
Abstract
Background:
Thyroid dysfunction is a common adverse event associated with tyrosine kinase inhibitors (TKI), but its underlying pathophysiology is unclear. Cabozantinib is a novel TKI currently Food and Drug Administration approved for advanced medullary thyroid cancer and tested in clinical trials on solid tumors including prostate, liver, bladder, breast, and ovarian cancer.
Methods:
We analyzed the thyroid function of patients enrolled in two phase 2 clinical trials using cabozantinib at the National Institutes of Health Clinical Center. Two cases of thyroiditis associated with cabozantinib therapy are presented in detail, and a systematic review of the literature on TKI-associated thyroid dysfunction is also discussed.
Results:
Between September 2012 and September 2013, 33 patients were treated with cabozantinib, and follow-up thyroid function tests were available for 31 (20 males, 11 females; age 59±1 years). Thyroid dysfunction was recorded in the majority of patients (93.1%), with a predominance of subclinical hypothyroidism. Two cases showed a biphasic pattern of thyroid dysfunction characterized by a transient thyrotoxicosis followed by hypothyroidism. Color Doppler demonstrated an increase in vascularization during the thyrotoxic phase, but no uptake was visualized on nuclear medicine imaging. A systematic review of the literature resulted in the identification of 40 original manuscripts, of which 13 were case series and 6 were case reports describing TKI-associated thyroid dysfunction.
Conclusion:
TKI therapy often results in clinically significant thyroid dysfunction. Cabozantinib treatment commonly results in thyroid dysfunction varying from subclinical hypothyroidism to symptomatic thyrotoxicosis. Early detection and characterization of cabozantinib-associated thyroid dysfunction and close follow-up are essential to provide adequate management of this common adverse event.
Introduction
T
Cabozantinib is a new multitargeted TKI that inhibits the tyrosine kinase activity of vascular endothelial growth factor receptors 1, 2, and 3 and MET, as well as a variety of other proto-oncogenes (RET, KIT, TRKB, FLT-3, AXL, and TIE-2). This agent was recently approved for the treatment of progressive, metastatic medullary thyroid cancer and is currently being evaluated in clinical trials for the treatment of prostate, ovarian, bladder, brain, melanoma, breast, non-small cell lung, pancreatic, hepatocellular, and renal cell cancer. In this report we present two illustrative cases of transient thyrotoxicosis associated with the treatment with cabozantinib and the prevalence and characteristics of cabozantinib-associated thyroid dysfunction in patients followed at the National Institutes of Health (NIH) Clinical Center.
Patients and Methods
We reviewed retrospectively all thyroid function tests available in patients enrolled in two nonrandomized, open label, single agent, phase 2 clinical trials using cabozantinib for the treatment of metastatic bladder cancer (NCT01688999) and metastatic soft tissue sarcoma (NCT01755195) at the NIH Clinical Center in Bethesda Maryland. Cabozantinib was administered at the dose of 60 mg daily in 28-day cycles in both the trials to assess antitumor activity by determining the objective response rate. Baseline thyroid function was assessed on patients enrolled in these trials, and thyroid dysfunction history was not an exclusion criterion as long as the patients were adequately treated at enrollment. All patients provided written informed consent for the participation in the respective studies. Two cases of cabozantinib- associated thyroiditis are described for illustrative purposes, and their serial changes in thyroid function and imaging are reported.
A systematic review of the literature for the period ranging from 2005 to 2013 was performed in PubMed using the following terms: “tyrosine kinase inhibitor” and “thyroid dysfunction” or “thyroiditis” or “hyperthyroidism” or “hypothyroidism.” The search was then limited to English language and to original reports or case series describing features of thyroiditis and/or thyrotoxicosis. Reports describing exclusively hypothyroidism associated with TKI use were not included in the analysis. Additional references were retrieved by cross-referencing and reviews.
