
Abstract
Background:
The spine is the most common site of bone metastases due to thyroid cancer, which develop in more than 3% of patients with well-differentiated thyroid cancer. Nearly half of patients with bone metastases from thyroid cancer develop vertebral metastases. Spinal metastases are associated with significantly reduced quality of life due to pain, neurological deficit, and increased mortality.
Summary:
Treatment options for patients with thyroid spinal metastases include radioiodine therapy, pharmacologic therapy, and surgical treatments, with recent advances in radiosurgery and minimally invasive spinal surgery as well. Therapeutic interventions require a multidisciplinary approach and aim to control pain, preserve or improve neurologic function, optimize local tumor control, and improve quality of life. We have proposed a three-tiered approach to the management and practical algorithms for patients with spinal metastases from thyroid carcinoma.
Conclusions:
The introduction of novel and improved techniques for the treatment of spinal metastases has created the opportunity to significantly improve control of metastatic tumor growth and the quality of life for the patients with spinal metastases from thyroid cancer. In order for these options to be effectively used, a multidisciplinary approach must be applied in the management of the patients with thyroid spinal metastases.
Introduction
B
Metastatic progression of TC is a multifaceted and complex process (5). The gene profile that conveys the potential for metastatic spread to bone may be expressed in TC cells early in carcinogenesis, or may be acquired later in the course of cancer progression, as a result of evolution of subclones of cancer cells that have undergone multiple episodes of cytogenetic and epigenetic alteration (5,6). Some cancer cells that disseminate early in the course of the cancer may remain dormant in their new location for a long time, becoming active only when their new microenvironment favors growth of the metastatic cancer cells (5,6). Biologically active mediators from the primary tumor may also promote development of favorable premetastatic niches, where colonization by dormant or newly arrived metastatic cells, will be supported (6). Within the bone tissue, metastatic cells can secrete factors that stimulate bone destruction, and the consequent release of numerous factors mobilized within the bony matrix that act on cancer cells promote a more aggressive tumor phenotype and potentiate cancer spread and bone destruction (7). Tumor cells and bone cells may rely on the same signaling pathways and transcription factors to facilitate their cooperative interactions at sites of metastases. This phenomenon has been suggested to represent “osteomimicry” on the part of the tumor cells (7,8). Metastatic progression at the metastatic site also requires tight interactions with immune cells, endothelial cells, and the stroma. Identification of intracellular pathways, mechanisms, and molecules responsible for progression of bone metastases may lead to the discovery of potential targets for therapy.
Current American Thyroid Association guidelines state that complete surgical resection of isolated symptomatic bone metastases can improve survival and should be considered, especially in patients <45 years old (9). A retrospective analysis of 202 cases of thyroid SMs revealed that almost half of patients with single-site SMs at the time of presentation do not have any other distant metastases and, therefore, may be considered for aggressive treatment of particular metastases (Kushchayeva et al., unpublished data). These features distinguish thyroid SMs from other primary cancers and provide an impetus for more aggressive therapy.
For the patients with advanced metastatic disease, new minimally invasive techniques may offer effective palliation of symptoms and mechanical stabilization with prevention or reduction of neurological complications. “Nevertheless the presence of distant metastases is not a justification for therapeutic nihilism but instead demands more aggressive therapy, with the hopeful expectation of improving outcome and prognosis” (10). Early detection of SMs is crucial because patient's outcome depends on the time of SM presentation. Patients presenting with initial distant bone metastases seem to have better outcomes compared to those who develop distant bone metastases after initial presentation (11,12).
Radionuclide Therapy
Radioiodine is the initial treatment of choice for patients with bone metastases from DTC if metastatic tumors are 131I avid. However, bone metastases may be unresponsive to radioiodine therapy. Positive uptake by bone metastases was reported in approximately half of the patients with bone metastases and complete responses to 131I treatment have been observed only in 30%–50% of those patients who have 131I avid metastases (2,13,14). To our knowledge, there are no publications specifically focused on the efficacy of 131I treatment of SMs. In general, the efficacy of 131I therapy depends on the volume of the metastatic tumor (15). Patients with small bone metastases that are not yet visible on radiographs, but that take up 131I on diagnostic scan, have better survival compared with patients with large symptomatic bone metastases (12). Hindié et al. (12) separately analyzed bone macro- and micrometastases. Macrometastases are generally not responsive to 131I and may require other approaches (1,12). The average survival of patients with non–131I avid bone macrometastases was 19.3 months, while for 131I-avid macrometastases survival was 49 months (12). There are at least two explanations for a better outcome in patients with 131I-avid macrometastases: the first is that 131I avidity implies a greater differentiation of the tumor and the second is the effective impact of radiation delivered by 131I (12). Moreover, radioiodine therapy may reduce the pain in unresectable bone metastases and even decrease the chances of developing neurologic deficits (16).
It appears that early diagnosis and repeated 131I therapy can be effective by targeting not only visible metastases but also those still too small to be imaged (17). The latter group includes metastases less than 3 mm, which is the typical threshold for magnetic resonance imaging detection (18). Early detection of metastases and administration of 131I seems likely to improve survival and quality of life in patients with bone metastases from DTC and the degree of 131I uptake is considered to be a prognostic factor in bone metastases (2,19). The role of 131I in control of residual tissue after resection for spinal macrometastases is unknown.
Usually radioiodine therapy is well tolerated. However, a case of radiation myelopathy 3 years after three courses of ablative 131I therapy for a patient with a thoracic spine metastasis from TC had been described (20). The patient underwent laminectomy and during the surgery, extensive epidural fibrous scar tissue (usually seen only after external radiation therapy) was found. Histological examination of the excised material from the affected vertebra showed extensive fibrous and necrotic tissue but no tumor cells (20). The authors suggested that the location of the metastatic lesion close to the spinal cord or even physical interaction with it may lead to the spinal cord injury by beta particles since they deposit the majority of their energy within 2 mm (20).
Protracted thyrotropin (TSH) elevation induced before 131I therapy by either thyroid hormone withdrawal or exogenously by administration of recombinant human TSH used in patients with TC metastases in confined spaces such as the brain or spine may cause clinically significant enlargement of the tumor size, with compressive or obstructive symptoms. The rate of neurological complications after recombinant human TSH and thyroid hormone withdrawal-aided 131I therapy for brain and spine metastases was similar (21).
