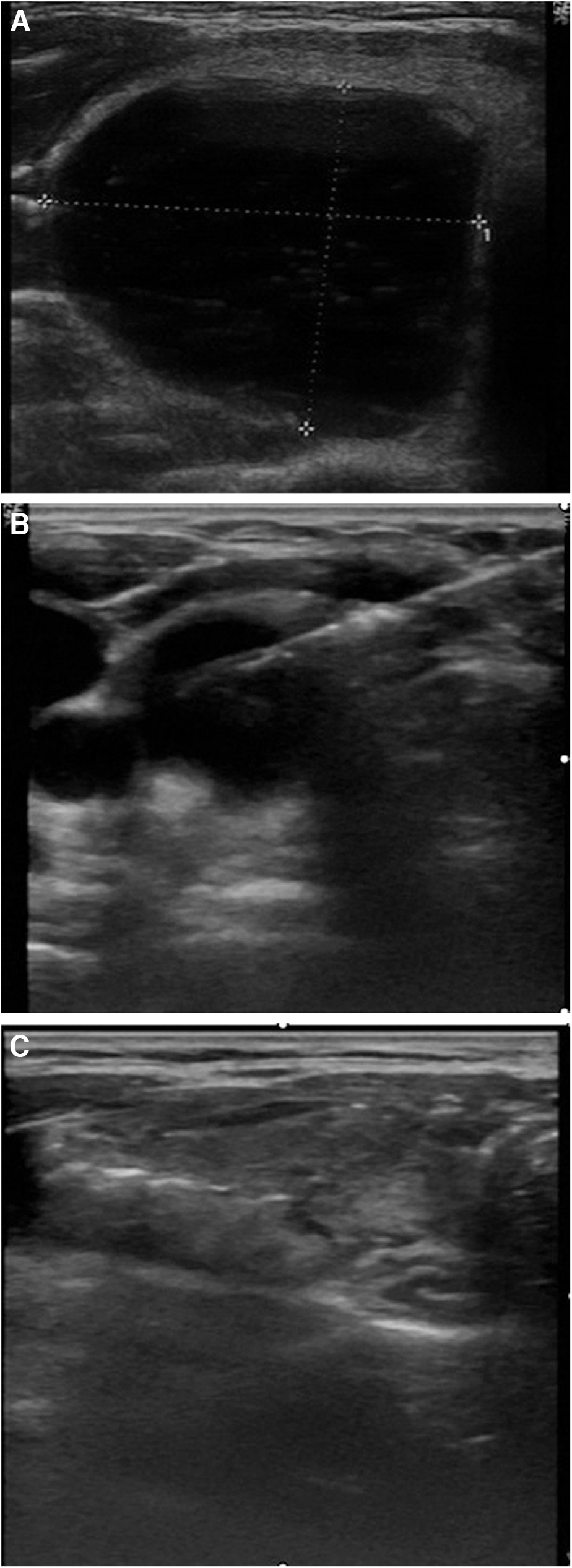
Thirty-year-old man with a colloidal cyst.
Statistical analysis
All statistical analyses were performed using the SPSS statistical software package v17.0 for Microsoft Windows (SPSS, Inc., Chicago, IL). Paired t-tests were used to compare aspiration efficiency. Mann–Whitney and Fisher's exact tests were used to compare sex distribution, age, duration of follow-up, initial nodule volume, and symptom and cosmetic scores between groups before treatment. Wilcoxon's signed-rank test was used to assess differences in volume reductions, symptoms, and cosmetic scores between groups, and to evaluate the therapeutic success and differences in the number of treatment sessions between groups. The level of significance was defined as p<0.05.
Results
Efficiency analysis of the various aspiration methods demonstrated that the new open-window intervention needle was superior compared to both the PTCA trocar and porous needles. Furthermore, aspiration efficiency was improved when the inner diameters were larger or needles were shorter (p<0.05; Table 1).
Data were the numerical value of the time required to aspirate 5mL of the coupling agent by the different needles when connected to 50 mL syringes under maximum negative pressure and the time accurate to the seconds. Data are expressed as the mean±standard deviation (SD) unless otherwise indicated.
Comparison of the same gauge of the same kind of needle.
Comparison of the same length of the same kind needle.
Open-window intervention long or short needle vs. ordinary PTCA long or short needle and the porous interventional long or short needle: * p<0.05, ** p<0.01.
PTCA, percutaneous transhepatic cholangiography.
Patients were divided into either the aspiration or nonaspiration group. Before treatment, there were no significant differences between the groups with respect to clinical or demographic parameters, including sex (p=0.86), age (p=0.43), follow-up period (p=0.30), nodule volume (p=0.94), symptom scores (p=0.30), or cosmetic scores (p=0.45; Table 2). Changes in nodule volume, symptom scores, and cosmetic scores at each follow-up visit in the treatment groups are described in Figures 3 –5, respectively. We observed significant decreases in nodule volume (p<0.001), symptom scores (p<0.001), and cosmetic scores (p<0.001) between the initial and the last follow-up visit in either group.