Results
Between September 2012 and September 2013, a total of 33 patients were enrolled in two trials. Twenty-three patients affected by metastatic bladder cancer (16 male and 7 female; age 62±8.4 years) were treated with cabozantinib for 107±83 (range: 10–308) days. Ten patients (5 female, 5 male; age: 50.5±11 years) affected by metastatic soft tissue sarcomas received cabozantinib for 78±55 (range: 4–196) days. All patients had at least a baseline serum thyroid stimulating hormone (TSH) value. Two patients had no follow-up thyroid function tests and were excluded from the analysis. The summary of the data are reported in Table 1. Two patients were affected by primary hypothyroidism at the time of enrollment; one was profoundly hypothyroid and required a dose increase at the beginning of the study; the second patient was euthyroid on levothyroxine treatment at the beginning of the treatment with cabozantinib; however, after 4 weeks of therapy, a rise in TSH was observed (from 0.64 to 7.6 mIU/L). These two cases were excluded from the subsequent analysis.
Case 1 and Case 24 are reported in the text.
Patients 10 and 21 were treated with levothyroxine before enrolling in the cabozantinib trials.
No follow-up thyroid function tests were available for patients 13 and 29 (see text for details).
At the time of enrollment in the trial, Case 23 had untreated subclinical hypothyroidism that progressed to frank hypothyroidism following the cabozantinib therapy.
FT4, free thyroxine; NA, not available; TSH, thyroid stimulating hormone.
Thyroid dysfunction was observed in 27 of the remaining 29 patients (93.1%). In two patients, the thyroid function remained normal after 42 and 120 days of therapy respectively. Thirteen patients (44.8%) developed subclinical hypothyroidism (TSH>4.0<10 mIU/L) and eight patients (27.6%) developed overt hypothyroidism and were prescribed levothyroxine treatment. Thyroiditis with varying degrees of documented transient thyrotoxicosis was diagnosed in 5 patients (17.2%); three out of these five patients eventually developed hypothyroidism and required levothyroxine treatment. In total, 11 patients (37.9%) developed frank hypothyroidism (Table 1) requiring levothyroxine therapy.
The literature search for TKI-induced thyroid dysfunction resulted in 40 original manuscripts, of which 13 were case series and 6 were case reports. The manuscripts reporting thyrotoxicosis (transient or prolonged) or thyroiditis are summarized in Table 2.
TKI, tyrosine kinase inhibitor.
Case Reports
Case 1
A 53-year-old woman with metastatic bladder cancer (Table 1; patient 1) developed neck pain and palpitations, heat intolerance, fatigue, nausea, generalized pain, and malaise after 2 weeks of cabozantinib. Her symptoms gradually intensified. On week 3 of therapy, her physical exam was significant for sinus tachycardia (120–130 beats/min), a weight loss of 6 pounds, warm skin, and hyperactive reflexes. Her TSH was 0.01 mIU/L (0.4–4.0), total triiodothyronine (T3) 394 ng/dL (90–215), and free thyroxine (FT4) 4.4 ng/dL (0.8–1.5). Thyrotropin receptor antibodies were not detected. The erythrocyte sedimentation rate was 83 mm/h. An 18F-Fluorodeoxyglucose Positron Emission Tomography scan performed as part of her staging demonstrated homogenous intense uptake in the anterior neck, while an ultrasound (US) showed a slightly enlarged thyroid with diffuse hypervascularity without any nodules. The differential diagnosis included Graves' disease versus subacute thyroiditis.
After one week, in spite of discontinuation of TKI therapy and supportive therapy with ibuprofen and propranolol, her thyrotoxicosis worsened. Since the patient underwent multiple computed tomography (CT) scans in the previous month, a Technetium 99-m (99mTc) pertechnetate thyroid scan was performed to overcome the iodine overload. The scan demonstrated no thyroid uptake, confirming the diagnosis of TKI-induced subacute thyroiditis. The patient was treated with high-dose prednisone, cholestyramine, and propranolol with clinical and biochemical improvement over the next 10 days. Her thyroid hormone levels normalized over 10 weeks: TSH 0.54 mIU/l, T4 9.5 mcg/dL (4.5–12.5), and T3 108 ng/dL (Fig. 1). A follow-up thyroid ultrasound 4 weeks after the first ultrasound demonstrated normal gland size and vascularity.