Other radionuclude therapies include beta particle emitters (samarium-153 ethylene diamine tetramethylene phosphonate [153Sm-EDTMP], rhenium-186 hydroxyethylidenediphosphonate [186Re-HEDP], and strontium-89 [89Sr] chloride) and an alpha particle emitter (radium-223 [223Ra] dichloride). These agents deposit in areas of bone formation, and they therefore may be potentially used for blastic thyroid SMs.
Selective Embolization Therapy
In 1980 Camille et al. (22) were the first to describe preoperative embolization therapy for TC in four patients with TC metastases to the spine and pelvis. Selective embolization therapy can be used as a palliative treatment method or as a preoperative procedure to decrease the risk of hemorrhage during open surgery (16,23 –25). Metastases arising from TC are notoriously vascular (26). The goal in tumor embolization is not just to sacrifice the feeding vessel, but rather to obliterate the tumor capillary bed to the greatest extent possible. During this interventional procedure the arteries feeding the involved vertebra are visualized by selective catheterization. The tumor is starved of blood flow by embolizing the main tumor-feeding artery with repetitive small injections of polyvinyl alcohol foam particles of 150–250 μm diameter. Success of embolization is usually verified by angiography after the procedure (16,23,24).
The effect of palliative embolization therapy on thyroid bone metastases including spinal lesions has been investigated in four studies (16,23,24,27). Embolization of bone metastases including SMs was performed in patients with unresectable bone metastases 4–6 weeks after 131I ablation (25,27). Embolization has proven to be significantly more effective in combination with radioiodine and external radiation than embolization alone, providing temporary symptomatic relief for 15 and 6.5 months, respectively (27). In general, the most effective results are achieved during the first embolization session since the development of a collateral blood supply system has not occurred. Embolization has been associated with decreasing serum thyroglobulin (Tg) levels (16). However, based on serum Tg measurements taken weeks after this therapy, the authors concluded that Tg was a weak indicator of tumor necrosis (24). Embolization therapy did not appear to improve life expectancy, but this technique could achieve palliation of pain and dramatic relief of neurological symptoms (16,23,24,27). A new liquid embolic agent called Onyx® (ethylene vinyl alcohol copolymer dissolved in dimethyl sulfoxide, and suspended micronized tantalum powder to provide contrast for visualization under fluoroscopy; Micro Therapeutics, Inc, Irvine, CA) has been reported to achieve deep penetration into tumor lesions. Onyx has been used successfully in osseous metastases from TC, and it can produce extensive tumor infarction with the need for fewer arterial catheterizations (28).
Embolization may be useful in patients with spinal cord compression secondary to TC who cannot undergo surgery or in whom surgery was unsuccessful because of severe hemorrhage (23). In cases of imminent fracture of affected vertebrae, surgical stabilization can be performed after embolization.
Embolization is widely used to prepare selected patients for open surgery of the targeted metastatic lesions. Preoperative embolization greatly decreased intraoperative blood loss from 5500 to 1900 mL and was found to allow for more complete tumor resection (26). Demura et al. (29) used this technique before en bloc total spondylectomy in all 24 patients with SMs due to TC. Sakaura et al. (30) used preoperative embolization in a series of 12 patients including three with TC SMs. Preoperative embolization of hypervascular SMs can also be performed using percutaneous direct injection with n-butyl cyanoacrylate (31).
Selective embolization of SMs appears to be a safe, minimally invasive technique, which can be an attractive therapeutic option in selected patients with advanced TC. The post-embolization syndrome, which manifests with symptoms such as fever, pain, and malaise due to tumor necrosis, occurs relatively often after tumor embolization (18%–86% of cases) and may even be seen after selective embolization of a single metastatic lesion (27).
Pharmacological Therapy
Bisphosphonate therapy is the current standard of care for preventing skeletal complications associated with malignant bone disease (e.g., fractures, spinal cord compression, need for external beam radiotherapy, and hypercalcemia) (32). Bisphosphonates inhibit osteoclast-mediated bone resorption and have antitumor effects by inhibiting tumor cell proliferation, adhesion, and invasion, as well as inhibiting angiogenesis and inducing apoptosis (33). Another rationale for using bisphosphonates is to prevent the accelerated bone loss that may occur from increased bone resorption induced by suppressive doses of levothyroxine (LT4) therapy prescribed after TC surgery. Although men and premenopausal women with TC on suppressive doses of LT4 do not lose a significant amount of bone mass over 2 years (34), postmenopausal women on suppressive doses of LT4 may have an increased risk of vertebral fractures. Since patients with TC SMs may have a long survival from their disease, it is essential to consider the potential advantages and disadvantages (osteonecrosis of the jaw and atypical femoral shaft fractures) of treating these patients with many years of bisphosphonate therapy (32).
There are a few studies specifically employing intravenous bisphosphonates in the management of bone metastases from TC and none specifically focused on SM. In one small study, DTC patients who had been administered bisphosphonates showed a significant decrease in bone pain, improved performance status, and improved quality of life (35). Furthemore, zoledronic acid administration was associated with a significantly reduced number of skeletal related events (19). Nakada et al. (36) assessed incadronate and pamidronate treatment of 18 patients (57 bone lesions, including 19 in the spine) and showed a 50% reduction in the maximum standardized uptake value on [18F]-fluorodeoxyglucose positron emission tomography (FDG-PET) in 40% of patients with FDG-avid tumors and demonstrated improvement in bone pain in 61% of patients, with 33% of patients no longer requiring analgesic medications for pain. The appearance of areas of sclerosis in lytic bone metastases suggests that this treatment may delay disease progression and induce clinical remission of bone metastases (35). The optimal protocol of bisphosphonate therapy is not established yet. Wexler (32) recommended a 4 mg dose of zoledronic acid once a year for those without a pathological fracture to continue this as long as the lesions persist. However, for patients with acute pathological fractures, 4 mg of zoledronic acid every 3 months for the first year and then twice yearly was recommended (32).
Denosumab, a monoclonal antibody against receptor activator of nuclear factor-kappaB ligand (RANKL), has been shown to increase bone mass in osteoporosis and reduce tumor-induced osteolysis in experimental models of bone metastases (4). In patients with bone metastases from advanced solid tumors, denosumab was superior to the bisphosphonate zoledronic acid in preventing skeletal-related events (37). The American Thyroid Association and the National Comprehensive Cancer Network guidelines endorse consideration of antiresorptive therapy with either a bisphosphonate or denosumab in patients with bone metastases (4).