Efficacy of nodule ablation. Thyroid nodule volumes of two treatment groups before ablation; one, three, and six months after ablation; and at the last follow-up. Significant decreases in nodule volume (p<0.001) were observed between pre-ablation and at the last follow-up for both groups.

Efficacy of treatment on symptom scores. Symptom scores of the two treatment groups before ablation; one, three, and six months after ablation; and at the last follow-up. Significant decreases in symptom scores (p<0.001) were observed between pre-ablation and at the last follow-up in both groups.
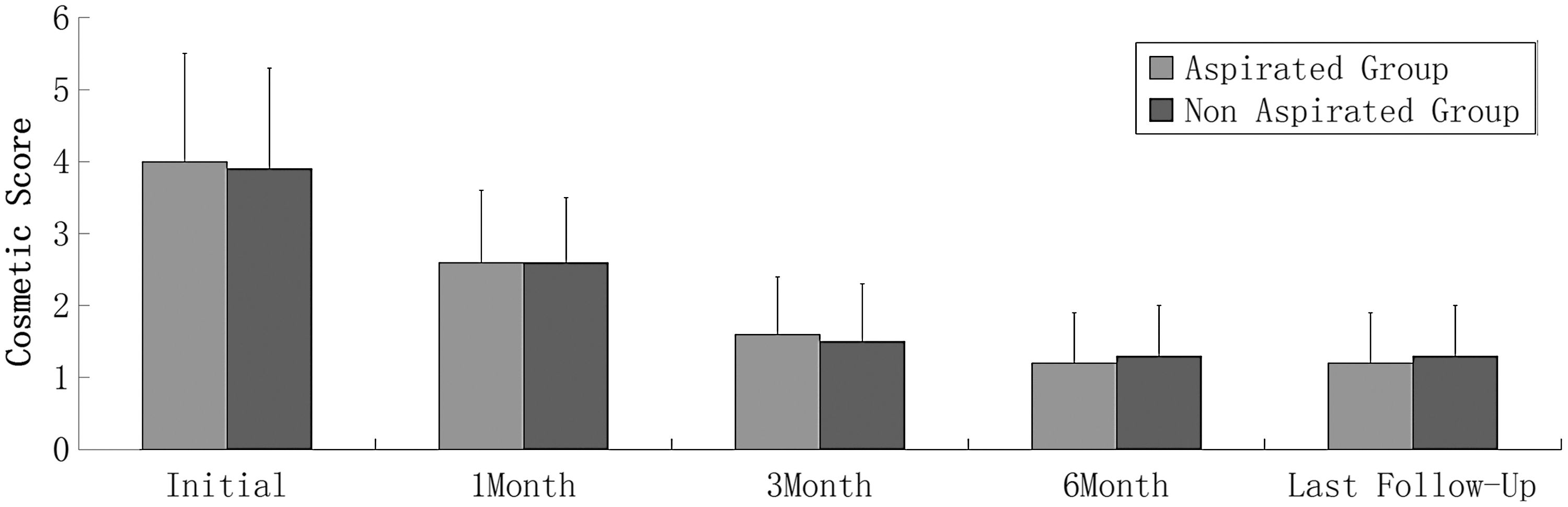
Efficacy of treatment on cosmetic scores. Cosmetic scores of the two treatment groups before ablation; one, three, and six months after ablation; and at the last follow-up. Significant decreases in cosmetic scores (p<0.001) were observed between pre-ablation and at the last follow-up in both groups.
Except for the number of men and women and p-values, data are expressed as the mean±SD (range).
The effects of the different treatments on the respective groups are described in Table 3. There were no differences between groups with regard to mean volume reduction (p=0.31), decrease in symptom scores (p=0.68), decrease in cosmetic scores (p=0.65), therapeutic success rates (p=0.61), or the mean number of treatment sessions (p=0.25).
Except for therapeutic success rates and p-values, data are expressed as the mean±SD (range). There were no major complications in either group.
VRR, volume reduction rate; VAS, visual analog scale.
No serious complications, including voice changes, skin burning, infections, or damage to vital neck structures were observed in either group. During EA, patients experienced only mild pain associated with needle puncture and removal.
Discussion
This report describes the development and testing of a new approach for the treatment of cystic thyroid nodules. There has been much research regarding the treatment of cystic nodules, specifically the use of the percutaneous ethanol injection technique developed in the early 1990s that has been successfully used for the treatment of cystic thyroid nodules (7,17). Previous studies have reported that EA was 85–98.5% effective in the treatment of cystic nodules (10,18 –22), 64–73.2% effective in treating predominantly cystic nodules (14,23), and 38–47% effective in the treatment of solid nodules (14,24). Therefore, EA has been recommended as a first-line treatment for benign cystic and predominantly cystic thyroid nodules (5).