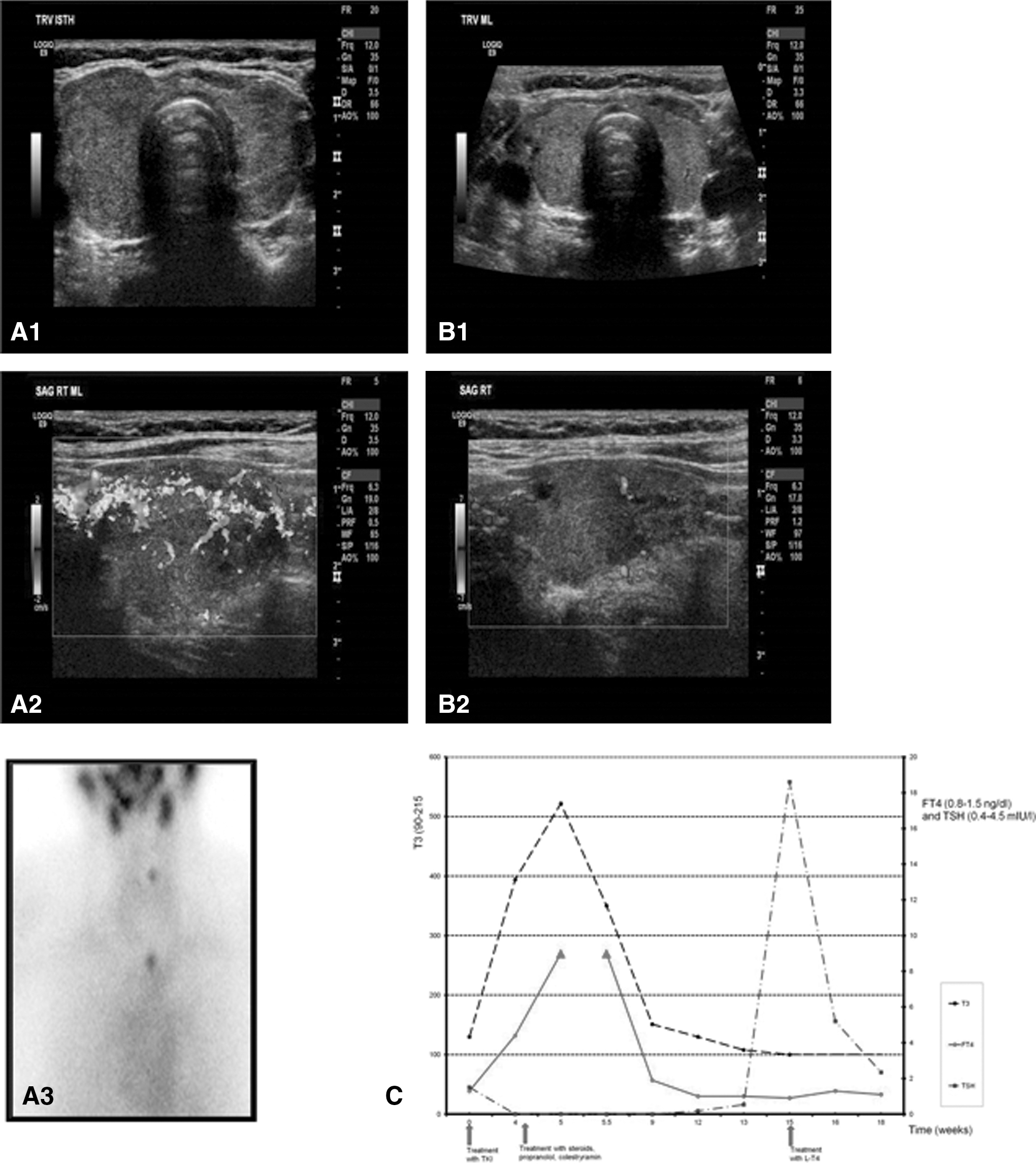
Case 1. Thyroid ultrasound, color Doppler:
On week 15 of therapy with cabozantinib, the patient developed hypothyroidism with a TSH of 18.6 mIU/L and a free T4 (FT4) of 0.7 ng/dL with mild symptoms of fatigue; she was started on levothyroxine therapy at the dose of 1.6 mcg/kg with resolution of the symptoms.