Tyrosine kinase inhibitors (TKIs) are a promising treatment option for patients with progressive, refractory TC (38 –40). However, based on the largest retrospective study evaluating TKI therapies outside of clinical trials, bone and pleural lesions were the most refractory sites to treatment (38). TC bone metastases were reported to be more susceptible to TKIs after radiation therapy (38,41). It seems that TKIs alone play a minor role in treatment of TC bone metastases.
Radiotherapy
Treatment with external beam radiation therapy (EBRT) is currently a standard of care for patients with localized bone pain. It often is considered a palliative intervention due to the relative radioresistance of TC (1,29,42). Moreover, it lacks the precision to deliver radiation to the spine near radiosensitive structures such as the spinal cord, which limits the treatment dose to a level that is far below the optimal therapeutic dose (43). Nevertheless, EBRT is widely used in clinical practice.
Spine Stereotactic Radiosurgery
Advances in radiotherapy, including three-dimensional localization and intensity modulation have resulted in the development of a new treatment paradigm called stereotactic body radiation therapy (SBRT), which provides a high degree of accuracy in achieving dose conformality, that delivers a therapeutic dose to the tumor while sparing normal tissue (e.g., spinal cord) (44,45). It is mostly used for patients without evidence of overt spinal instability, those with life expectancy more than 3 months, and without neurologic deficit resulting from bony compression of neural structures (46). SBRT can provide high rates of control for SMs. In nonthyroid SM, Chang et al. (47) reported radiological control in 90% of the patients at 6 months and in 80% at 12 months. Sheehan et al. (48) also reported decreased or stable tumor volume in 82% of the patients treated (mean of 12.7 months of follow-up). There are no studies devoted to the assessment of the efficiency of SBRT on thyroid SMs. SBRT in patients with solitary thyroid SMs can provide efficient local disease control (Gerszten, personal communication). SBRT can also be used as salvage treatment, after failure of previously irradiated epidural SMs or palliative treatment and local disease control in patients with advanced cancer (49,50). Moreover, in patients with SMs, SBRT can be applied after spinal surgery for decompression and stabilization (50).
Gerszten et al. (43) analyzed a cohort of 500 patients with SMs who underwent SBRT, including 11 patients with metastatic TC. Overall long-term pain improvement occurred in 86% and long-term tumor control was demonstrated in 90% of patients. SBRT was shown to be successful for treatment of single papillary thyroid SMs (44). However, SBRT was also found to be associated with a significant risk (20%) of vertebral compression fracture (51). Risk factors for the development of vertebral compression fractures included an age >55 years, a pre-existing fracture, and baseline pain. To avoid compression fractures, the patients who undergo spinal SBRT should be considered for prophylactic vertebral stabilization or augmentation procedures (51).
Vertebroplasty/Kyphoplasty
Patients with mechanical spine instability usually require a stabilization procedure (52). Percutaneous vertebroplasty (PV) is a minimally invasive, radiologically guided procedure in which bone cement (polymethylmethacrylate) is injected into structurally weakened vertebrae. Balloon kyphoplasy (BK) is modified PV where balloons are used to gently elevate the fractured vertebrae in an attempt to return it to the correct position. PV was introduced in 1984 by Deramond and Galibert for the treatment of an aggressive vertebral hemangioma and adopted to treat SMs by Weill et al. (53) in 1996. Vertebral stabilization and pain relief are the major benefits of PV and BK. Many authors report significant pain relief in up to 97% cancer patients after PV (54). According to recently published recommendations of the Spine Oncology Study Group, using percutaneous techniques (PV and embolization) in the treatment of metastatic spinal tumors is “strongly recommended” (55). A strong recommendation means that most, if not all clinicians would want to use the intervention, patients would almost all want it, and policy makers should consider reimbursing for it in most situations.
In the first series of 37 patients, Weill et al. (53) described two patients with advanced TC who underwent PV to palliate pain. Clear improvement was noted in both patients, and radiation therapy followed cement injection. Mont'Alverne et al. (56) reported a patient with SM due to TC within a group of patients with SMs from different primary tumors. Pain improvement was achieved in 80% patients and spine stability in 87.5%. Martin et al. (57) performed PV of C2 vertebra lesion due to TC via the transoral approach. Togao et al. (58) described a patient who suffered from progressive pain despite treatment with analgesic agents, EBRT, 131I therapy, and posterior fusion surgery, who achieved pain relief after PV. We have reported two patients with advanced follicular TC and medullary TC treated with palliative PV who experienced significant pain relief, reduction in analgesic requirements, and improvement in other symptoms. In one case, PV was combined with transpedicular fixation for additional stability of the weakened segment (59). Quan et al. (60) successfully used PV for local mechanical pain due to osteolytic TC metastases in the absence of significant spinal cord compression or spinal instability. In this series, one patient required subsequent open posterior spinal cord decompression.
Percutaneous injection of the cement is accompanied by exothermic polymerization of polymethyl methacrylate. The temperature of the composite reaches over 75°C, however, cytotoxic effect is limited to 3 mm around the cement (54). Thus, the antitumoral effect of the cement is insufficient, and specific tumor therapy (i.e., chemotherapy, radiotherapy, or thermoablation) should be given where appropriate (54). The site of the cement injection is a critical issue. Recent research shows that direct injection of the cement into a metastatic lesion may lead to tumor dissemination. Axelsen et al. (61), using a large animal cancer model, demonstrated tissue migration from the intratrabecular space of vertebral bodies to the lungs when performing PV. They suggested that a significant risk of exporting neoplastic disease exists if composite is injected directly into a metastatic lesion. Therefore, the technique of cement delivery to intact bone appears to be safer. Our group reported an approach injecting the cement into the vertebral body bone from the unaffected side to prevent further metastatic destruction of bone (59).
Cardoso et al. (62) described an enhancement of the PV technique using percutaneous curettage of SM and administering vertebral intracavitary bone cement radiolabeled with 153Sm-EDTMP. Three millicuries of 153Sm-EDTMP was mixed with bone cement and injected into the void created by the balloon tamp. The accuracy of targeted delivery of the 153Sm-EDTMP was confirmed by sequential total body scintigraphs within several hours of completion of the procedure. Another novel approach to delivering intraoperative radiotherapy during kyphoplasty involves the percutaneous puncture of the injured vertebral body and inserting a specially designed metallic sleeve to guide the electron drift tube of the miniature X-ray generator and allowing the radiation dose to be delivered to the center of the metastasis (26,63).