One particular type of cystic nodules that is difficult to treat are the viscous cystic thyroid nodules that account for approximately 30% of cystic thyroid nodules (11) and that are defined as nodules that cannot be aspirated with an 18-gauge needle. Other difficult to treat nodules include a unique cyst with a spongiform appearance defined by the presence of multiple microcystic components and nodules with segmented solid components that are difficult to aspirate. Traditionally, cystic thyroid nodules have been treated using EA. However, this treatment is less effective in the treatment of viscous cystic thyroid nodules and nodules with segmented solid components compared to the efficacy observed in the treatment of serous cystic nodules because EA efficacy depends on the amount of aspirated fluid and its even tissue distribution (12). Therefore, a two-stage EA technique has been used to treat viscous cystic thyroid nodules (9,10). During the first stage, 95% sterile ethanol is injected into the nodule (1 mL per 10 mL of nodule volume) to dilute the nodule fluid. During the second stage (two to four weeks later), the cyst fluid is aspirated, and ethanol is injected. This approach is based on observations by Cho et al. (21) who demonstrated that repeated ethanol instillations diluted the cyst fluid making it easier to aspirate. However, these methods have drawbacks, including the number of instillations required and the amount of time required to complete the treatment (8). Moreover, if 95% sterile ethanol is injected into the nodule to treat nodules containing viscous cystic fluid and this fluid is not completely aspirated, the remaining fluid can develop into a coagulable colloid that cannot be absorbed, or it can generate small concretions that may easily block the needle. Sung et al. (8) described an effective one-step EA technique using either a 16-gauge needle or a 8.5 F pigtail catheter with negative pressure to aspirate cystic mucous from a thyroid nodule. However, this method was very time-consuming (an average of about 1.5 h) and was associated with an increased risk of complications such as hemorrhages or ethanol leakage due to the use of a large-bore needle. Treatment of viscous cystic nodules with spongiform appearance was less effective using either a one- or two-step EA procedure.
Regardless of whether ethanol, radiofrequency, or microwave ablation is used, it is critical that all cystic fluid be aspirated for therapy to be successful. Since these techniques are sometimes associated with incomplete aspiration, we developed a novel open-window interventional needle with the goal of solving these problems. Data presented in this study demonstrate the superior aspiration efficiency of the open-needle approach compared to the aspiration efficacy observed for the PTCA needle or the porous puncture needle, suggesting that the short open-window intervention needle (7 cm) should be the first choice for sclerotherapy of thyroid cystic nodules. Clinical application of the open-needle approach confirmed the efficacy of the novel open-needle sclerotherapy approach for the treatment of thyroid cystic nodules that cannot be aspirated with an 18-gauge needle.
Furthermore, the open-needle approach was more effective in carrying out EA therapy for the treatment of thyroid cystic nodules that could not be aspirated with an 18-gauge needle. There were no differences in treatment efficacy if the thyroid cystic nodule could be aspirated with an 18-gauge PTCA needle (p>0.05). Based on data presented in this report, the open-window approach has the following advantages. First, the new open-window needle is not easily obstructed by necrotic tissue or concretions. In addition, since the open window width is significantly smaller than the diameter of the needle, it serves as a filter. Second, this approach is conducive for the aspiration of multilocular cystic neoplasms because the needle has two different channels and a long strip window, making it less likely to become blocked. Third, the shorter needle improved the liquid extraction efficiency using needles of two different lengths (7 cm and 13 cm), both much shorter than the corresponding PTCA needle (20 cm). Finally, the window at the end of the needle tip is a long strip that increases the odds of the ethanol reaching the tissues of a multilocular cyst during EA procedures.
Moreover, during EA, repeat irrigation with isotonic saline was carried out until the colloid suspension disappeared completely, followed by EA therapy. This diminished the risk of coagulation that could block the needle, and at the same time increased the sclerotherapy efficacy. Although we used a relatively large amount of ethanol, there were no complications or requests by the patients to stop the procedure, probably due to our use of a transisthmic approach that minimized perithyroid leakage that represents a frequent cause of pain during EA (25). In conclusion, we recommend this new open-window intervention needle approach for effectively carrying out EA of cystic thyroid nodules that cannot be aspirated with an 18-gauge needle. Clinical trials with more patients will be needed to assess the validity of this approach further.
Footnotes
Acknowledgments
This study was supported by grants from the Key Program of Scientific Research of Fujian Medical University, Quanzhou, China (No. 09ZD015) and the National Natural Science Foundation of China (81271587).
Author Disclosure Statement
No competing financial interests exist.