Case 2
A 69-year-old African American male with metastatic high-grade soft tissue sarcoma (Table 1, patient 24) of the thigh was enrolled in the phase 2 cabozantinib trial. Prior to TKI treatment, his thyroid function tests were normal. One month after the initiation of treatment, his TSH was 8.54 mIU/L with an FT4 of 0.8 ng/dL. In month 2, the TSH increased to 12.8 mIU/L with an FT4 of 0.9 ng/dL and a total T3 of 67 ng/dL (90–215 ng/dL) with negative thyroid antibodies. At that time, he was asymptomatic and treatment was deferred. Due to mild neutropenia, the cabozantinib dose was decreased to 40 mg. Four months after the start of cabozantinib, his thyroid function tests normalized with a TSH of 3.0 mIU/L and a FT4 of 1.3 ng/dL. In July 2013, his TSH was 0.11 mIU/L, with an FT4 of 1.6 ng/dL and a total T3 of 107. Two weeks later, the patient complained of fatigue, lack of appetite, and intermittent diarrhea despite the reduced dose of cabozantinib. He also noted palpitations; however, he denied any other symptoms suggestive for thyrotoxicosis. A repeated TSH was 0.03 mIU/L with FT4 of 1.6 ng/dL and a total T3 of 121 ng/dL (Fig. 2). The patient had mild resting tachycardia (heart rate 108 bpm), his thyroid gland was of normal size, and no nodules were appreciated. A thyroid ultrasound demonstrated a thyroid gland with normal size and echostructure with a normal vascularity. A 99mTc pertechnetate thyroid scan showed no visible accumulation of tracer activity in the thyroid gland. The patient was treated with propranolol 10 mg three times daily and a short course of prednisone with resolution of the symptoms and normalization of the thyroid function tests in 3 weeks (TSH:0.59, FT4: 0.8).
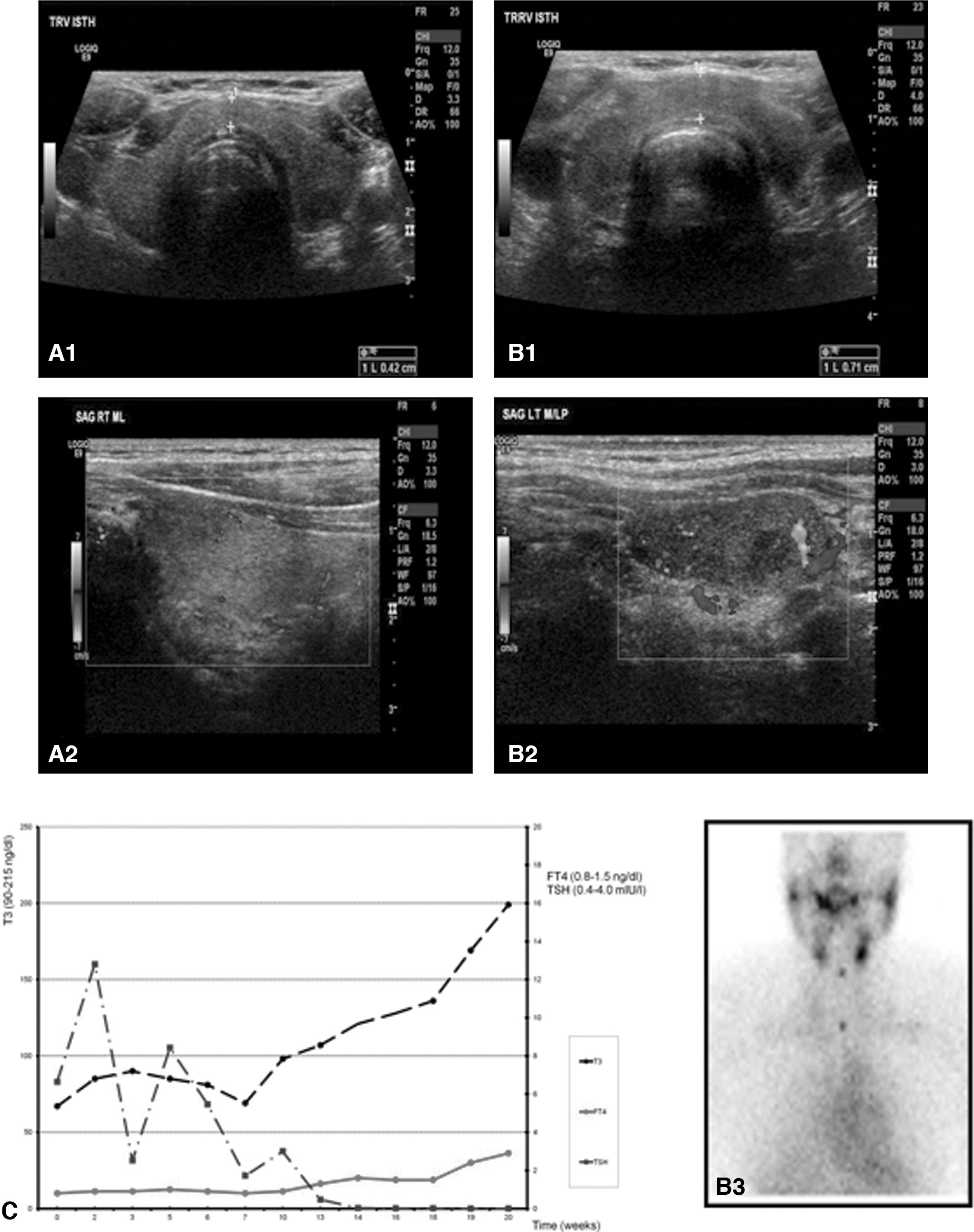
Case 2. Thyroid ultrasound, color Doppler:
Three other patients who have been treated with cabozantinib for metastatic bladder cancer demonstrated similar thyroid dysfunction patterns (Table 1).
Discussion