Percutaneous Spinal Tumor Ablation
Spinal tumor ablation is defined as the direct, focal application of chemical or physical therapies to a specific tumor site to achieve its destruction. During the past few decades, several percutaneous ablation techniques have emerged (54).
Local tumor radiofrequency ablation (RFA) is considered one method of achieving tumor control (54). It utilizes a high-frequency alternating current that is passed from a needle electrode into the surrounding tissue, resulting in frictional heating and necrosis. The primary goal of symptomatic pain relief is achieved through necrosis of the metastatic lesion and, in bone metastases, destruction of sensory nerve fibers in the periosteum and bone cortex induced by the elevated temperature induced by the RFA technique (64). RFA has been demonstrated to be safe, with a mortality rate of 0.3% and a major complication rate (such as infections, neural structures injury) of 2.2% (54). In the presence of an impending vertebral compression fracture, RFA should be combined with cement augmentation to provide mechanical stabilization. This technique is indicated for nonsurgical candidates, patients with painful SMs, especially for those who have rupture of the vertebral posterior wall with risk of tumor retropulsion after PV. Since RFA produces intratumoral cavitation with pressure reduction, once cavitation of the spinal lesion is accomplished, vertebral consolidation is achieved with subsequent cement injection (54).
Treatment methods can be employed to effectively complement each other to increase the effectiveness of treatment or decrease the complication rate. Hoffmann et al. (65) successfully used RFA and vertebroplasty within one session in the treatment of 22 patients with pain due to metastatic vertebral lesions including one patient with TC. Sandri et al. (64) reported another series of 11 patients including two with SM due to TC treated by combined RFA and kyphoplasty.
Several other ablation techniques can also be used to control SMs. Percutaneous ethanol injection is the simplest and cheapest method of percutaneous tumor ablation, causing tumor necrosis directly through cellular dehydration and indirectly through vascular thrombosis and tissue ischemia, leading to a reduction in pain and an improved quality of life for patients (66).
Cryoablation, a technique that utilizes uses extreme cold (lower than −20°C) to destroy tumor tissue, has gained new interest since the development of miniaturized 17-gauge gas-driven cryoprobes that can be used percutaneously under computed tomography or magnetic resonance monitoring. Recent studies report an interest in cryoablation for the palliative treatment of bone metastases with very promising results and few complications (54,67). A patient with ilium metastases due to medullary TC was reported among 13 others in whom cryoablation was applied to control pain. All patients reported a reduction in pain medications after the procedure (67).
Open Surgery
The role of surgery for metastatic spinal tumors is under significant revision. Old surgical techniques of decompression such as laminectomy with or without stabilization resulted in poor outcomes, leading many to believe that radiotherapy was the preferred option over surgery (68). However, recent data have shown that modern surgical techniques resulted in much better outcomes than radiotherapy alone, and that quality of life after surgery is often improved (68).
The first case of an total en bloc spondylectomy (TES) was published by Stener in 1971 in a case of chondrosarcoma (69). In 1980–1990 Tomita et al. (70,71) and Fidler (72) further standardized and popularized this technique for treatment of SMs. TES is a technique that enables wide or marginal resection of malignant lesions of the spine. Additional stabilizing posterior instrumentation is usually required. It is used primarily for patients with a solitary SM who are in good general health and have a long life expectancy. Complications may occur in up to 25% of patients, the most common being wound infection and intraoperative bleeding (73). Zettinig et al. (74) found that surgical resection of the bone metastasis is associated with improved survival. Patients who underwent TES had a better survival rate than those who underwent debulking surgery (29). Enkaoua et al. (75) analyzed 37 patients with metastatic TC and concluded that surgery to excise single metastases provided good results. Sakaura et al. (30) analyzed 12 patients with solitary metastasis to the spine who underwent TES, including three patients with TC. They found that local recurrences were common in patients with paraspinal extension.
In circumstances where the lesion cannot be completely resected, palliative surgery may be superior to nonsurgical treatment. Pittas et al. (2) analyzed a cohort of 146 patients with bone metastases and showed that, although statistical significance was not reached, there was a trend toward improved survival for those patients whose metastases had been removed compared to those patients who did not have surgery.
Palliative debulking surgery of thyroid SM is associated with a local recurrence rate of 57% compared to only a 10% local recurrence rate after TES (29). Abdel-Wanis et al. (76) found that the incidence of local recurrence after palliative surgery was 50%, a statistically significant increase as compared to the TES technique. Partial resection and vertebral body replacement with a ceramic prosthesis can be followed by local recurrence in as many as 46% of patients (77). Spinal stabilization techniques (i.e., transpeduncular rod fixation) are often required after tumor decompression is achieved. Several studies were done on bone metastases including lesions other than SMs. In patients without extraskeletal metastases, the radical surgical extirpation of bone metastases from DTC may be associated with improved survival. It also has been shown that surgical removal of up to five bone metastases was associated with improved survival and quality of life. Complete bone metastases surgery in young patients was found to be an independent prognostic factor associated with an improved survival (50,78).
Treatment Strategy
The evaluation of patients with SMs includes an assessment of pain, neurologic status, and general performance. Pain assessment can be most readily performed with a visual analog scale (0 to 10). The Frankel grading system is one of the most commonly used scales for functional assessment of the spinal cord (Table 1) (79,80). The Karnofsky performance status is widely used to measure the level of patient activity and medical care requirements in patient with SMs (48,81) (Table 2).
From Appendix I: Performance Status Scales (82).
In patients with solitary SMs and limited metastatic disease from TC, long survival may occur and therefore, advanced therapeutic options should be considered in the decision-making process (60,76). Several classification systems have been described in an attempt to promote the adoption of different surgical strategies. The recently published “Review of metastatic spine tumor classification and indications for surgery: the consensus statement of the Global Spine Tumor Study Group” proposed the use of Tomita's and Tokuhashi's staging systems in order to establish the optimal surgical strategy (68).