In this report, we analyzed the prevalence of thyroid dysfunction associated with the novel tyrosine kinase inhibitor cabozantinib in two ongoing phase 2 trials carried out at our institution. Similar to other TKIs, the prevalence of thyroid dysfunction associated with this drug is high (93.1%). To our knowledge, this is the first assessment of thyroid dysfunction occurring during the therapy with this specific agent; thyroid dysfunction is also described in the package insert for cabozantinib.
Thyroid dysfunction is a frequent adverse event observed during the treatment with TKIs (1,2). Although thyroid function abnormalities are common, limited information is available about the pathophysiology and the course of the disease. Various mechanisms have been proposed in the development of TKI-associated thyroid dysfunction: inhibition of iodide uptake (22), reduced synthesis of thyroid hormone (23), influence on deiodinase activity (24), impairment of transmembrane transport (27), direct damage to the thyroid gland via autoimmune processes (21,10), impaired blood flow and ischemia (9,26), or destructive thyroiditis (27). Interestingly, in some athyreotic patients treated with TKIs, the levothyroxine replacement dose required a substantial increase; this phenomenon might be secondary to poor absorption or concomitant use of antacids, and/or to comorbidities leading to non-thyroidal illness (28,29). Although some authors have argued that the inhibition of vascular endothelial growth factor receptors is the main mechanism of TKI-induced thyroid dysfunction (30), it is still unclear whether an agent-specific mechanism can be responsible for this phenomenon. Interestingly, some reports indicate that the development of hypothyroidism during TKI therapy correlates with favorable outcomes, suggesting that thyroid damage is a proxy for effectiveness of the drug (31). Indeed, patient 1, who had the most severe form of thyroid dysfunction in our series, had a remarkable response to cabozantinib, with resolution of many of her bone lesions, and she remained on the investigational trial for almost one year before progression occurred.