Tomita's system is based on three factors: the rate of growth of the primary tumor, number of bone metastases, and visceral metastases (70,71) (Table 3). The scores of these three components can be added together to produce a total score. According to this system patients with very good prognostic scores (2–3) should undergo wide excision, whereas patients with intermediate scores should undergo marginal or intralesional excision (scores 4–5) and palliative surgery (scores 6–7), while nonsurgical supportive care should be performed for the worst prognostic group (scores 8–10) (68,70,71). Solid organ metastasis is considered a poor prognostic factor for survival in patients with SMs due to TC. Additional nonskeletal organ involvement at the time of presentation of bone metastases was also a significant negative prognostic variable (2). Demura et al. (29) compared patients who underwent TES and found that 5-year survival rates in the patients without solid organ metastases were statistically better than those in patients with additional nonskeletal metastases. They found that multiple bone metastases also correlated with poor survival.
Tomita et al. (70,71).
Tokuhashi et al. (83) proposed another prognostic scoring system comprising six variables. Each variable was evaluated with a score from 0 to 5 points, giving a maximum total score of 15 (Table 4). Tokuhashi et al. recommended excisional surgery for patients with a good prognosis (Tokuhashi score of 12–15), palliative surgery for most patients with an intermediate prognosis (score of 9–11), and conservative management for patients with a score of 8 or less (68,83). Zeng et al. (84) reviewed 447 patients with SMs including patients with metastatic TC and found that the Tokuhashi scoring system could support decision making with reliable estimation of life expectancy of these patients, as well as being a valuable prognostic tool in thyroid SM (75).
Criteria of predicated prognosis: total score (TS) 0–8, <6 months; TS 9–11, ≥6 months; TS 12–15, ≥1 year. From Tokuhashi et al. (83).
A proposed assessment strategy of the patients with thyroid SMs based on metastatic spread and functional status utilizing the Tokahashi and Tomita scoring system, Karnofsky performance status and spinal metastatic spread is presented in Figure 1.
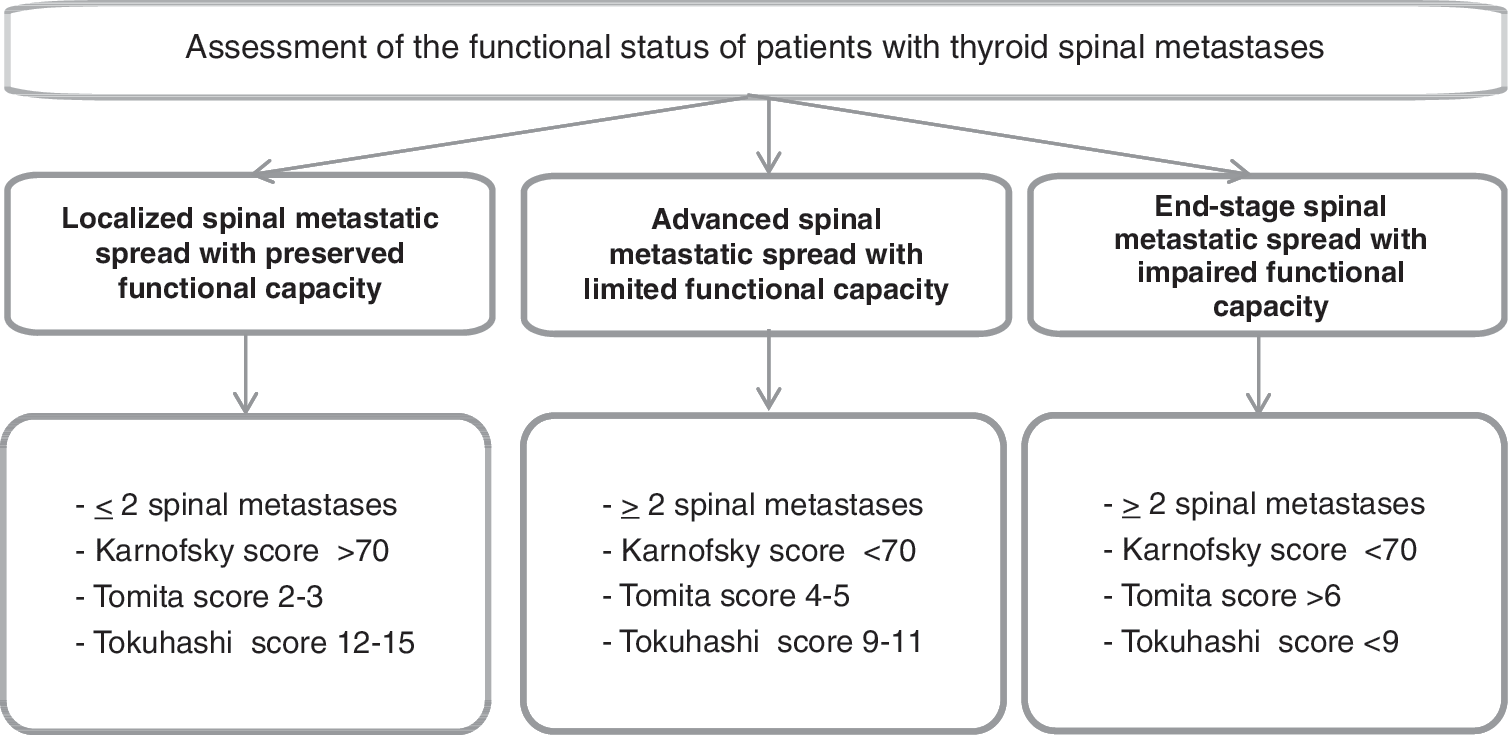
Proposed assessment strategy of the patients with thyroid spinal metastases (SMs) based on spreading metastases and functional status.
We propose a tiered approach to the treatment of SMs originating from TC (Table 5). Radioiodine is considered first line therapy to treat patients with metastatic disease. 131I can control not only the microscopic carcinoma in residual tissue, but also small bone metastases. However, large SMs are generally resistant to 131I treatment. In patients without spinal cord compression or without risk of imminent compression fracture, 131I is usually considered as initial therapy (as a part of post-thyroidectomy radioablation or treatment other thyroid metastases) and surgery is usually reserved for patients refractory to 131I treatment (1,30). Some recommended to add postoperative radioiodine treatment after surgical excision of bone metastases (85) because total vertebrectomy may increase the efficacy of 131I therapy for thyroid bone metastasis (86,87). If the SM cannot be cured with radioiodine, or if the response is incomplete, second line methods such as TES or radiosurgery (with or without vertebral stabilization technique) should be considered. For patients presenting with symptoms from SM due to TC, prompt surgical decompression and stabilization of the involved spinal segments followed by total thyroidectomy and radioactive iodine to the primary and metastatic sites is preferable (52). There has been a lack of publications in support of surgical resection of SMs or SMs radiosurgery prior to 131I treatment.
Radiosurgery and TES for single-site metastatic lesions are potentially radical treatments of SMs and aim at complete removal/destruction of metastatic tumor tissue with the intention to improve survival. Radiosurgery can be used in patients without neurological deficits or compression fractures, while TES can be performed in the complicated cases in patients with spinal cord compression, extravertebral extension of the tumor, or for those patients who are at risk of those complications.
The third line of therapy includes methods of mechanical stabilization of the diseased vertebral body and as well as methods to control tumor growth. Mechanical stabilization can be achieved by using open palliative surgery (e.g., transpedicular stabilization) or percutaneous techniques including PV and BK. Partial surgical removal of the tumor, embolization external beam radiation and methods of percutaneous ablation can be used to control tumor growth. Finally, all patients with bone metastases should be considered for treatment with zoledronic acid or denosumab in order to decrease the likelihood of developing a skeletal-related events from the osseous metastases. Optimal management of the patients with thyroid SMs depends on the location and vertebral stability and the entire clinical context. Thyroid SMs may present as the initial presentation of TC, and occurs approximately in one third of cases (Kushchayeva, unpublished data) or SMs after TC diagnosis that take place in approximately two thirds of cases (Kushchayeva, unpublished data). According to the time interval from TC diagnosis to detection of SMs, metastases were classified into two types: synchronous and metachronous. Synchronous metastases that were identified at the time of the TC presentation or within 6 months after its diagnosis, were found in 30% of all TC patients. Metachronous metastases, defined as metastases that developed more than 6 months after diagnosis, were diagnosed in 35% of all TC patients (Kushchayeva, unpublished data) (Fig. 2). Treatment algorithms for managing SMs in these clinical groups are depicted in Figures 3, 4, and 5.
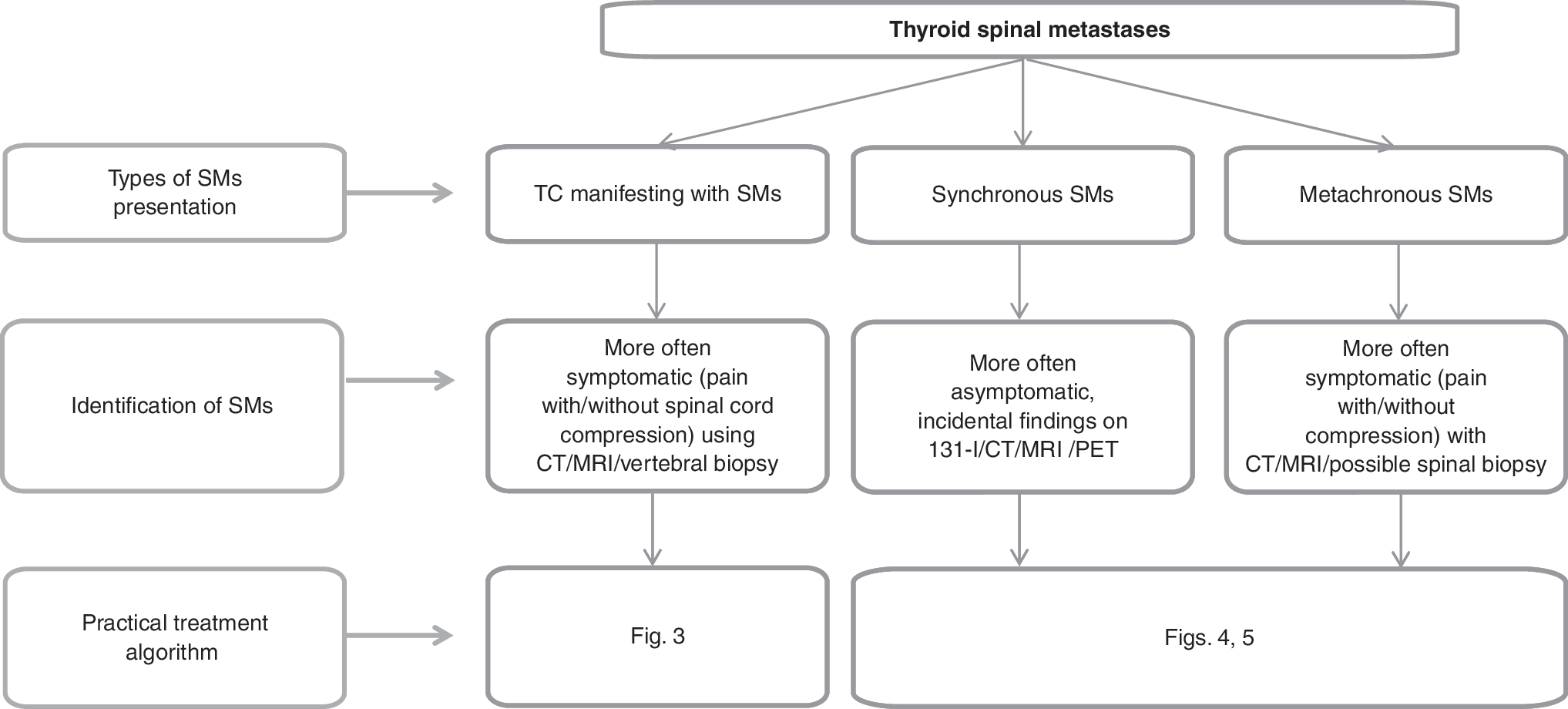
Types of clinical presentation of thyroid spinal metastases. CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography.