While the most common thyroid function abnormality is hypothyroidism (ranging from 36% to 85% in different reports) (1,30), cases of thyrotoxicosis have also been documented (6% to 44%) (21,27,30,16 –18). In some cases, the thyrotoxicosis is transient, followed by hypothyroidism and recovery to an euthyroid state, consistent with a form of destructive thyroiditis; however, hypothyroidism can also be permanent (19,32).
The first association between TKI therapy and hypothyroidism was noted in 2006 with sunitinib (4). Follow-up studies on sunitinib-associated hypothyroidism reported prevalences as high as 85% (33). Similarly, in two patients with sorafenib-induced thyroiditis/hyperthyroidism, this condition was demonstrated both biochemically and with ultrasound (12). Several reports have demonstrated the decrease in size of the thyroid as a sign of irreversible organ damage resulting in permanent hypothyroidism (16,34,35); therefore, it has been postulated that the transient thyrotoxicosis was due to a destructive thyroiditis, which may go unrecognized in a significant number of cases of TKI-induced hypothyroidism. The clinical course of the two patients described in this report is consistent with this proposed pathophysiologic mechanism, and clearly illustrates the dynamic changes in thyroid function and morphology during TKI-induced thyroid dysfunction.
The diagnostic imaging in the evaluation of TKI-induced thyroiditis is challenging because this condition is almost invariably observed in the context of iodine overload due to the iodinated contrast media used for the staging of the underlying disease. In fact, the patients described in this manuscript underwent multiple CT scans with intravenous contrast, and radioiodine could not be employed for functional thyroid imaging. We thus elected to use 99mTc scans to interrogate the activity of the gland. This tracer enters the thyroid cell via the sodium iodine symporter and it is sensitive and specific for the functional evaluation of the gland (36) and the characterization of amiodarone-induced thyrotoxicosis, which is a classic state of iodine overload (37,38).
The combination of color Doppler ultrasound and 99mTc scan has allowed us to document the acute phase of the thyroiditis in patient 1. Although the typical ultrasound findings of subacute thyroiditis are decreased gland size and vascularity (39), we observed a diffusely increased vascularity and increased gland size during the initial phase of thyrotoxicosis. These findings reverted when a follow-up ultrasound was performed four weeks later. Collectively, these data suggest that the timing of imaging studies is critical, and the results should be evaluated in the context of the onset of symptoms and changes in thyroid function. The observation of hypervascularity, coupled with a decreased 99mTc uptake while the patient was thyrotoxic, are consistent with an acute phase of tissue damage and hormonal leakage. This multimodal approach allowed us to establish a correct diagnosis and to avoid the empirical use of thionamides.
Conclusion
The specific mechanisms of action underlying cabozantinib- or other TKI-induced thyroid dysfunction are not clear. The symptoms associated with hypothyroidism or thyrotoxicosis are nonspecific and may overlap with the ones associated with the underlying malignancy and its therapy. A delay in the diagnosis of TKI-induced thyroid dysfunction may further worsen the quality of life and increase morbidity in already compromised and frail patients. Our findings suggest that patients undergoing cabozantinib therapy require assessment of the thyroid function at baseline and at least monthly during the follow-up to provide an early diagnosis and to guide the treatment of this common condition. To the best of our knowledge, this is the first report describing the features of cabozantinib-induced thyroid dysfunction in detail, although the prescribing information describes that increased levels of TSH were observed in 57% of medullary thyroid cancer patients receiving cabozantinib as compared with 19% of placebo patients. Our data indicate that this is an extremely common occurrence during treatment with this agent. In particular, the high prevalence of transient thyrotoxicosis secondary to destructive thyroiditis may pose a challenge in the initial evaluation of this condition. Since this is a relatively new agent, long-term follow-up of patients treated with cabozantinib will provide further information on the course of the disorder and the potential for recovery of thyroid function after discontinuation of the drug.
Footnotes
Acknowledgments
We are grateful for the help of the National Institutes of Health Clinical Center staff including nurses, clinical and research fellows, and study participants. This work was supported by the Intramural Research Program of the National Institute of Diabetes and Digestive and Kidney Diseases program Z01-DK047057-02, National Cancer Institute, and the Clinical Center, National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.