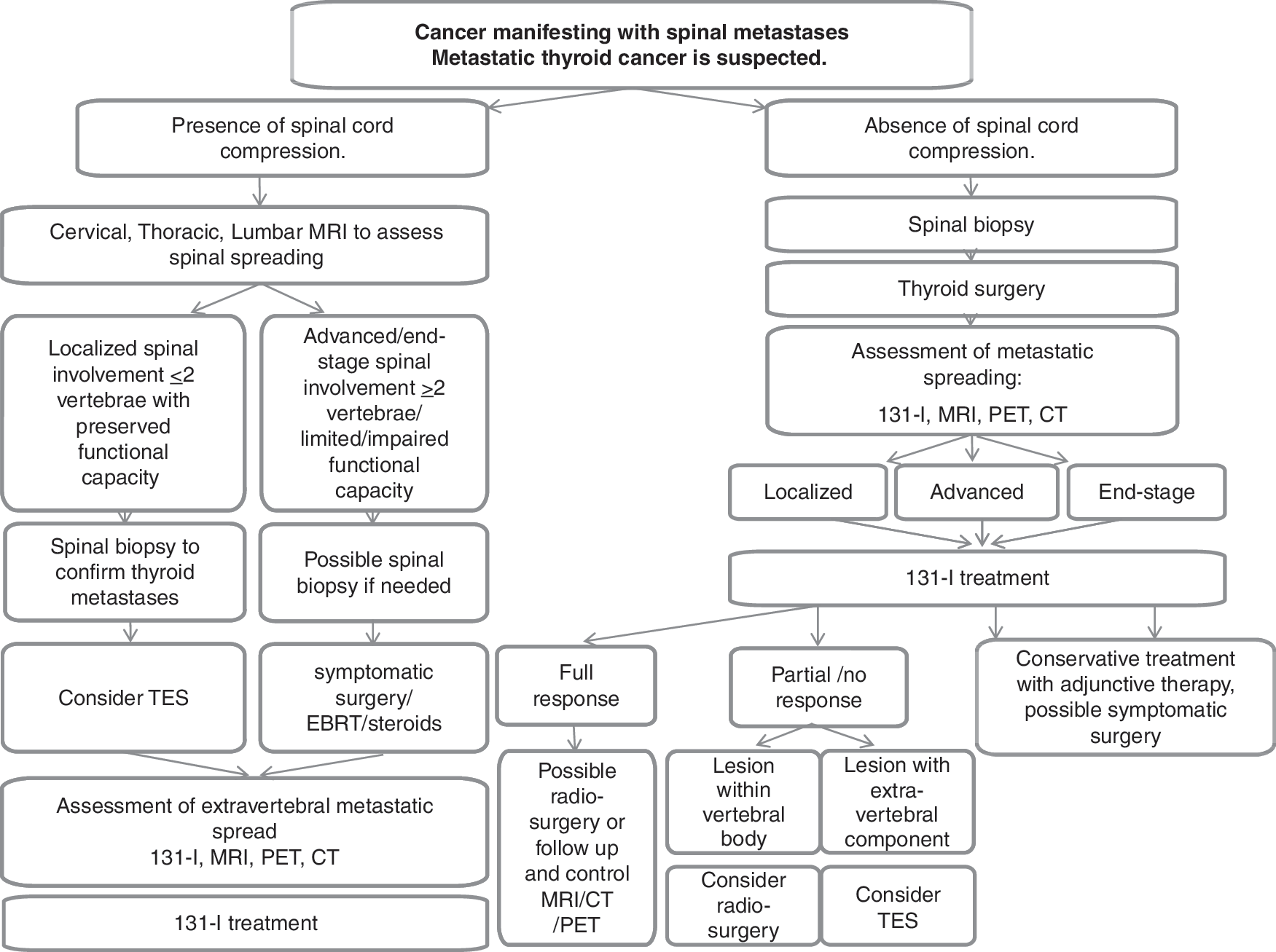
A proposed algorithm for managing spinal metastases presenting as the initial manifestation of carcinoma with suspected thyroid cancer origin. TES, total en bloc spondylectomy.
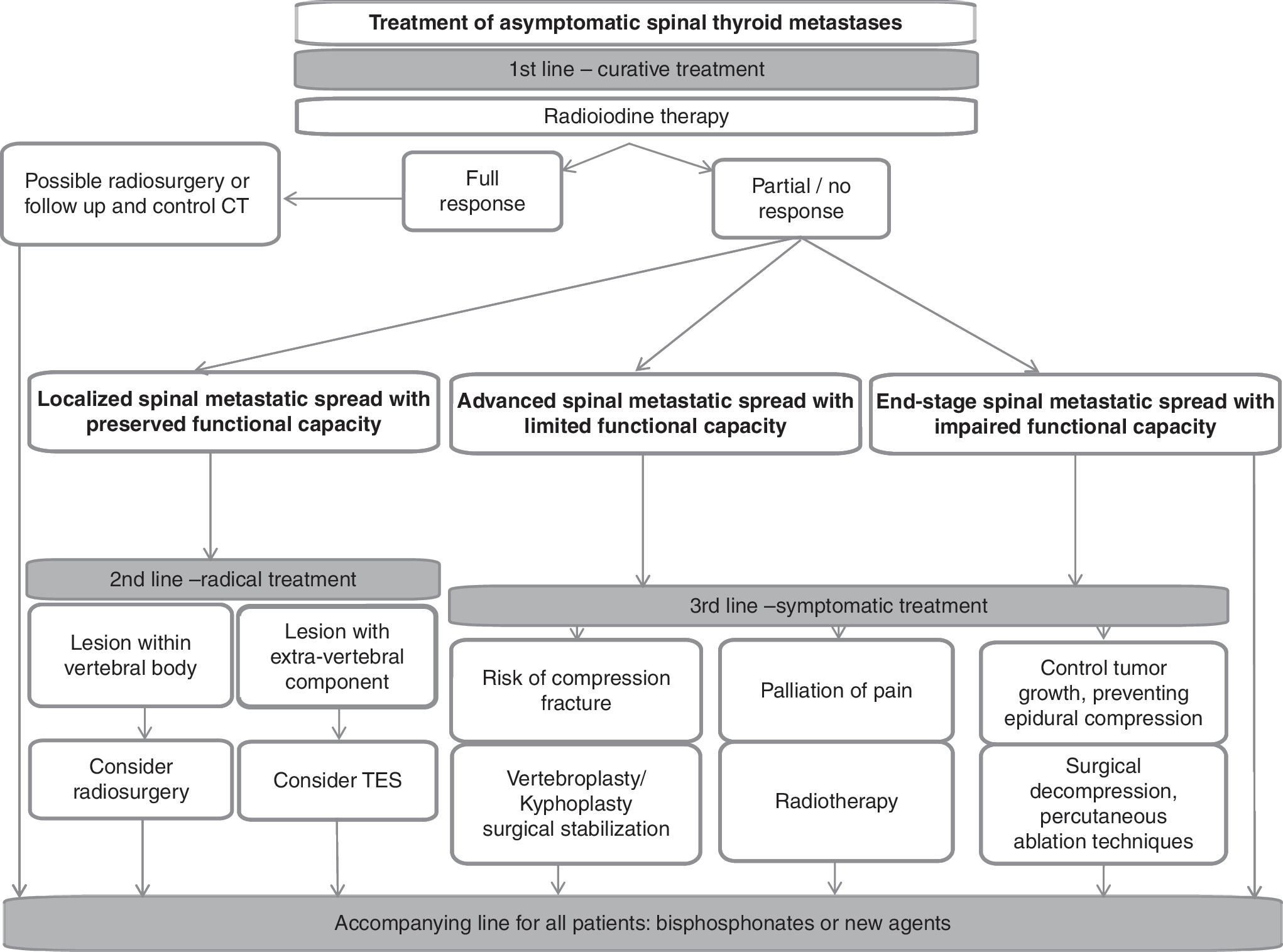
A proposed algorithm for managing patients with asymptomatic thyroid spinal metastases.
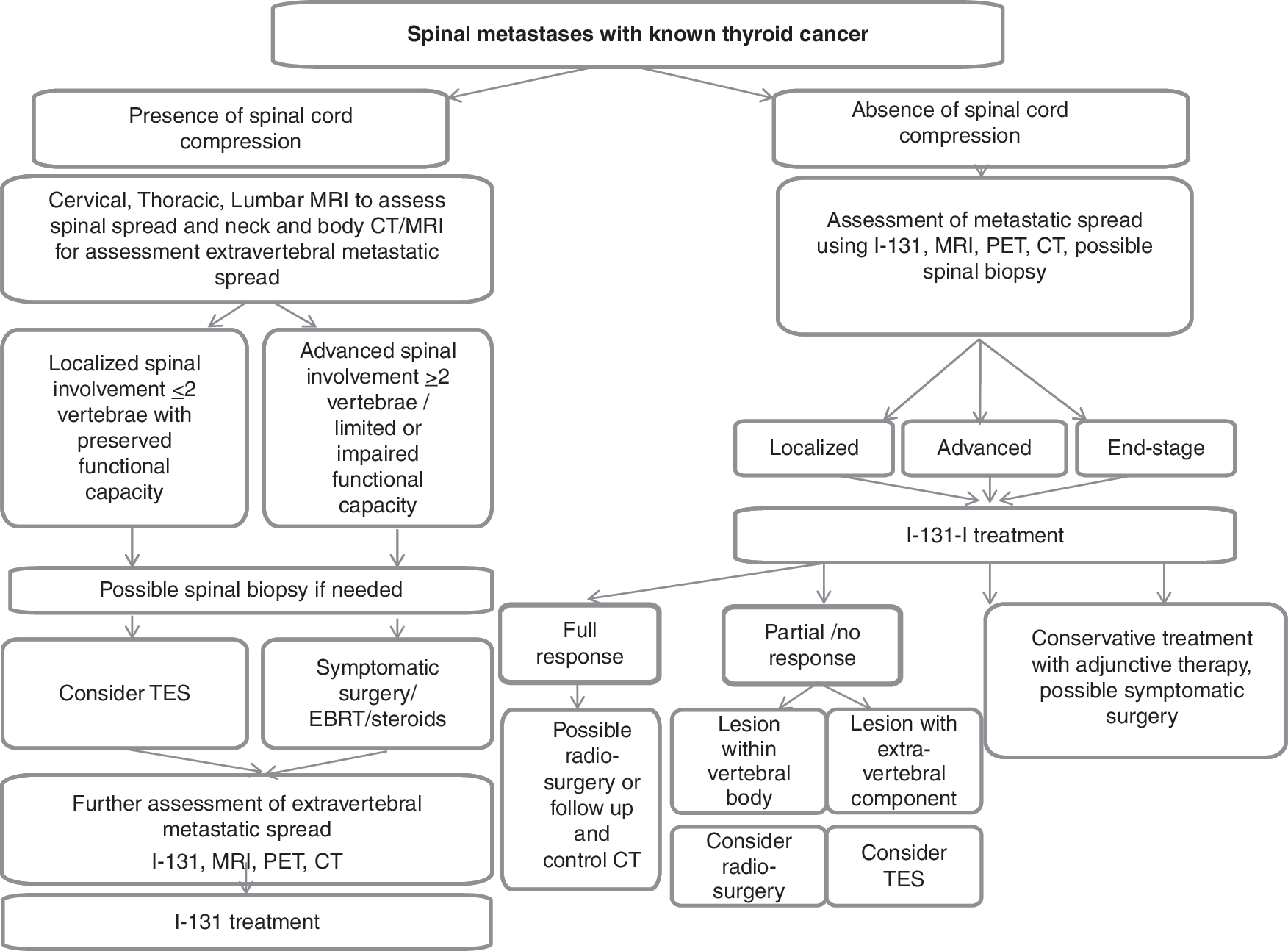
A proposed algorithm for managing spinal metastases in patients with known thyroid cancer. EBRT, external beam radiation therapy.
Saillant et al. (86) advocate the most aggressive therapeutic approach possible for vertebral metastases from thyroidal origin when it is feasible and appropriate to do so. Spine surgeons play a leading role in the management of these patients. However, many cancer centers do not employ a multidisciplinary approach for patients with newly diagnosed metastatic spinal disease. Instead, the majority of patients are sent directly to radiation oncology for conventional external therapy (88).
Conclusion
The introduction of novel and improved techniques for the treatment of SMs (such as radiosurgery and minimally invasive percutaneous techniques) has created the opportunity to significantly improve control of metastatic tumor growth and the quality of life for patients bone metastases from TC. We proposed a three-tiered approach to the management and practical algorithms for patients with SMs from TC.
In order to effectively use modern treatment options, a multidisciplinary approach must be used in the management of the patients with SMs due to TC, involving endocrinologists, nuclear medicine physicians, radiologists, interventional radiologists, radiation oncologists, medical oncologists, neurosurgeons, orthopedic oncologists, and other relevant health care professionals (e.g., nurses, social work) in the decision-making process.
Footnotes
Author Disclosure Statement
No competing financial interests exist.